Embed Size (px)
Citation preview

Review
Glucose metabolism in burn patients: The role of insulin andother endocrine hormones
Nikiforos Ballian a, Atoosa Rabiee b,c, DanaK. Andersen b, Dariush Elahi b,c,*, B. Robert Gibson b
aDepartment of Surgery, University of Wisconsin, Madison, WI, United StatesbDepartment of Surgery, Johns Hopkins University School of Medicine, Johns Hopkins Bayview Medical Center, Baltimore, MD, United StatescDepartment of Medicine, Johns Hopkins University School of Medicine, Johns Hopkins Bayview Medical Center, Baltimore, MD, United States
Contents
1. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 600
2. Glucose metabolism in burn patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 600
2.1. Gluconeogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 600
2.2. Insulin resistance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 601
3. Deleterious effects of hyperglycemia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 601
4. Pharmacological agents and burn-related metabolic abnormalities. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 601
4.1. Insulin therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 601
4.2. Metformin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 603
4.3. Other agents . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 603
b u r n s 3 6 ( 2 0 1 0 ) 5 9 9 – 6 0 5
a r t i c l e i n f o
Article history:
Accepted 11 November 2009
Keywords:
Insulin
GLP-1
Burn ICU
Glycemic control
a b s t r a c t
Severe burn causes a catabolic response with profound effects on glucose and muscle
protein metabolism. This response is characterized by hyperglycemia and loss of muscle
mass, both of which have been associated with significantly increased morbidity and
mortality. In critically ill surgical patients, obtaining tight glycemic control with intensive
insulin therapy was shown to reduce morbidity and mortality and has increasingly become
the standard of care. In addition to its well-known anti-hyperglycemic action and reduc-
tion in infections, insulin promotes muscle anabolism and regulates the systemic inflam-
matory response. Despite a demonstrated benefit of insulin administration on the
maintenance of skeletal muscle mass, it is unknown if this effect translates to improved
clinical outcomes in the thermally injured. Further, insulin therapy has the potential to
cause hypoglycemia and requires frequent monitoring of blood glucose levels. A better
understanding of the clinical benefit associated with tight glycemic control in the burned
patient, as well as newer strategies to achieve and maintain that control, may provide
improved methods to reduce the clinical morbidity and mortality in the thermally injured
patient.
# 2009 Elsevier Ltd and ISBI. All rights reserved.
* Corresponding author at: Department of Surgery, Johns Hopkins University School of Medicine, Johns Hopkins Bayview Medical Center,4940 Eastern Avenue, A5, Baltimore, MD 21224, United States. Tel.: +1 410 550 2385; fax: +1 410 550 1895.
avai lab le at www.sc iencedi rect .com
journal homepage: www.elsevier.com/locate/burns
E-mail address: [email protected] (D. Elahi).
0305-4179/$36.00 # 2009 Elsevier Ltd and ISBI. All rights reserved.doi:10.1016/j.burns.2009.11.008

5. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 603
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 603
b u r n s 3 6 ( 2 0 1 0 ) 5 9 9 – 6 0 5600
1. Introduction
Despite advances in the resuscitation and surgical treatment
of burn patients, metabolic dysfunction remains a significant
cause of morbidity and mortality [1]. Significant thermal injury
is characterized by hypermetabolism and catabolism propor-
tional to burn surface area. This metabolic profile includes
changes in glucose homeostasis and muscle protein metabo-
lism that persist from the first few days following injury to as
long as three years later [2]. Healing of burn wounds is an
anabolic process which consumes massive amounts of amino
acids, supplied by breakdown of skeletal muscle [3–5].
Hyperglycemia and loss of muscle mass that are attendant
with catabolism have a central role in determining the
prognosis of these patients [1].
Insulin therapy has been shown to reduce mortality and
morbidity in surgical patients [6] and has both anti-hyperglyce-
mic and anabolic effects in muscle. Although the role of insulin
in maintaining muscle mass after burn has been investigated
[6,7], the potential influence on mortality is unknown. Since
patients with significant burns have the most intense and
prolonged catabolic response of all ‘surgical’ ICU patients, one
might conclude that the most robust clinical benefit of insulin
treatment in terms of a potential reduction in morbidity and
mortality may beobtained inthe burn population. Inthis review,
we present an overview of glucose regulation after burn injury
and describe the role of insulin and other endocrine hormones
in improving glycemic control and reversing catabolism.
2. Glucose metabolism in burn patients
Glucose metabolism is altered after significant burn, leading to
hyperglycemia [8,9]. Numerous mediators are involved in
Table 1 – Endocrine mediators of glucose regulation in burn p
Mediator Levels Direct effects
Insulin " # Gluconeogenesis
# Glycogenolysis
Glucagon " " Gluconeogenesis
" Glycogenolysis
# Glycogenesis
Catecholamines " " Gluconeogenesis
" Glycogenolysis
Impaired glucose transp
Corticosteroids " " Gluconeogenesis
TNF " Altered insulin signalin
IL-6 " Altered insulin signalin
MCP-1 " Altered insulin signalin
Growth hormone " Improved glucose dispo
# Gluconeogenesis
IGF-1 – Improved glucose dispo
TNF, tumor necrosis factor; IL, interleukin; MCP, monocyte chemotactic
regulating glucose metabolism and have complex effects
(Table 1).The maincontributors to burn-inducedhyperglycemia
are increased gluconeogenesis and insulin resistance [9–11].
