Embed Size (px)
Citation preview

GINGIVA
CONTENTS Introduction Macroscopic features Microscopic features
Gingival epithelium
Oral epithelium
Sulcular epithelium
Junctional epithelium Renewal of gingival epithelium Cuticular structures Gingival crevicular fluid Gingival connective tissue Gingival fibres Blood supply, nerve supply and lymphatics Correlation of clinical & microscopic features Age changes
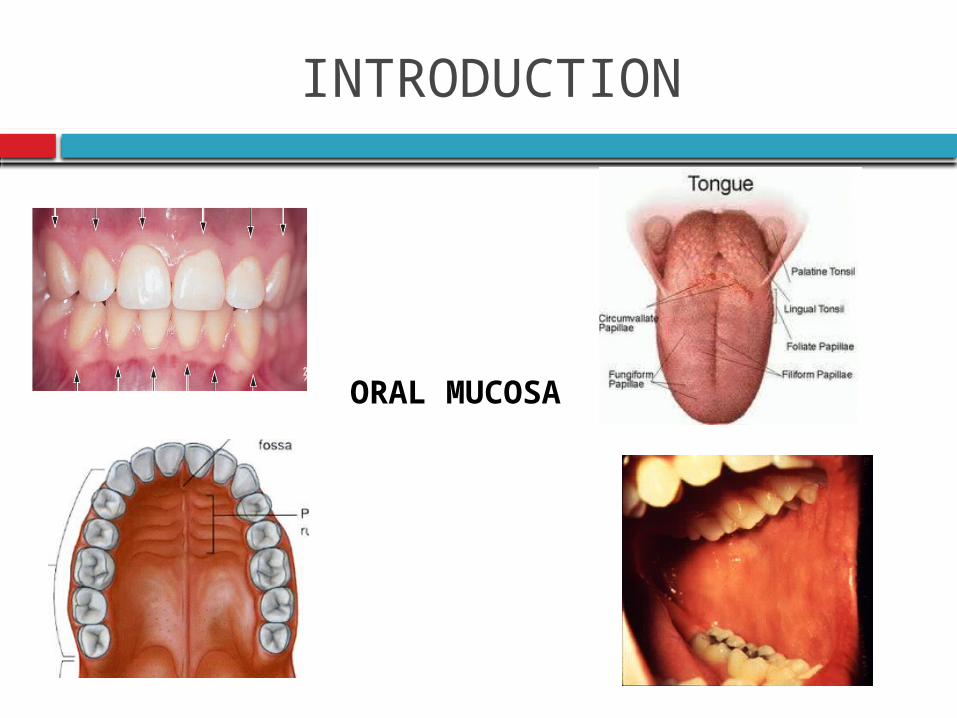
INTRODUCTION
ORAL MUCOSA
GINGIVA
Carranza
Gingiva is the part of the oral mucosa that covers the alveolar processes of the jaws & surrounds the necks of the teeth
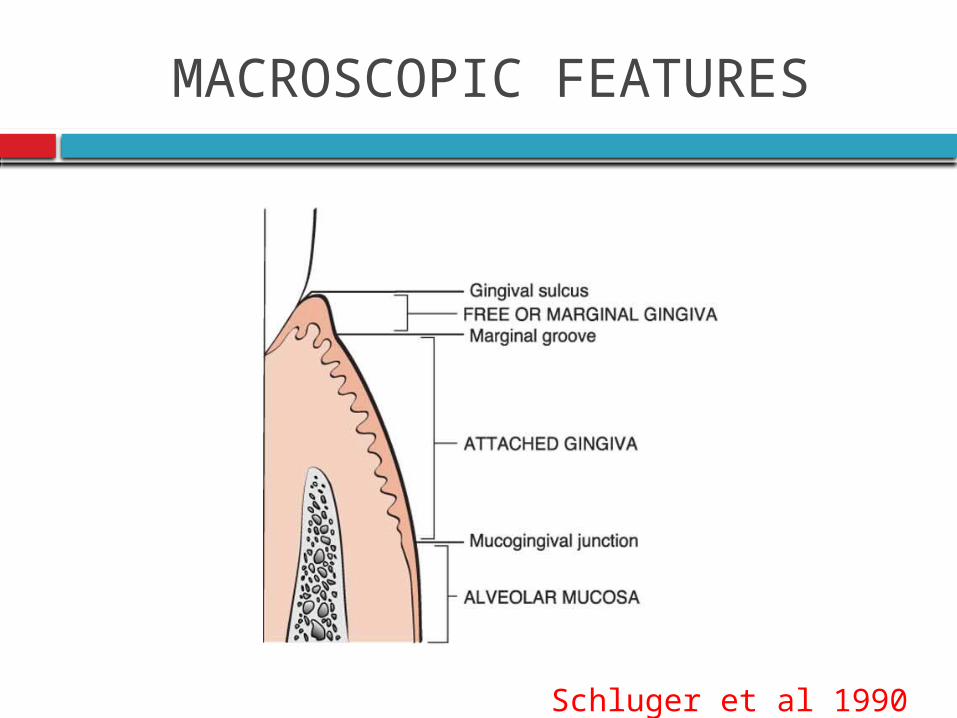
MACROSCOPIC FEATURES
