Embed Size (px)
Citation preview

Granuloma Inguinale,
Lymphogranuloma Venereum,
Gonorrhea
082012100062
Nur Hanisah Zainoren
Objective
To understand the underlying causes of the
diseases
To understand the clinical findings of the
diseases
To know and memorize the drug used for the
treatment of the diseases

Pathology of the Diseases
Granuloma Inguinale
Chronic, relapsing granulomatous anogenital
infection
Due to: Calymmatobacterium granulomatis
Lesion occur on the skin or mucous membranes of
the genitalia or perineal area
Painless infiltrated nodules that soon slough.
A shallow, sharply demarcated ulcer forms, with a
beefy-red friable base of granulation tissue.

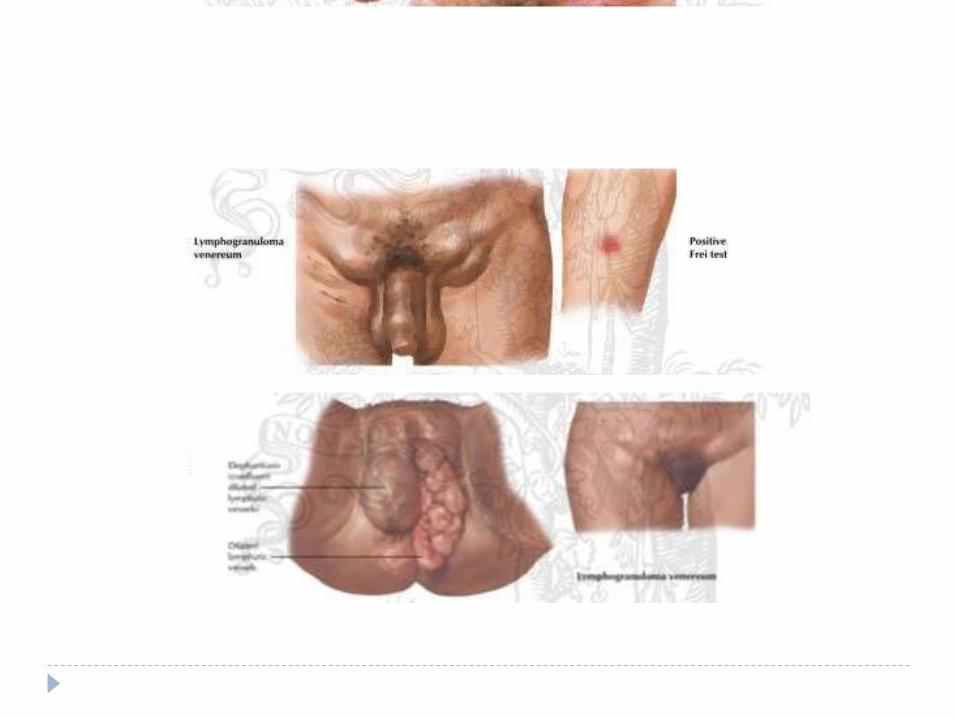
Lymphogranuloma Venereum
LGV is an acute and chronic sexually transmitted
disease caused by Chlamydia trachomatis types
L1-L3
Disease is acquired during intercourse or through
contact with contaminated exudate from active
lesions.
After the genital lesions disappears, the infection
spreads to lymph channels and lymph nodes of
genital and rectal areas.