2.1. Gluconeogenesis
Enhanced gluconeogenesis primarily occurs in the liver and its
purpose is to increase energy supply to the wound. Gluconeo-
genesis accounts for 11% of increased energy expenditure in
burn patients [12,13] and its main substrates are amino acids
derived from muscle catabolism and lactate produced by the
burn wound itself [12,13]. Although in vivo studies have shown
an increase in hepatic gluconeogenesis [14–16], Yamaguchi
and coworkers showed that gluconeogenesis in isolated
perfused rat livers after burn is not increased compared to
sham-burned animals [15]. Hence, it seems that increased
gluconeogenesis does not result from intrinsic hepatic
changes, but from the release of systemic mediators that
act on the liver [8,17,18]. In critical illness, systemic mediators
of gluconeogenesis include glucagon, catecholamines and
corticosteroids. Specifically in the setting of burn injury,
glucagon has been shown to be a significant stimulator of
gluconeogenesis [8]. On the other hand, catecholamines do not
seem to contribute to increased glucose production, since
adrenergic blockade potentiates glucose production [19]. Of
note, glucose oxidation is increased after thermal injury and
does not contribute to increased gluconeogenesis [11].
Increased gluconeogenesis after burn is characterized by
inefficient use of metabolic substrates. For example, the total
rate of gluconeogenesis and glycolysis, which are opposing
metabolic pathways, is increased 2.5-fold, leading to increased
energy expenditure [20]. Although one would expect increased
gluconeogenesis to cause a net increase in hepatic glucose
production, some studies have shown this not to be the case
atients.
Indirect effects References
Insulin resistance [73]
[73]
Insulin resistance [74]
[74]
ort [75]
Insulin resistance [76]
g [77]
g [77]
g [78]
sal " IGF-1 [79]
[80]
sal Reduced insulin secretion [81]
protein; IGF, insulin-like growth factor.

b u r n s 3 6 ( 2 0 1 0 ) 5 9 9 – 6 0 5 601
[18,21]. In an animal model of burn, Lee et al found that
gluconeogenesis was significantly upregulated and glucose
was diverted to the pentose phosphate pathway to support the
production of antioxidants [21]. Hence, the net glucose output
was not increased compared to control animals [21].
2.2. Insulin resistance
Insulin resistance is a critical part of the etiology of
hyperglycemia after burn and its etiology is poorly understood
[22]. The first 48 h after thermal injury (‘ebb’ phase) are
characterized by decreased metabolic rate and soon give way
to hypermetabolism (‘flow’ phase) accompanied by hyper-
insulinemia and hyperglycemia, the hallmark of insulin
resistance [23]. Insulin resistance is thought to be mediated
by local and systemic release of hormones and factors that
oppose insulin action, among which are glucagon, corticos-
teroids and catecholamines [24]. Insulin resistance results
both from reduced insulin-mediated glucose uptake in
skeletal muscle and by loss of muscle mass, the most
important tissue for glucose disposal [9,25]. Indeed, there is
evidence that cytokine release after burn injury can reduce
glucose uptake by skeletal muscle [26]. Perhaps the most
important contributor to insulin resistance is muscle wasting.
Other studies suggest an increased rate of glucose uptake by
tissues other than skeletal muscle, such as skin, wound and
intestine [24].
Although insulin seems to retain its biological effective-
ness in burn patients, there is significant evidence of insulin
resistance in response to injury [17], which tends to progress
with time [27]. Studies in animal models on the molecular
basis of burn-induced insulin resistance have revealed
defects in activation of the insulin receptor itself and of
downstream intracellular pathways which are activated by
insulin binding to its receptors [28]. Akt/PKB is an intracellular
enzyme responsible for glucose uptake and glycogen synthe-
sis that is activated by insulin [28]. Akt/PKB activation by
insulin in skeletal muscle is impaired following burn and may
be involved in the impaired metabolism and muscle wasting
found in these patients [28]. However, insulin administration
following burn increases protein turnover but does not result
in a positive protein balance [29,30]. To further complicate
muscle protein dynamics, burn patients seem to have a
different response to insulin therapy than healthy volun-
teers. Sakurai et al. found that 7-day systemic high-dose
insulin infusion increased muscle proteolysis in burn patients
and attributed this paradox to adaptation to hyperinsuline-
mia [7]. These investigators hypothesized that insulin acutely
stimulates protein synthesis, leading to depletion of the
intracellular amino acid pool, and that this acute phase is
then followed by stimulation of proteolysis to maintain
intracellular amino acid concentrations during prolonged
insulin infusion [7].