Schluger et al 1990
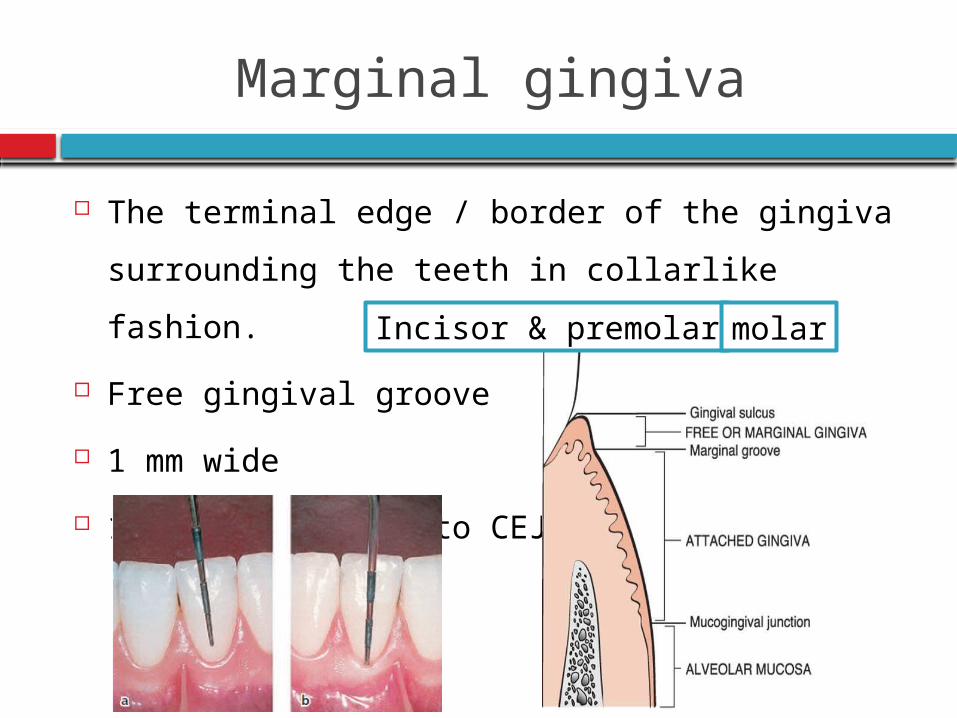
Marginal gingiva
The terminal edge / border of the gingiva
surrounding the teeth in collarlike fashion.
Free gingival groove
1 mm wide
1.5- 2mm coronal to CEJ
Incisor & premolar molar
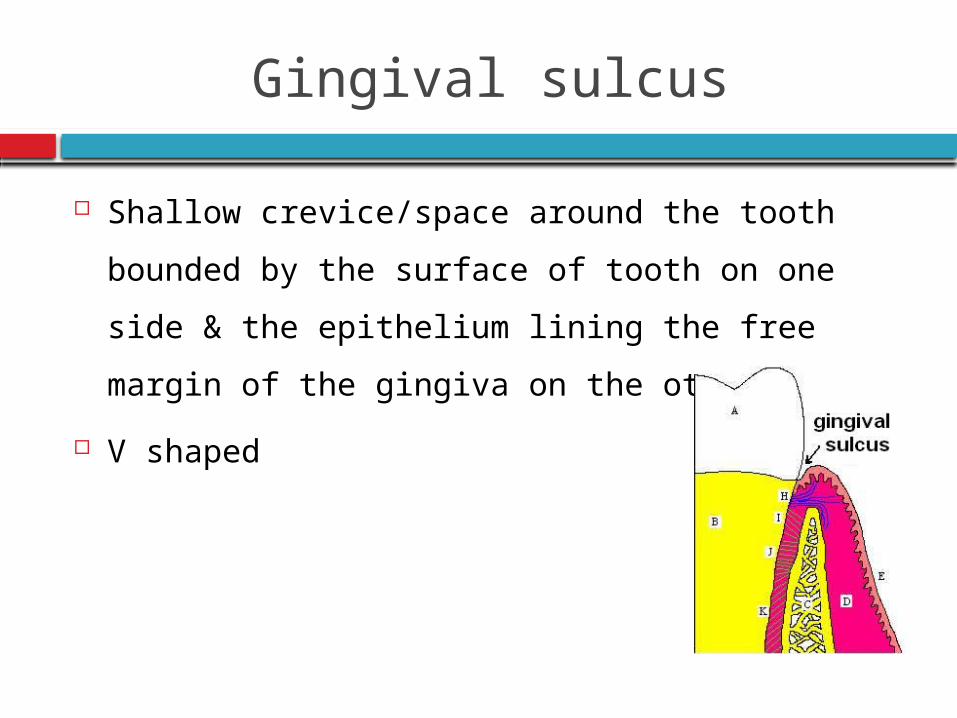
Gingival sulcus
Shallow crevice/space around the tooth bounded
by the surface of tooth on one side & the
epithelium lining the free margin of the gingiva
on the other side
V shaped
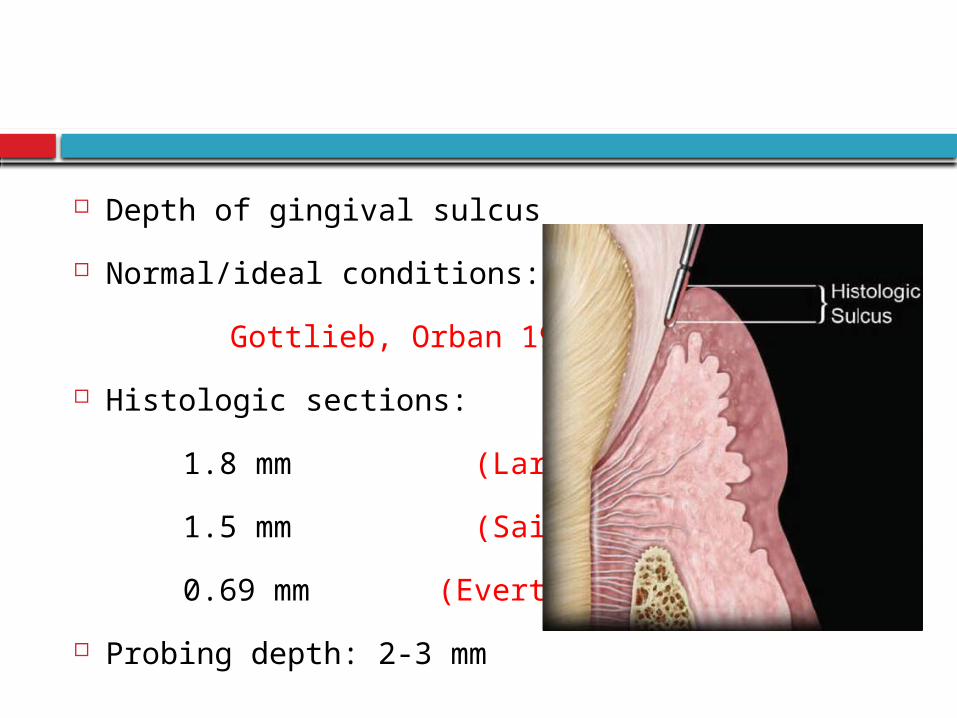
Depth of gingival sulcus
Normal/ideal conditions: 0
Gottlieb, Orban 1933
Histologic sections:
1.8 mm (Larjava et al)
1.5 mm (Saito et al)
0.69 mm (Everts et al)
Probing depth: 2-3 mm