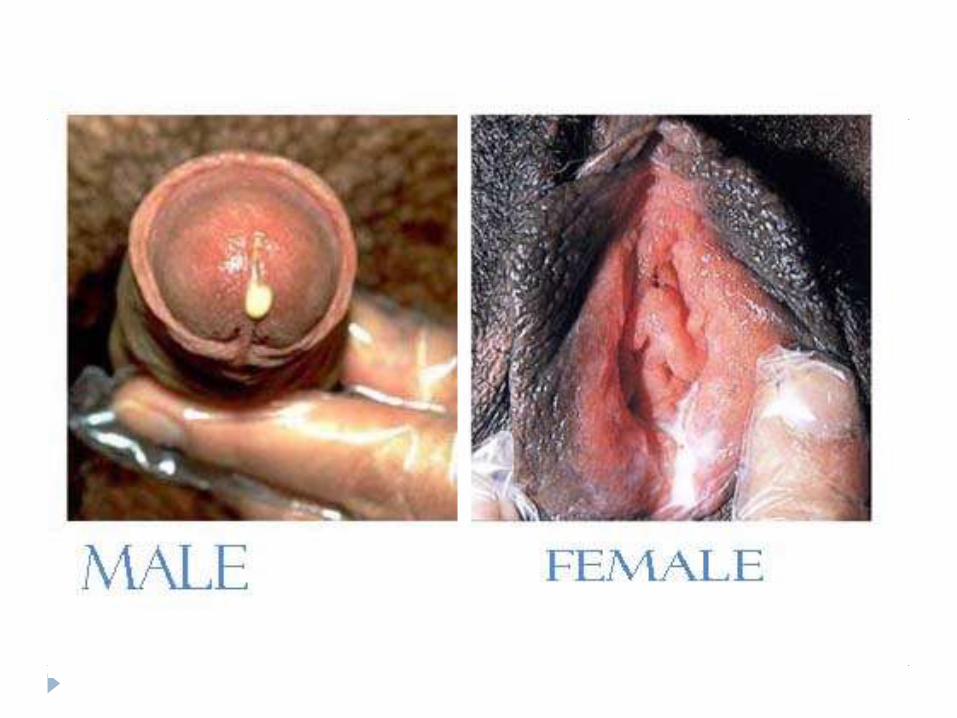
Gonorrhea
Caused by: Neisseria Gonorrrhoeae
Transmitted during sexual activity and has greater
incidence in the 15-29-year-old age group.
Characterized by thick discharge from the penis
and vagina.
In addition to male reproductive organs & female
genital tract, gonorrhea may infect the rectum,
throat, eyes, blood, skin & joints.
Pharmacotherapy of the
Diseases
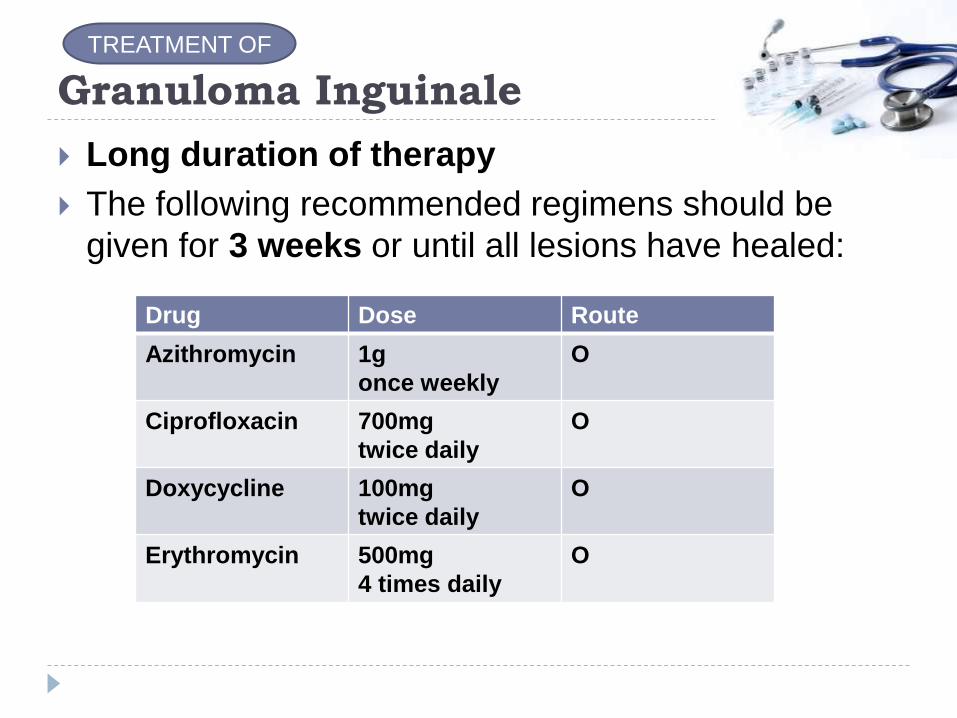
Granuloma Inguinale
Long duration of therapy
The following recommended regimens should be
given for 3 weeks or until all lesions have healed:
Drug Dose Route
Azithromycin 1g
once weekly
O
Ciprofloxacin 700mg
twice daily
O
Doxycycline 100mg
twice daily
O
Erythromycin 500mg
4 times daily
O
TREATMENT OF
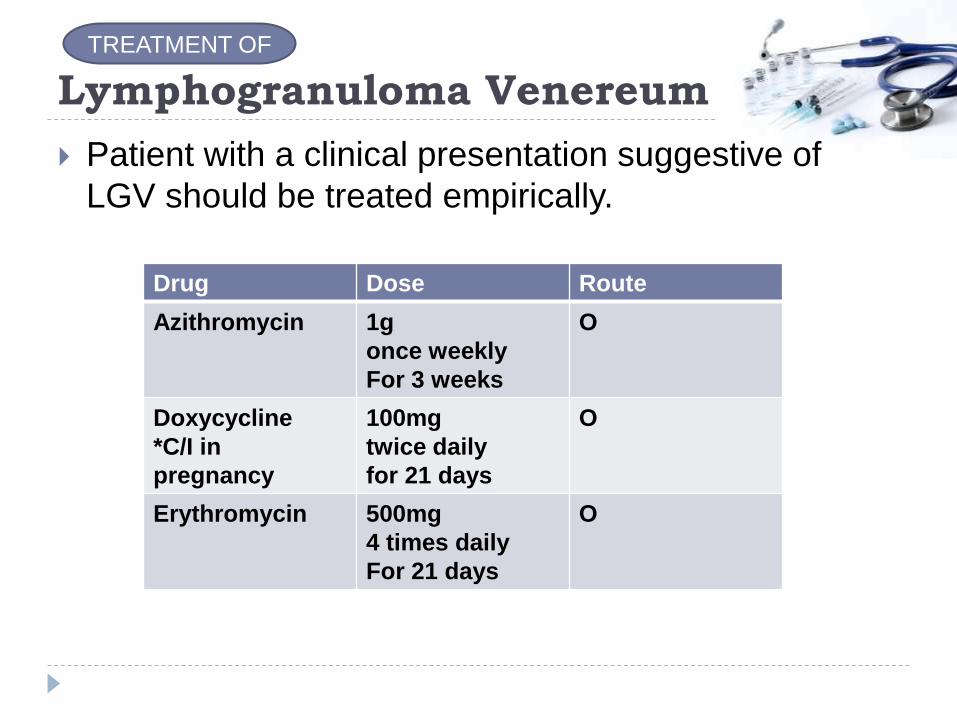
Lymphogranuloma Venereum
Patient with a clinical presentation suggestive of
LGV should be treated empirically.
Drug Dose Route
Azithromycin 1g
once weekly
For 3 weeks
O
Doxycycline
*C/I in
pregnancy
100mg
twice daily
for 21 days
O
Erythromycin 500mg
4 times daily
For 21 days
O
TREATMENT OF
Gonorrhea
The choice of which regimen to use should be based on the national prevalences of antibiotic resistant organisms.
Nationwide, strains of gonococci that are resistant to penicillin, tetracycline, or ciprofloxacin have been increasingly observed.
Hence no longer be considered as 1st line therapy
Treatment of: 1. Uncomplicated Gonorrhea
2. Disseminated gonococcal infection
3. Endocarditis
4. Postgonococcal urethritis and cervicitis
5. Pelvic inflammatory disease
TREATMENT OF

Gonorrhea
1. Uncomplicated Gonorrhea
Higher dose of IM Ceftriaxone in combination with
second drug (Azithromycin or Doxycyline)
regardless of concern for possible secondary infection
with chlamydia.