3. Deleterious effects of hyperglycemia
Despite its uncertain pathogenesis, hyperglycemia in the
immediate post-burn injury period is associated with in-
creased morbidity and mortality [31]. Multiple mechanisms for
this increased morbidity and mortality are thought to be
involved. Impairment of the immune system and an increased
risk of infection have been demonstrated, and there is
evidence that these effects result from leukocyte dysfunction,
changes in immunoglobulin structure, proinflammatory
changes and leukopenia [32–34]. Particularly important in
burn patients are the defects in wound and skin graft healing,
and increased muscle catabolism associated with hypergly-
cemia [5,9,33,35,36].
Some of the deleterious effects of hyperglycemia have been
elucidated at the cellular and molecular level. Hyperglycemia
contributes to endothelial dysfunction, one of the main
pathways to organ failure in critical illness. Endothelial
dysfunction leads to activation of the inflammatory response,
platelet degranulation and coagulopathy [32,37,38]. In turn,
these effects create a prothrombotic state that contributes to
organ hypoperfusion [32,37]. Langouche et al showed that
correction of hyperglycemia in critically ill patients reduces
endothelial activation by suppressing production of inducible
nitric oxide synthase, a key enzyme in nitric oxide production
and endothelial activation [38]. Furthermore, in an animal
model of burn, Vanhorebeek et al. demonstrated that
hyperglycemia impairs mitochondrial function despite ade-
quate tissue oxygenation and perfusion [10]. In their study,
hyperglycemia was shown to upregulate glycolysis, leading to
accumulation of excessive amounts of metabolites which
were toxic to mitochondria [10]. Interestingly, this effect of
hyperglycemia was more pronounced in the presence of
hyperinsulinemia.
Besides causing hyperglycemia, thermal injury has direct
effects on glucose utilization by tissues and organs. In an
animal model of burn, deregulated expression of enzymes and
transporters involved in glucose uptake and utilization caused
dysfunction of muscle mitochondria [39].
4. Pharmacological agents and burn-relatedmetabolic abnormalities
4.1. Insulin therapy
Peak serum glucose concentrations and duration of hypergly-
cemia are independently associated with increased morbidity
and mortality in critically ill adults and children [40–42]. In
response to the deleterious effects of hyperglycemia, insulin
treatment has been the mainstay of glucose control in the
critically ill [43].
Intravenous insulin infusion inhibits proteolysis, an effect
which is maximal in the splanchnic region and less potent in
skeletal muscle [44]. In addition, insulin administration
stimulates protein synthesis and intracellular transport of
certain amino acids [45]. These effects are dependent not only
on the presence of insulin but also on amino acid availability,
which is paradoxically reduced by insulin infusion [30,46].
Hence, administration of insulin alone will fail to prevent
muscle proteolysis due to depletion of the intracellular amino
acid pool and decreases in intracellular amino acid transport.
The net effect of exogenous insulin and amino acid adminis-
tration is to create a net positive nitrogen balance. Interest-
ingly, the beneficial effects of insulin on muscle protein are

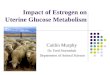
Fig. 1 – Scatter plot of third day average glucose level as a
function of age and glycemic control with regard to follow
up outcome of sepsis and mortality.
b u r n s 3 6 ( 2 0 1 0 ) 5 9 9 – 6 0 5602
maintained during prolonged administration, resulting in
improved outcomes, such as reduced hospital stay [31].
In a landmark study by van den Berghe et al. of surgical ICU
patients, intensive glycemic control with insulin to a serum
glucose goal of 80–110 mg/dl significantly reduced mortality
and morbidity, regardless of patient diabetic status [47].
Insulin therapy also improved intermediate measures of
morbidity such as: length of ICU stay, duration of ventilatory
support, need for renal replacement therapy and the incidence
of critical illness polyneuropathy and septicemia. This study
did include burn patients, however their number was too
small to allow outcome extrapolations for this subgroup [47].
In the immediate period following burn, hyperglycemia is
prevalent and frequently inadequately treated, despite evi-
dence that it is associated with increased mortality [48].
Subsequently, van den Burghe and colleagues concluded that
the mechanism of insulin’s benefit is likely due to the
establishment and maintenance of normoglycemia rather
than a direct effect of insulin [49,50]. However, insulin has
direct effects unrelated to glucose homeostasis that are
beneficial in critically ill patients. In the critically ill cardiac
surgery population, infusion of glucose, insulin and potassium
(GIK) improves cardiovascular and cerebral function in
patients with cardiac or cerebral ischemia [32]. Insulin has
been shown to regulate the systemic inflammatory response
to critical illness, which is thought to be important in reducing
multi-organ dysfunction in critically ill patients [51,52]. Insulin
markedly reduces the hepatic acute phase response, which is
implicated in the systemic inflammatory reaction and
catabolic response after thermal injury [53,54]. Jeschke et al.
demonstrated that insulin therapy significantly improves
hepatic morphology and function in rat models of burn and
endotoxemia [55,56]. Although the role of insulin in main-
taining muscle mass after burn has been investigated [6,7], the
potential benefit on other outcomes in burn patients, includ-
ing mortality, is unknown. In a recent study, intensive insulin
therapy was shown to be successful in achieving normogly-
cemia in adult burn patients [57].