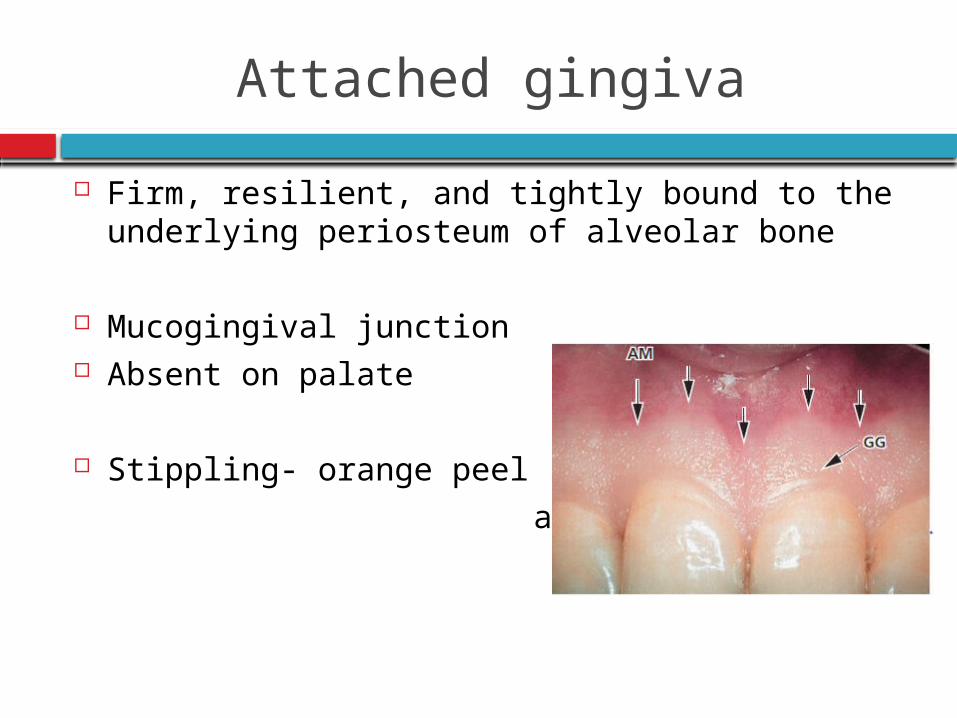
Attached gingiva
Firm, resilient, and tightly bound to the underlying periosteum of alveolar bone
Mucogingival junction Absent on palate
Stippling- orange peel
appearance
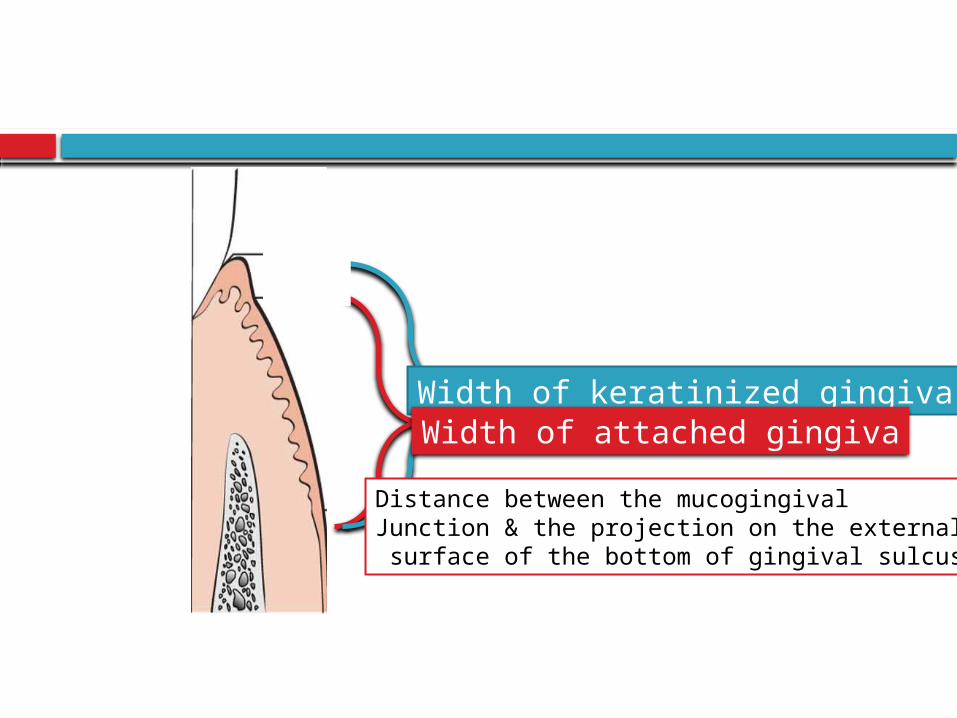
Width of keratinized gingivaWidth of attached gingiva
Distance between the mucogingivalJunction & the projection on the external surface of the bottom of gingival sulcus
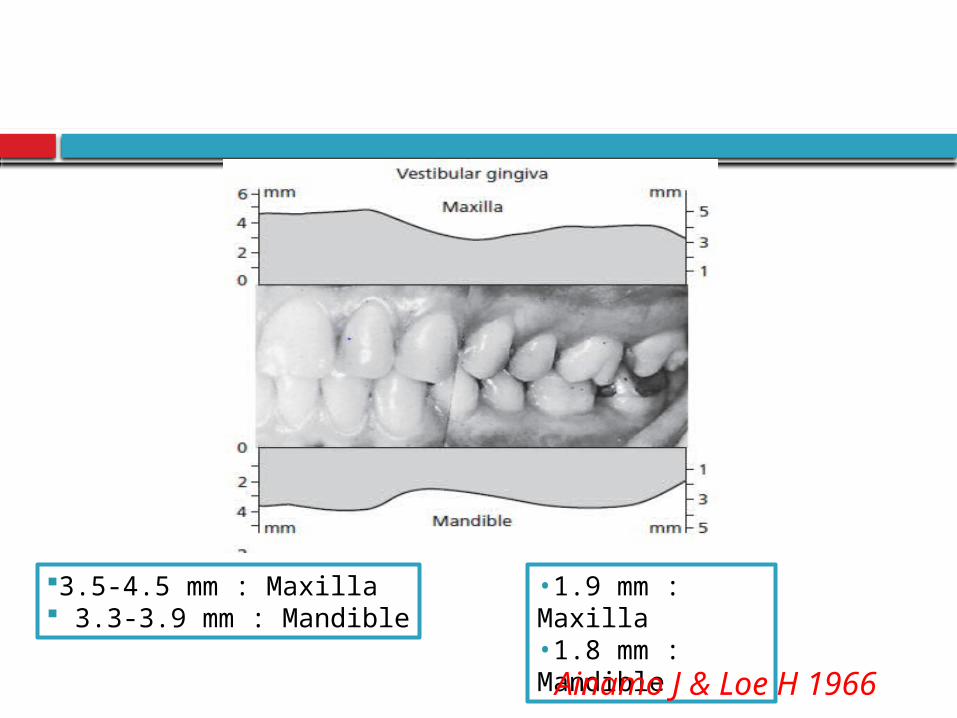
3.5-4.5 mm : Maxilla 3.3-3.9 mm : Mandible
•1.9 mm : Maxilla•1.8 mm : Mandible
Ainamo J & Loe H 1966
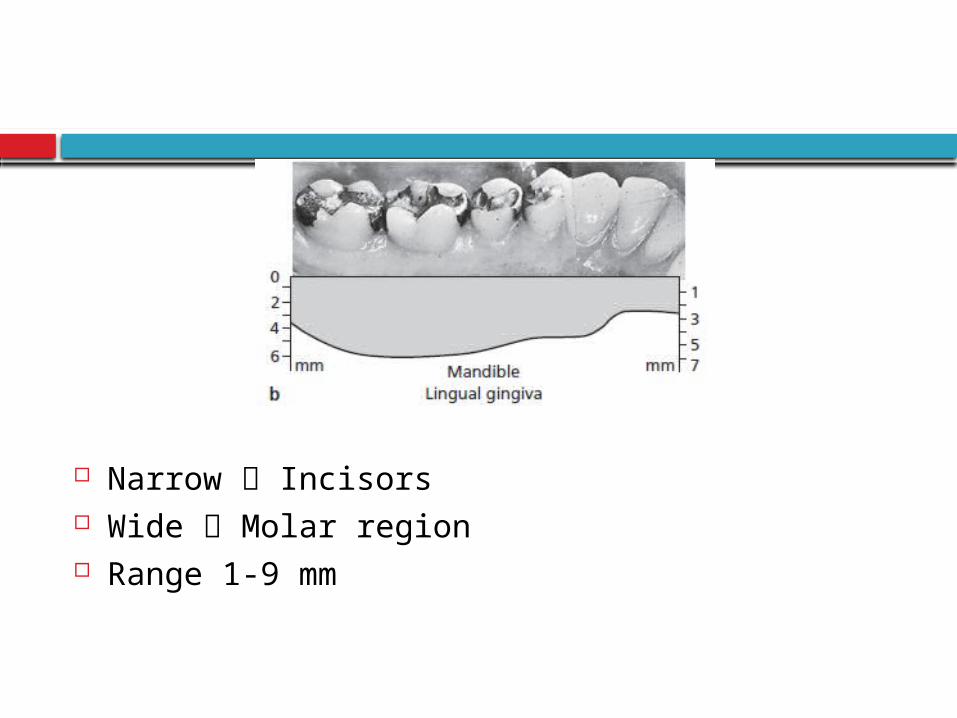
Narrow Incisors Wide Molar region Range 1-9 mm