For uncomplicated gonococcal infection of the cervix,
urethra, and rectum and pharyngeal gonorrhea
Ceftriaxone (250mg IM) + Azithromycin (1000mg orally as
SD) / Doxycycline (100mg BD for 7 days)
TREATMENT OF
*In case where an oral cephalosporin is the only option,
Cefixime (400mg, O, SD) can be combined with
Azithromycin/Doxycycline as above
but a “test of cure” is recommended 1 week after treatment
Gonorrhea
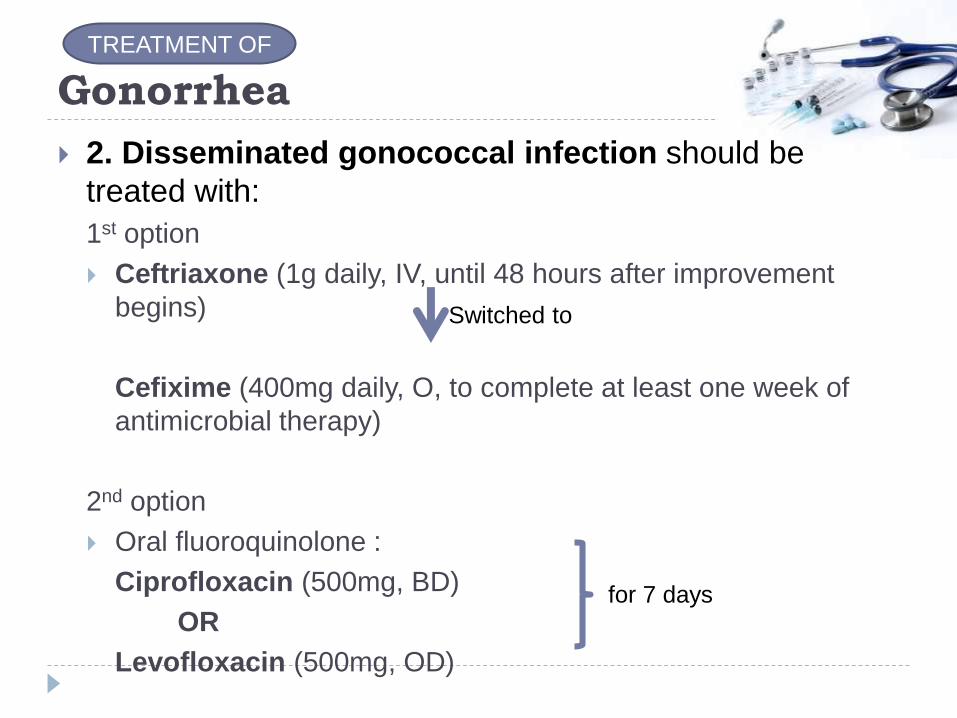
2. Disseminated gonococcal infection should be
treated with:
1st option
Ceftriaxone (1g daily, IV, until 48 hours after improvement
begins)
Cefixime (400mg daily, O, to complete at least one week of
antimicrobial therapy)
2nd option
Oral fluoroquinolone :
Ciprofloxacin (500mg, BD)
OR
Levofloxacin (500mg, OD)
Switched to
for 7 days
TREATMENT OF
Gonorrhea
3. Endocarditis should be treated with: Ceftriaxone ( 2g every 24 hours, IV, for at least 3 weeks)
4. Postgonococcal urethritis and cervicitis are treated with a regimen of erythromycin, doxycycline or azithromycin
5. Pelvic inflammatory disease:
1st option Cefoxitin (2g parenterally every 6 hours) OR
Cefotetan (2g IV every 12 hours)
Doxycycline (100mg every 12 hours)
TREATMENT OF
Gonorrhea
Pelvic inflammatory disease:
2nd option
Clindamycin (900mg, IV every 8 hours)
Gentamicin ( IV as a 2mg/kg loading dose followed by
1.5 mg/kg every 8 hours)