Despite the absence of published trials, there is good reason
to suspect a clinical benefit of tight glucose control achieved by
insulin infusion therapy in the adult burn population. In
children with severe burns, Pham et al. found that intensive
glycemic control (90–120 mg/dl) achieved by insulin infusion
reduces rates of urinary tract infection and overall mortality
[58]. In our own study of adult patients in the burn ICU and
surgical ICU, intensive insulin therapy which achieved a mean
blood glucose level of no more than 150 mg/dl by day 3 of the
infusion was shown to have a similar survival benefit in the
burn population as in the mixed surgical ICU population [59]
(Fig. 1).
While potentially beneficial in critically ill patients and
those with severe burn, insulin therapy is not without risk.
Van den Berghe et al. found that the incidence of hypoglyce-
mia was up to eight times greater in patients receiving
intensive insulin therapy than in controls [47]. In a second
study by Van den Berghe et al. in medical ICU patients,
hypoglycemia was identified as an independent risk factor for
death and possibly reduced the beneficial effect of insulin in
the treatment arm of the study [47,60]. Despite improved
mortality, hypoglycemia occurred in 18% of patients with
acute cardiac ischemia treated with intravenous insulin to
maintain normoglycemia [61] (126–196 mg/dl). In addition,
hypoglycemia was more frequently observed in severely
burned children receiving insulin therapy to maintain
normoglycemia [58]. In a separate study of intensive insulin
therapy in burn patients, the incidence of hypoglycemia was
5% and did not result in significance adverse effects [57].
Although the authors of the above studies concluded that
intensive insulin therapy is safe, hypoglycemia is a significant
problem even in an ICU setting where blood glucose can be
closely monitored.
Furthermore, there are significant barriers to implement-
ing intensive insulin protocols in the ICU. For instance, in their
study of insulin therapy in severely burned children, Pham
et al. emphasized the difficulty of convincing health care
professionals of the need to maintain subjects on an
intravenous insulin infusion when serum glucose remained
at levels considered ‘acceptable’ [58]. They reported that,
during the initial study period, ICU staff were concerned about
insulin-induced hypoglycemia and tended to inappropriately
terminate insulin infusion, resulting in rebound hyperglyce-
mia. In addition, further research into staff resistance to tight
glycemic control protocols has been likened to selling ‘‘root
canals’’ to the ICU staff [62]. Hence, a significant ‘learning
curve’ occurs during implementation of intensive insulin
therapy [58].
In burn patients, the frequent need to return to the
operating room for grafting and other procedures often results
in a mandated suspension of the insulin infusion during
anesthesia. This is counter-productive in that rebound
hyperglycemia frequently occurs with suspension of the
insulin infusion. In cardiac surgery patients, intra-operative
insulin therapy has been found to be safe and effective in
maintaining euglycemia, and is thought to be an important
component of achieving and maintaining euglycemia [63]. In
addition, the frequent use of enteral tube feeding in burn
patients makes intensive insulin therapy more problematic,

b u r n s 3 6 ( 2 0 1 0 ) 5 9 9 – 6 0 5 603
particularly if the enteral feedings are temporarily suspended
during operative procedures. Despite these aspects of routine
burn care, insulin infusions can be maintained with appropri-
ate attention to frequent blood glucose determinations.
Another potential concern with insulin and glucose admin-
istration is hepatic injury. Burned patients are predisposed to
hepatic steatosis, even in the absence of insulin and glucose
therapy. Contributing factors are thought to include: insulin-
induced hepatic lipogenesis, increased hepatic delivery of
glucose, and increased fatty acid release from adipose tissue
[7,64,65]. Importantly, in studies that used continuous insulin
infusion at 28 units/h, caloric needs in the form of glucose
increased twofold, however; hepatic steatosis did not occur
[7,66]. The authors attributed this absence of steatosis to the
concurrent infusion of insulin, directing excess glucose to
tissues with insulin-dependent glucose uptake such as skeletal
muscle and adipose tissue, and not to the liver, where glucose
uptake is insulin-independent and proportional to portal vein
glucose levels. It appears that when normoglycemia is main-
tained, burn patients do not get hepatic steatosis [66]. A recent
study showed that insulin can protect the liver from alcohol-
induced steatosis in burn patients [67]. Elevated blood alcohol is
common in patients with burns and contributes to hepatic
steatosis, which can progress to severe hepatic dysfunction [67].
Of note, both insulin-induced peripheral glucose uptake and its
conversion to triglycerides were found to be normal in burn
patients [7,68].