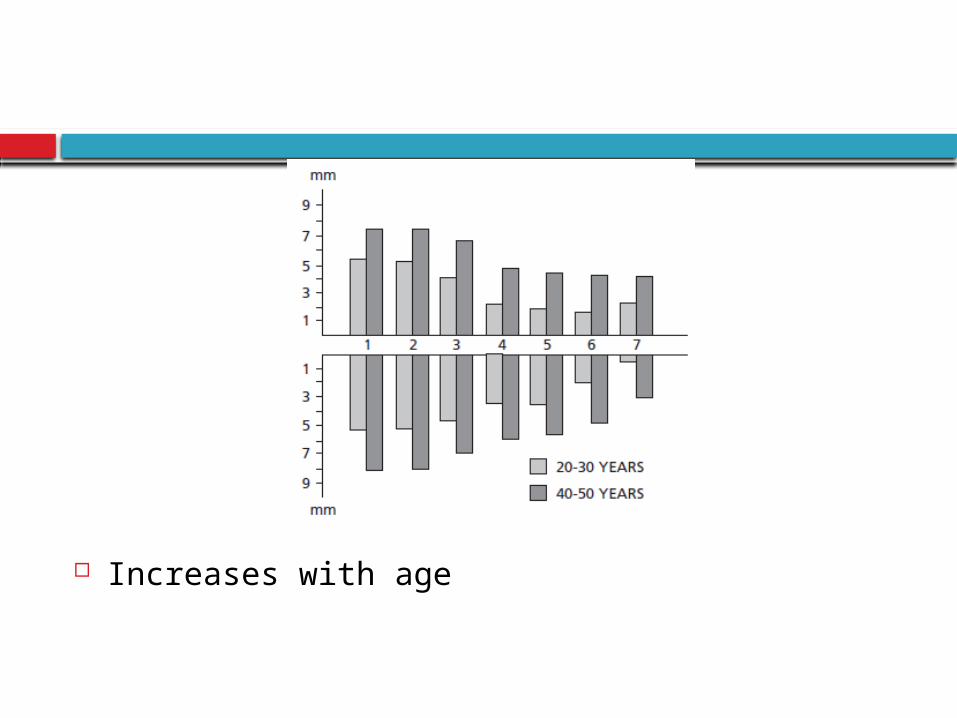
Increases with age
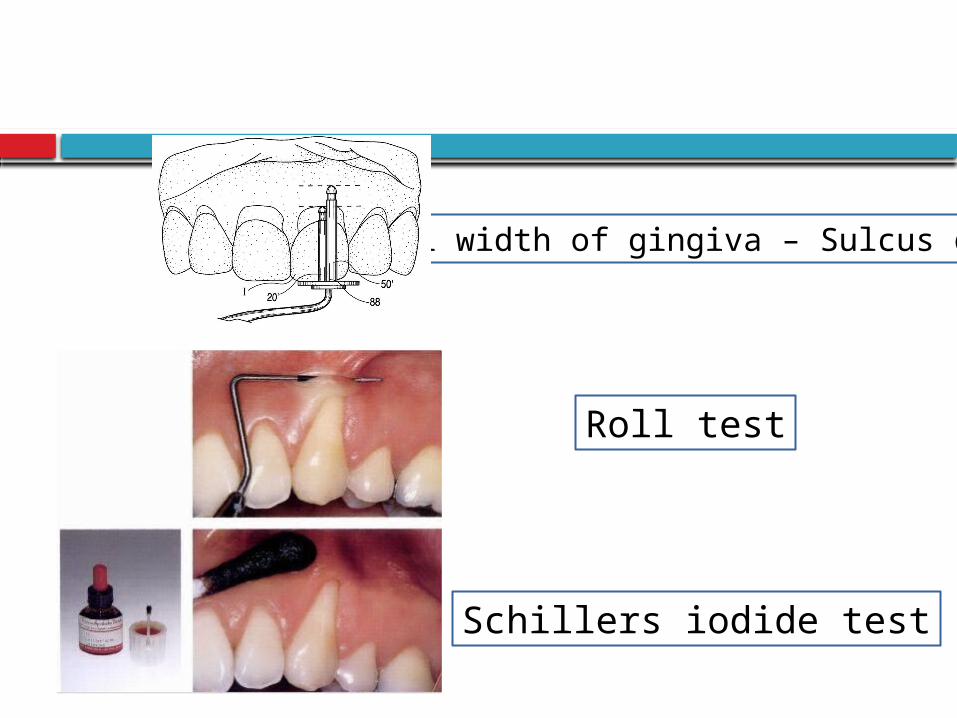
Roll test
Schillers iodide test
Total width of gingiva – Sulcus depth
Importance of attached gingiva
PREDISPOSING FACTORS
INADEQUATE ATTACHED GINGIVA
• Narrow zone of gingiva is considered insufficient to:
– Protect the periodontium from masticatory forces
– Dissipate the pull because of muscles of adjacent mucosa
(Friedman 1957)
• Inadequate zone of gingiva favors:
– Subgingival plaque formation (Friedman, 1962)
– Attachment loss and soft tissue recession due to decreased
resistance to apical spread of plaque associated gingival lesions
(Stern, 1976)
– Along with decreased vestibular depth it causes accumulation of