3rd option
Ceftriaxone (250mg IM, SD) OR
[Cefoxitin (2g IM, SD) + Probenecid (1g orally as a
SD)]
Doxycycline (100mg BD for 14 days)
With or without Metronidazole (500mg, BD for 14 days)
TREATMENT OF
Conclusion
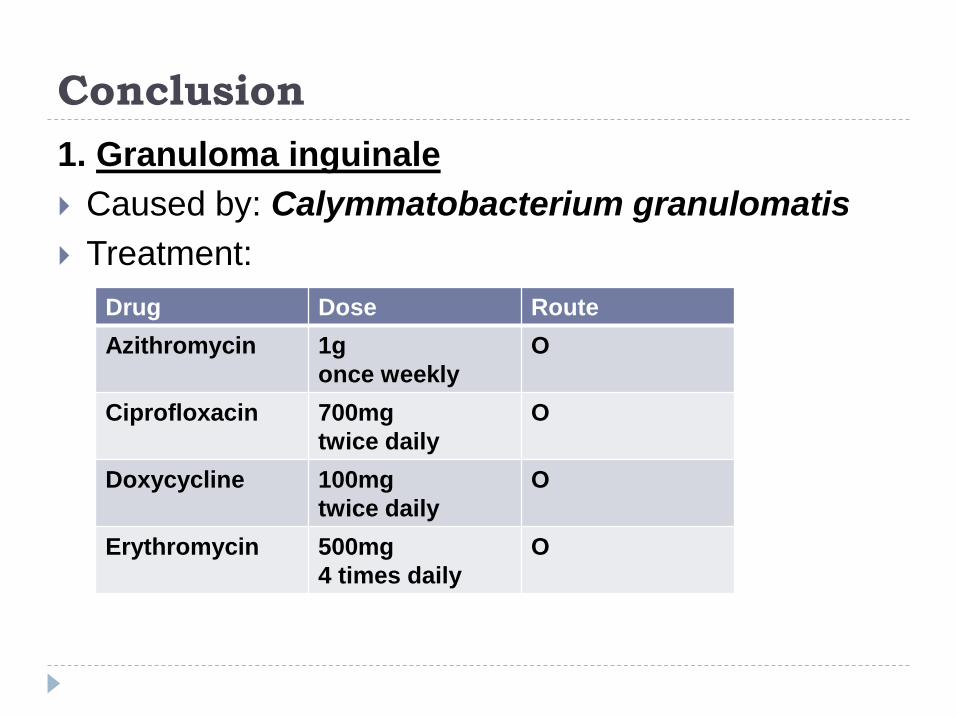
1. Granuloma inguinale
Caused by: Calymmatobacterium granulomatis
Treatment:
Drug Dose Route
Azithromycin 1g
once weekly
O
Ciprofloxacin 700mg
twice daily
O
Doxycycline 100mg
twice daily
O
Erythromycin 500mg
4 times daily
O

2. Lymphogranuloma Venereum:
Caused by: Chlamydia trachomatis types L1-L3
Treatment:
Drug Dose Route
Azithromycin 1g
once weekly
For 3 weeks
O
Doxycycline
*C/I in pregnancy
100mg
twice daily
for 21 days
O
Erythromycin 500mg
4 times daily
For 21 days
O

3. Gonorrhea
Caused by: Neisseria Gonorrrhoeae
Treatment:
1.Uncomplicated Gonorrhea-Ceftriaxone/Cefixime+Azithromycin/Doxycycline
2.Disseminated gonococcal infection-CeftriaxoneCefixime or
-Oral fluoroquinolones (Ciprofloxacin/Levofloxacin)
3.Endocarditis
-Ceftriaxone
4.Postgonococcal urethritis and cervicitis
-Erythromycin, Doxycycline or Azithromycin
5.Pelvic inflammatory disease-Cefoxitin/Cefotetan+Doxycycline
-Clindamycin+Gentamicin
- Ceftriaxone OR [Cefoxitin + Probenecid] + Doxycycline
With or without Metronidazole
Reference
Stephen J.McPhee, Macine A.Papakadis, Current
Medical Diagnosis and Treatment, McGrawHill.
Thank you