Unfortunately, low-dose insulin therapy has not been found
to prevent hyperglycemia in burn patients and does not affect
muscle glucose uptake; therefore, it does not change patient
caloricdemands[6].Since mostof theobservedbenefit of insulin
therapy results from maintaining normoglycemia [49,50], low-
dose insulin therapy which does not result in euglycemia would
be expected to have reduced impact on overall outcomes.
4.2. Metformin
The role of metformin has been examined in an effort to reduce
hyperglycemic complications in the immediate post-burn
period, while attempting to avoid the attendant risk of
hypoglycemia noted with intensive insulin therapy. Metformin
acts by reducing hepatic gluconeogenesis and improving
peripheral insulin sensitivity, which are the most significant
pathophysiologic alterations responsible for hyperglycemia
following burn injury [69]. In addition, there is evidence that
metformin acts by an additional mechanism in burn patients:
the augmentation of endogenous insulin release [43]. A parti-
cularlyappealing advantage of metformin is itsability toachieve
normoglycemia without the need of frequent glucose monitor-
ing [43]. However, what prevents metformin therapy from being
ideal in the burn populace is that this agent is associated with
potentially lethal lactic acidosis in patients with septic shock,
hypovolemia and heart failure, which can be common in
patients with significant burns [43]. Therefore, metformin has
not been advocated as routine therapy in burn patients.
4.3. Other agents
A number of other pharmacological agents have been
examined in burn patients in an attempt to reverse the
numerous metabolic abnormalities present in this patient
population. In a recent randomized trial, fenofibrate, a PPAR-g
agonist, was shown to improve insulin-mediated glucose
disposal and insulin-mediated inhibition of hepatic glucose
release in children with significant burns [70]. In addition,
growth hormone and insulin-like growth factor-1 therapy
have been studied for their potential anabolic effects and have
been associated with decreased mortality in burn patients. It is
unknown whether this clinical benefit arises through an
anabolic effect or through an insulin-mediated effect [71].
Finally, despite its lack of direct effects on glucose
metabolism, oxandrolone stimulates protein synthesis and
has proven benefits in burn patients, including improved
wound healing and decreased hospital length of stay
[45,72,73]. Unfortunately, a prolonged ventilation requirement
is a potential concern with oxandrolone administration [28]. In
one study, where oxandrolone administration was found to
prolong the need for ventilatory support, it was proposed that
the prolongation was due to increased pulmonary collagen
deposition [28].
5. Conclusion
Thermal injury leads to a systemic catabolic response with
adverse effects on glucose homeostasis and muscle protein
balance. Morbidity and mortality outcomes in critically ill
patients, including burn patients, depend in part on the
control of these metabolic changes. Numerous strategies,
including nutritional support and treatment with anabolic
hormones, have been examined in an effort to reverse the
catabolic response to burn injury. Intensive insulin therapy in
the ICU setting has been shown to reduce patient morbidity
and mortality and is being widely used in surgical patients.
Although problematic in burn patients, intensive insulin
therapy holds the potential to reduce the incidence of
complications such as sepsis through improved glycemic
control, and may improve overall outcomes in critically ill
burn patients.
Conflict of interest
None of the authors have anything to disclose.
r e f e r e n c e s
[1] Ipaktchi K, Arbabi S. Advances in burn critical care. CritCare Med 2006;34(9 Suppl.):S239–44.
[2] Gauglitz GG, Herndon DN, Kulp GA, Meyer 3rd WJ, JeschkeMG. Abnormal insulin sensitivity persists up to three yearsin pediatric patients post-burn. J Clin Endocrinol Metab2009;94(5):1656–64.
[3] Gore DC, Jahoor F. Glutamine kinetics in burn patients.Comparison with hormonally induced stress in volunteers.Arch Surg 1994;129(12):1318–23.
[4] Gore DC, Chinkes DL, Wolf SE, Sanford AP, Herndon DN,Wolfe RR. Quantification of protein metabolism in vivo forskin, wound, and muscle in severe burn patients. JPEN2006;30(4):331–8.

b u r n s 3 6 ( 2 0 1 0 ) 5 9 9 – 6 0 5604
[5] Gore DC, Wolf SE, Herndon DN, Wolfe RR. Relativeinfluence of glucose and insulin on peripheral amino acidmetabolism in severely burned patients. JPEN2002;26(5):271–7.
[6] Ferrando AA, Chinkes DL, Wolf SE, Matin S, Herndon DN,Wolfe RR. A submaximal dose of insulin promotes netskeletal muscle protein synthesis in patients with severeburns. Ann Surg 1999;229(1):11–8.
[7] Sakurai Y, Aarsland A, Herndon DN, Chinkes DL, Pierre E,Nguyen TT, et al. Stimulation of muscle protein synthesisby long-term insulin infusion in severely burned patients.Ann Surg 1995;222(3). 283-94; 94-7.
[8] Jahoor F, Herndon DN, Wolfe RR. Role of insulin andglucagon in the response of glucose and alaninekinetics in burn-injured patients. J Clin Invest 1986;78(3):807–14.