food particles during mastication and impedes oral hygiene
measures (Gottsegen, 1954)
• Bowers, 1963: Classic study on width of attached gingiva. To clarify meanings of
ADEQUATE / INADEQUATE gingiva.
• Width varied for different teeth and different individuals
• Mean width increased from deciduous to permanent dentition, but changed
little after maturity
• Ranged from 1 – 9mm
• Lowest in the premolar canine region
• Influenced by tooth malposition, frenum attachment and recession
• Recession was most common in 1st premolar-canine, maxillary 1st molar and
mandibular incisor regions
Gingiva could be maintained with <1mm present
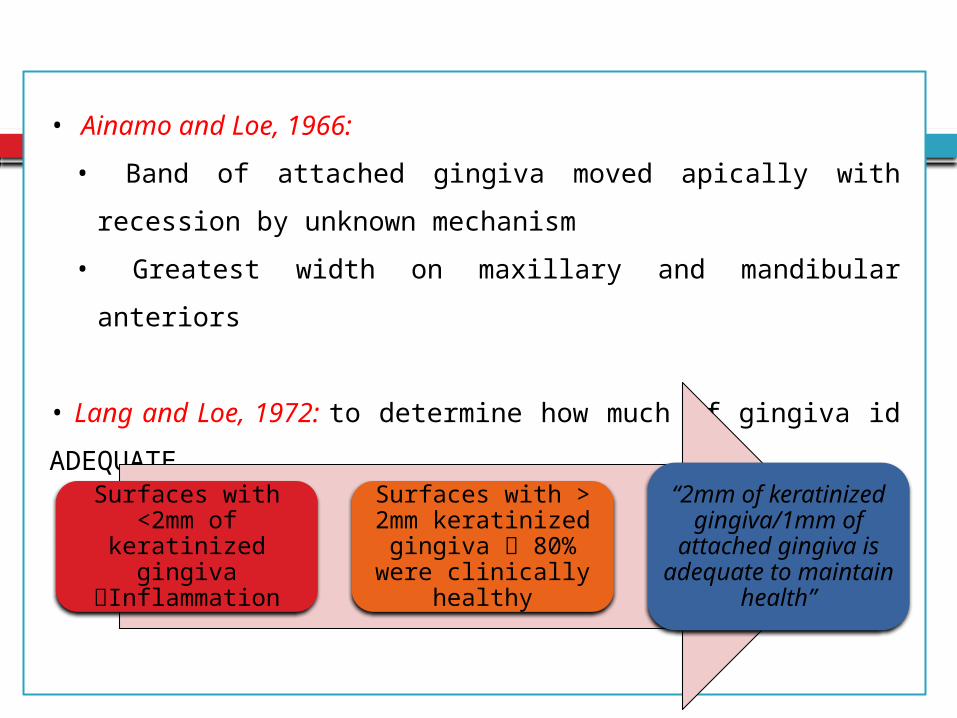
• Ainamo and Loe, 1966:
• Band of attached gingiva moved apically with recession by unknown
mechanism
• Greatest width on maxillary and mandibular anteriors
• Lang and Loe, 1972: to determine how much of gingiva id ADEQUATE
(118 randomly selected plaque free surfaces)
Surfaces with <2mm of
keratinized gingiva Inflammation
Surfaces with > 2mm keratinized
gingiva 80% were clinically healthy
“2mm of keratinized
gingiva/1mm of attached gingiva is
adequate to maintain health”
• Maynard and Wilson, 1979 subgingival restorative
procedures require
2mm free gingiva
3mm attached gingiva
5mm keratinized
gingiva
• Miyasato et al., 1977
Study on dental students
