Embed Size (px)
Citation preview

BYSROTA DAWN.
1 S T YEARM.PHARM(PHARMACOLOGY)
GOUT & ITS TREATMENT

INTRODUCTION
‘Gout’ is a metabolic disorder characterized by
hyperuricemia .
Hyperuricemia is a condition when blood SERUM URIC ACID
LEVEL gets increased.
Uric acid is the end product of purine metabolism

NORMAL PLASMA URIC ACID CONCENTRATIONS
In men 3-7 mg/dl
In women 2-6mg/dl
Daily excretion of uric acid is about 500 – 700 mg.
The prevalence of gout is about 3 per 1,000 persons .
mostly affecting males & post-menopausal women however , are as susceptible as man for this disease.

Gout is a metabolic disease associated with over production of uric acid. Biologically it is synthesized
during purine metabolism,Uric acid has
1. Low water solubility.2 . Especially in low pH
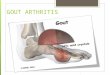
When blood levels are high ,it precipitates and deposit as sodium urate crystals on joints, kidneys and subcutaneous tissue( tophy )

Gout: pathophysiology
Food intake Cell breakdown
Purines
Uric acid
HYPERURICAEMIA
Kidney
Soft tissue of the joints
Other tissue Ear
Overproduction Under excretion



• FACTORS INFLUENCING GOUT FORMATION:
1. HIGH LIVING
2. OVER EATING
3. ALCOHOL CONSUMPTION
4. LEAD POISONING

Gout is of two types –
1. Primary gout2. Secondary gout
1. Primary gout :
it is an inborn error of metabolism of purine due to over production of uric acid. This is mostly related to increased synthesis of purine nucleotides.
2. Secondary gout :
secondary hyperuricemia is due to various disease causing increased synthesis or decreased excretion of uric acid.

DISORDERS OF PURINE METABOLISM (URIC ACID SYNTHESIS PATHWAY)


The important metabolic defects are associated with primary gout formation :
ENZYMES DIRECTLY INVOLVED IN PURINE SYNTHESIS:
1. PRPP SYNTHATASE : In normal circumstances , PRPP
synthetase is under feed back control mechanism by purine nucleotides (ADP and GDP ).This leads to the increased production of purines .
2. PRPP glutamylamidotransferase :The lack of feedback control of
this enzyme by purine nucleotides also leads to their elevated synthesis .
3. HGPRT deficiency :This is an enzyme of purine
Salvage pathway , and its defects causes lesch – Nyhan syndrome.

Lesch – Nyhan syndrome.
This disorder occurs with increased synthesis of purine nucleotides by 2 fold mechanism
Decrease utilization of Purine nucleotides ( hypoxanthine & guanine)
The defect in salvage pathway, leads to IMP & GMP

ENZYMES INDIRECTLY INVOLVED IN PURINE SYNTHESIS:
4 . GLUCOSE 6 – PHOSPHATASE DEFFICIENCY : In von Gierke’s
disease, glucose 6-phosphate can not be converted to glucose due to the deficiency of glucose 6- phosphatase. This leads to increased utilization of glucose 6- phosphate by HMP shunt ,resulting in elevated levels of ribose 5- phosphate and PRPP and ultimately leads to purine overproduction.
5.ELIVATION OF GLUTATHIONE REDUCTASE : Increase glutathione
reductase generates more NADP+ which is utilized by HMP shunt. This leads to elevated levels of ribose 5- phosphate and PRPP and ultimately leads to purine overproduction.

PATHWAY OF FORMATION OF GOUT:
1.Precipitation of uric acid crystals on synovial fluid
2. Inflammatory response, chomotactic factors produced
3.Granulocyte migration into the joint, they phagocytose urate crystals and release a glycoprotein which aggregates the inflammation by
4.Increasing lactic acid production from inflammatory cells

PATHWAY OF FORMATION OF GOUT:
5.local PH reduced
2. more uric acid crystals precipitates in the affected joint .
3. Release lysozomal enzymes which causes joint destruction.

How is Gout Cured?
No cureGout can be controlled
Diet – eating low purine foods, drinking water
Drugs – Allopurinal lowers uric acid production

Therapy for Acute Gouty Arthritis
Colchicine Oral IV
Nonsteroidal Anti-inflammatory AgentsCorticosteroids
Intra-articular IM (ACTH)

Colchicine : BIOLOGICAL SOURCE : Colchicum autumnale
neither analgesic nor anti – inflammatory but suppress the gouty inflammation does not inhibit the synthesis of uric acid does not promote the excretion of uric acid thus has no effect on blood uric acid levels
Colchicine inhibits release of the glycoprotein and their by inhibit the following pathway.
TOXICITY: Dose related.ADR: 1. Nausea ,vomiting, watery or bloody diarrhoea and abdominal cramps. 2.overdose leads to kidney damage.3.Chronic therapy with colchichine is not recommended because it causes aplastic anaemia,agranulocytosis,myopathy and loss of hair.

Nonsteroidal Anti-inflammatory Agents : Strong NSAID s used :
indomethacine , naproxen , piroxicam, diclofenac, etoricoxib
strong anti-inflammatory action
naproxen and piroxicam inhibits chemotactic migration of leucocytes into the inflamed joint.
they are not recommended for long term therapy

Corticosteroids :
intraarticular injection of a soluble steroid suppresses symptoms of acute gout.
they are very effective and produce nearly as rapid a response as colchicine
but are reserved for the patients of renal failure history of peptic ulcer bleed in whom NSAID s are
contraindicated. Inhibit PGE2 and LTB4 Stabilize lysosomal membranes

Therapy for Acute Gouty Arthritis
When pain and stiffness persist in a joint between attacks, gout has become chronic .
Other features are : 1.Hyperuricaemia
2. tophy 3. urate stones in the kidney
Two types of drugs are used in this type of chronic gout: uricosuric drugs : 1 . PROBENECID 2 . SULFINPYRAZONE uric acid synthesis inhibitors : ALLOPURINOL






Probenecid/Sulfinpyrazone
No analgesic/anti-inflammatory activity.Inhibits uric acid reabsorption.Plenty of water /fluids should be given with
probenecid to avoid urate crystallization in urinary tract
Increase uric acid excretion in urine.Uses: Chronic gout and hyperuricemiaAdverse effects: Hypersensitivity

Allopurinol
No analgesic/anti-inflammatory activity.Reduces plasma, tissue and urine
concentration of uric acid.Reverses of deposition of urate crystals
and inhibits urate stone formation.

Drugs used in chronic gout (antihyperuricemic drugs) : sites of action
Purines
Hypoxanthine
Xanthine
Uric acid
Xanthine oxidase
Xanthine oxidase
PROBENECIDSULPFINPYRAZO
NE
-
OXYPURINOL
--
Overproducers: Allopurinol
Underexcretors: Probenecid
Sulfinpyrazome
ALLOPURINOL
-

Allopurinol
Uses: Chronic gout
Tophi Nephropathy
Secondary gout Cancer
radio/chemotherapy (coadministered with
azathioprine/mercaptopurine)

Allopurinol
Drug interactions: Azathioprine,
mercaptopurine(inhibits degradation) Probenecid(complex
interaction) Warfarin,theophyline(inhibit
metabolism) Ampicillin(skin rashes)
Xanthine oxidase
Azathioprine
Mercaptopurine
Inactive metabolites
Allopurinol
-
• Adverse effects:– Hypersensitivit
y

Thank you