[9] Gore DC, Chinkes DL, Hart DW, Wolf SE, Herndon DN,Sanford AP. Hyperglycemia exacerbates muscle proteincatabolism in burn-injured patients. Crit Care Med2002;30(11):2438–42.
[10] Vanhorebeek I, Ellger B, De Vos R, Boussemaere M,Debaveye Y, Perre SV, et al. Tissue-specific glucose toxicityinduces mitochondrial damage in a burn injury model ofcritical illness. Crit Care Med 2009;37(4):1355–64.
[11] Wolfe RR, Jahoor F, Herndon DN, Miyoshi H. Isotopicevaluation of the metabolism of pyruvate and relatedsubstrates in normal adult volunteers and severely burnedchildren: effect of dichloroacetate and glucose infusion.Surgery 1991;110(1):54–67.
[12] Yu YM, Tompkins RG, Ryan CM, Young VR. The metabolicbasis of the increase of the increase in energy expenditurein severely burned patients. JPEN 1999;23(3):160–8.
[13] Yarmush DM, MacDonald AD, Foy BD, Berthiaume F,Tompkins RG, Yarmush ML. Cutaneous burn injury altersrelative tricarboxylic acid cycle fluxes in rat liver. J BurnCare Rehabil 1999;20(4):292–302.
[14] Burke JF, Wolfe RR, Mullany CJ, Mathews DE, Bier DM.Glucose requirements following burn injury. Parameters ofoptimal glucose infusion and possible hepatic andrespiratory abnormalities following excessive glucoseintake. Ann Surg 1979;190(3):274–85.
[15] Wolfe RR, Durkot MJ, Allsop JR, Burke JF. Glucosemetabolism in severely burned patients. Metabolism1979;28(10):1031–9.
[16] Wolfe RR. Metabolic response to burn injury: nutritionalimplications. Keio J Med 1993;42(1):1–8.
[17] Jahoor F, Shangraw RE, Miyoshi H, Wallfish H, Herndon DN,Wolfe RR. Role of insulin and glucose oxidation inmediating the protein catabolism of burns and sepsis. Am JPhysiol 1989;257(3 Pt 1):E323–31.
[18] Yamaguchi Y, Yu YM, Zupke C, Yarmush DM, BerthiaumeF, Tompkins RG, et al. Effect of burn injury on glucose andnitrogen metabolism in the liver: preliminary studies in aperfused liver system. Surgery 1997;121(3):295–303.
[19] Durkot MJ, Wolfe RR. Effects of adrenergic blockade onglucose kinetics in septic and burned guinea pigs. Am JPhysiol 1981;241(3):R222–7.
[20] Wolfe RR, Herndon DN, Jahoor F, Miyoshi H, Wolfe M. Effectof severe burn injury on substrate cycling by glucose andfatty acids. N Engl J Med 1987;317(7):403–8.
[21] Lee K, Berthiaume F, Stephanopoulos GN, Yarmush DM,Yarmush ML. Metabolic flux analysis of postburn hepatichypermetabolism. Metab Eng 2000;2(4):312–27.
[22] Cree MG, Wolfe RR. Postburn trauma insulin resistance andfat metabolism. Am J Physiol Endocrinol Metab2008;294(1):E1–9.
[23] Gauglitz GG, Herndon DN, Jeschke MG. Insulin resistancepostburn: underlying mechanisms and current therapeuticstrategies. J Burn Care Res 2008;29(5):683–94.
[24] Carter EA, Tompkins RG, Babich JW, Correia J, Bailey EM,Fischman AJ. Thermal injury in rats alters glucoseutilization by skin, wound, and small intestine, but not byskeletal muscle. Metabolism 1996;45(9):1161–7.
[25] DeFronzo R. The effect of insulin on renal sodiummetabolism. A review with clinical implications.Diabetologia 1981;21:165–71.
[26] Fang CH, Li BG, James JH, Fischer JE, Hasselgren PO.Cytokines block the effects of insulin-like growth factor-I(IGF-I) on glucose uptake and lactate production in skeletalmuscle but do not influence IGF-I-induced changes inprotein turnover. Shock 1997;8(5):362–7.
[27] Pidcoke HF, Salinas J, Wanek SM, Concannon M, Loo F,Wirfel KL, et al. Patterns of exogenous insulin requirementreflect insulin sensitivity changes in trauma. Am J Surg2007;194(6):798–803 [discussion].
[28] Sugita H, Kaneki M, Sugita M, Yasukawa T, Yasuhara S,Martyn JA. Burn injury impairs insulin-stimulated Akt/PKBactivation in skeletal muscle. Am J Physiol EndocrinolMetab 2005;288(3):E585–91.
[29] Gore DC, Wolf SE, Sanford AP, Herndon DN, Wolfe RR.Extremity hyperinsulinemia stimulates muscle proteinsynthesis in severely injured patients. Am J PhysiolEndocrinol Metab 2004;286(4):E529–34.
[30] Zhang XJ, Chinkes DL, Irtun O, Wolfe RR. Anabolic action ofinsulin on skin wound protein is augmented by exogenousamino acids. Am J Physiol Endocrinol Metab2002;282(6):E1308–15.
[31] Gore DC, Chinkes D, Heggers J, Herndon DN, Wolf SE, DesaiM. Association of hyperglycemia with increased mortalityafter severe burn injury. J Trauma 2001;51(3):540–4.
[32] Clement S, Braithwaite SS, Magee MF, Ahmann A, Smith EP,Schafer RG, et al. Management of diabetes andhyperglycemia in hospitals. Diabetes Care 2004;27(2):553–91.
[33] Black CT, Hennessey PJ, Andrassy RJ. Short-termhyperglycemia depresses immunity through nonenzymaticglycosylation of circulating immunoglobulin. J Trauma1990;30(7):830–2 [discussion 2–3].
[34] von Kanel R, Mills PJ, Dimsdale JE. Short-termhyperglycemia induces lymphopenia and lymphocytesubset redistribution. Life Sci 2001;69(3):255–62.
[35] Perner A, Nielsen SE, Rask-Madsen J. High glucose impairssuperoxide production from isolated blood neutrophils.Intens Care Med 2003;29(4):642–5.
[36] Mowlavi A, Andrews K, Milner S, Herndon DN, Heggers JP.The effects of hyperglycemia on skin graft survival in theburn patient. Ann Plast Surg 2000;45(6):629–32.
[37] Weekers F, Giulietti AP, Michalaki M, Coopmans W, VanHerck E, Mathieu C, et al. Metabolic, endocrine, andimmune effects of stress hyperglycemia in a rabbit modelof prolonged critical illness. Endocrinology2003;144(12):5329–38.
[38] Langouche L, Vanhorebeek I, Vlasselaers D, Vander Perre S,Wouters PJ, Skogstrand K, et al. Intensive insulin therapyprotects the endothelium of critically ill patients. J ClinInvest 2005;115(8):2277–86.
[39] Padfield KE, Astrakas LG, Zhang Q, Gopalan S, Dai G,Mindrinos MN, et al. Burn injury causes mitochondrialdysfunction in skeletal muscle. Proc Natl Acad Sci USA2005;102(15):5368–73.
[40] Capes SE, Hunt D, Malmberg K, Gerstein HC. Stresshyperglycaemia and increased risk of death after myocardialinfarction in patients with and without diabetes: asystematic overview. Lancet 2000;355(9206):773–8.
[41] Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC.Stress hyperglycemia and prognosis of stroke innondiabetic and diabetic patients: a systematic overview.Stroke 2001;32(10):2426–32.

b u r n s 3 6 ( 2 0 1 0 ) 5 9 9 – 6 0 5 605
[42] Srinivasan V, Spinella PC, Drott HR, Roth CL, Helfaer MA,Nadkarni V. Association of timing, duration, and intensityof hyperglycemia with intensive care unit mortality incritically ill children. Pediatr Crit Care Med 2004;5(4):329–36.
[43] Gore DC, Wolf SE, Herndon DN, Wolfe RR. Metformin bluntsstress-induced hyperglycemia after thermal injury. JTrauma 2003;54(3):555–61.
[44] Arora NS, Rochester DF. Respiratory muscle strength andmaximal voluntary ventilation in undernourished patients.Am Rev Respir Dis 1982;126(1):5–8.
[45] Biolo G, Declan Fleming RY, Wolfe RR. Physiologichyperinsulinemia stimulates protein synthesis andenhances transport of selected amino acids in humanskeletal muscle. J Clin Invest 1995;95(2):811–9.
[46] Thomas SJ, Morimoto K, Herndon DN, Ferrando AA, WolfeRR, Klein GL, et al. The effect of prolonged euglycemichyperinsulinemia on lean body mass after severe burn.Surgery 2002;132(2):341–7.
[47] Van den Berghe G, Wouters P, Weekers F, Verwaest C,Bruyninckx F, Schetz M, et al. Intensive insulin therapy inthe critically ill patients. N Engl J Med 2001;345(19):1359–67.
[48] Holm C, Horbrand F, Mayr M, von Donnersmarck GH,Muhlbauer W. Acute hyperglycaemia following thermalinjury: friend or foe? Resuscitation 2004;60(1):71–7.
[49] Ellger B, Debaveye Y, Vanhorebeek I, Langouche L, GiuliettiA, Van Etten E, et al. Survival benefits of intensive insulintherapy in critical illness: impact of maintainingnormoglycemia versus glycemia-independent actions ofinsulin. Diabetes 2006;55(4):1096–105.
[50] Van den Berghe G, Wouters PJ, Bouillon R, Weekers F,Verwaest C, Schetz M, et al. Outcome benefit of intensiveinsulin therapy in the critically ill: insulin dose versusglycemic control. Crit Care Med 2003;31(2):359–66.
[51] Jeschke MG, Einspanier R, Klein D, Jauch KW. Insulinattenuates the systemic inflammatory response to thermaltrauma. Mol Med 2002;8(8):443–50.
[52] Jeschke MG, Klein D, Herndon DN. Insulin treatmentimproves the systemic inflammatory reaction to severetrauma. Ann Surg 2004;239(4):553–60.
[53] Wu X, Thomas SJ, Herndon DN, Sanford AP, Wolf SE.Insulin decreases hepatic acute phase protein levels inseverely burned children. Surgery 2004;135(2):196–202.
[54] Jeschke MG, Barrow RE, Herndon DN. Extendedhypermetabolic response of the liver in severely burnedpediatric patients. Arch Surg 2004;139(6):641–7.
[55] Jeschke MG, Rensing H, Klein D, Schubert T, Mautes AE,Bolder U, et al. Insulin prevents liver damage and preservesliver function in lipopolysaccharide-induced endotoxemicrats. J Hepatol 2005;42(6):870–9.
[56] Klein D, Schubert T, Horch RE, Jauch KW, Jeschke MG.Insulin treatment improves hepatic morphology andfunction through modulation of hepatic signals after severetrauma. Ann Surg 2004;240(2):340–9.
[57] Cochran A, Davis L, Morris SE, Saffle JR. Safety and efficacyof an intensive insulin protocol in a burn-trauma intensivecare unit. J Burn Care Res 2008;29(1):187–91.
[58] Pham TN, Warren AJ, Phan HH, Molitor F, Greenhalgh DG,Palmieri TL. Impact of tight glycemic control in severelyburned children. J Trauma 2005;59(5):1148–54.
[59] Gibson BR, Galiatsatos P, Rabiee A, Eaton L, Abu-Hamdah R,Christmas C, et al. Intensive insulin therapy confers asimilar survival benefit in the burn intensive care unit as inthe surgical intensive care unit. Surgery 2009;146(5):922–30.
[60] Van den Berghe G, Wilmer A, Hermans G, Meersseman W,Wouters PJ, Milants I, et al. Intensive insulin therapy in themedical ICU. N Engl J Med 2006;354(5):449–61.
[61] Malmberg KA, Efendic S, Ryden LE. Feasibility of insulin-glucose infusion in diabetic patients with acute myocardialinfarction. A report from the multicenter trial: DIGAMI.Diabetes Care 1994;17(9):1007–14.
[62] Goldberg PA. Memoirs of a root canal salesman: thesuccessful implementation of a hospital-wide intravenousinsulin infusion protocol. Endocr Pract 2006;12(Suppl. 3):79–85.
[63] Furnary AP, Wu Y, Bookin SO. Effect of hyperglycemia andcontinuous intravenous insulin infusions on outcomes ofcardiac surgical procedures: the Portland Diabetic Project.Endocr Pract 2004;10(Suppl 2):21–33.
[64] Aarsland A, Chinkes D, Wolfe RR. Contributions of de novosynthesis of fatty acids to total VLDL-triglyceride secretionduring prolonged hyperglycemia/hyperinsulinemia innormal man. J Clin Invest 1996;98(9):2008–17.
[65] Gibbons GF. Insulin, diabetes and hepatic very-low-densitylipoprotein metabolism. Biochem Soc Trans 1989;17(1):49–51.
[66] Aarsland A, Chinkes DL, Sakurai Y, Nguyen TT, HerndonDN, Wolfe RR. Insulin therapy in burn patients does notcontribute to hepatic triglyceride production. J Clin Invest1998;101(10):2233–9.
[67] Emanuele NV, Emanuele MA, Morgan MO, Sulo D, Yong S,Kovacs EJ, et al. Ethanol potentiates the acute Fattyinfiltration of liver caused by burn injury: prevention byinsulin treatment. J Burn Care Res 2009;30(3):482–8.
[68] Shangraw RE, Jahoor F, Miyoshi H, Neff WA, Stuart CA,Herndon DN, et al. Differentiation between septic andpostburn insulin resistance. Metabolism 1989;38(10):983–9.
[69] Stumvoll M, Nurjhan N, Perriello G, Dailey G, Gerich JE.Metabolic effects of metformin in non-insulin-dependentdiabetes mellitus. N Engl J Med 1995;333(9):550–4.
[70] Cree MG, Zwetsloot JJ, Herndon DN, Qian T, Morio B, FramR, et al. Insulin sensitivity and mitochondrial function areimproved in children with burn injury during a randomizedcontrolled trial of fenofibrate. Ann Surg 2007;245(2):214–21.
[71] Jenkins RC, Ross RJ. Growth hormone therapy for proteincatabolism. QJM 1996;89(11):813–9.
[72] Tessari P, Trevisan R, Inchiostro S, Biolo G, Nosadini R, DeKreutzenberg SV, et al. Dose–response curves of effects ofinsulin on leucine kinetics in humans. Am J Physiol1986;251(3 Pt 1):E334–42.
[73] Kettelhut IC, Wing SS, Goldberg AL. Endocrine regulation ofprotein breakdown in skeletal muscle. Diabetes Metab Rev1988;4(8):751–72.