Mid facial plaque free surface of
mandibular premolars
Minimal keratinized
gingiva 1mm
Appreciable keratinized
gingiva 2mm
25 days experimental
gingivitis
Increases in plaque, gingival
exudate and inflammation
were similar in both groups
• Dorfman et al., 1980 2 year study on 92 patients
Experimental side free gingival grafts Control side root planing and oral hygiene instructions every 3 months
Grafted areas had an increase of 4mm of attached gingiva but no difference in GI, PI and loss of attachment compared to the controls
Patient can be maintained in gingival health with excellent oral hygiene and regular periodontal care at 3 month intervals
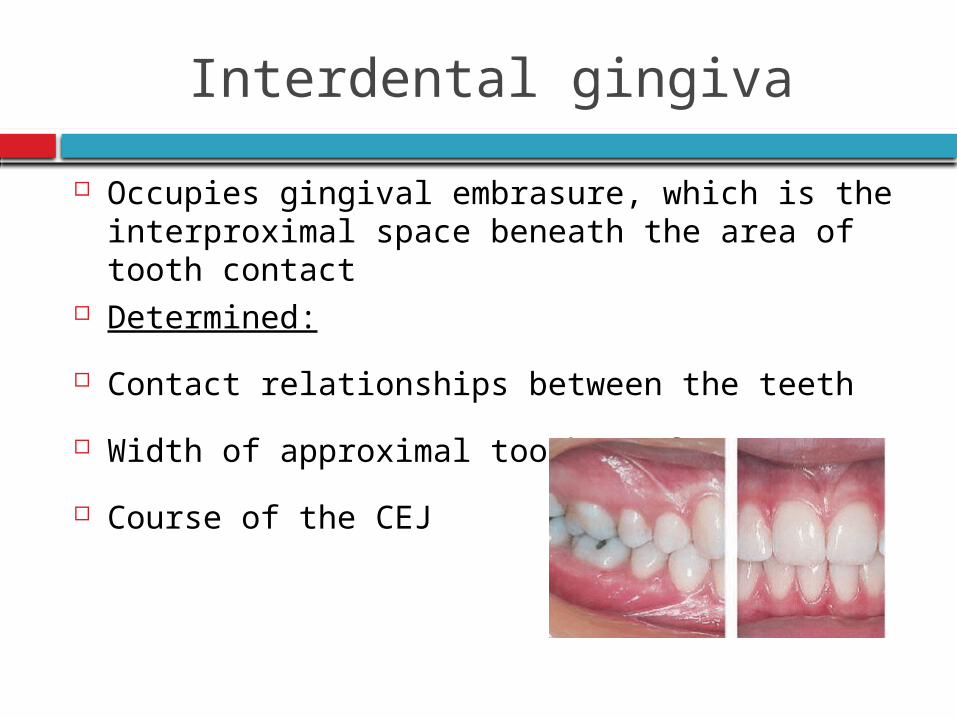
Interdental gingiva
Occupies gingival embrasure, which is the interproximal space beneath the area of tooth contact
Determined:
Contact relationships between the teeth
Width of approximal tooth surfaces
Course of the CEJ
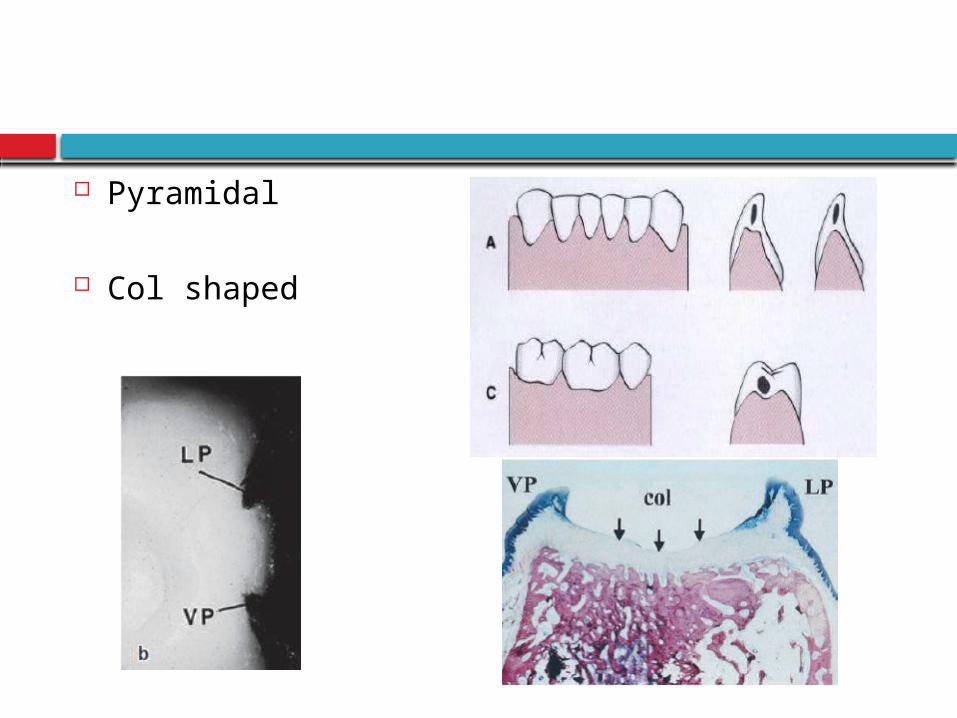
Pyramidal
Col shaped Cohen
MICROSCOPIC FEATURES
Stratified squamous epithelium
Central core of connective tissue
GINGIVAL EPITHELIUM
Function:
Protects deep structures
Mechanical, chemical, water, microbial barrier
Signalling function
General aspects of gingival epithelium biology
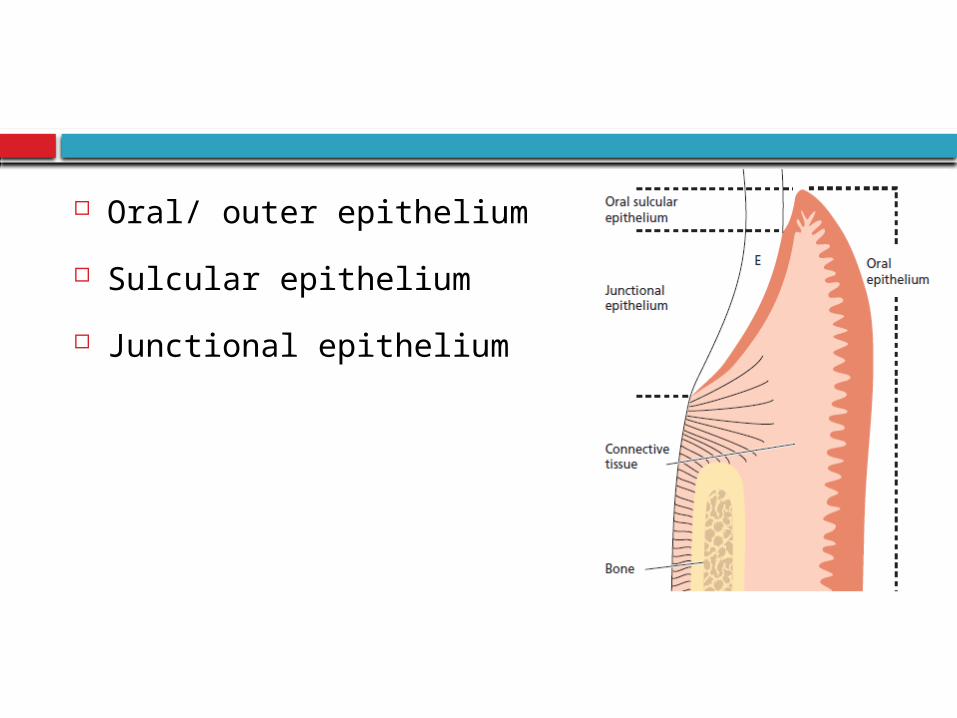
Oral/ outer epithelium
Sulcular epithelium
Junctional epithelium
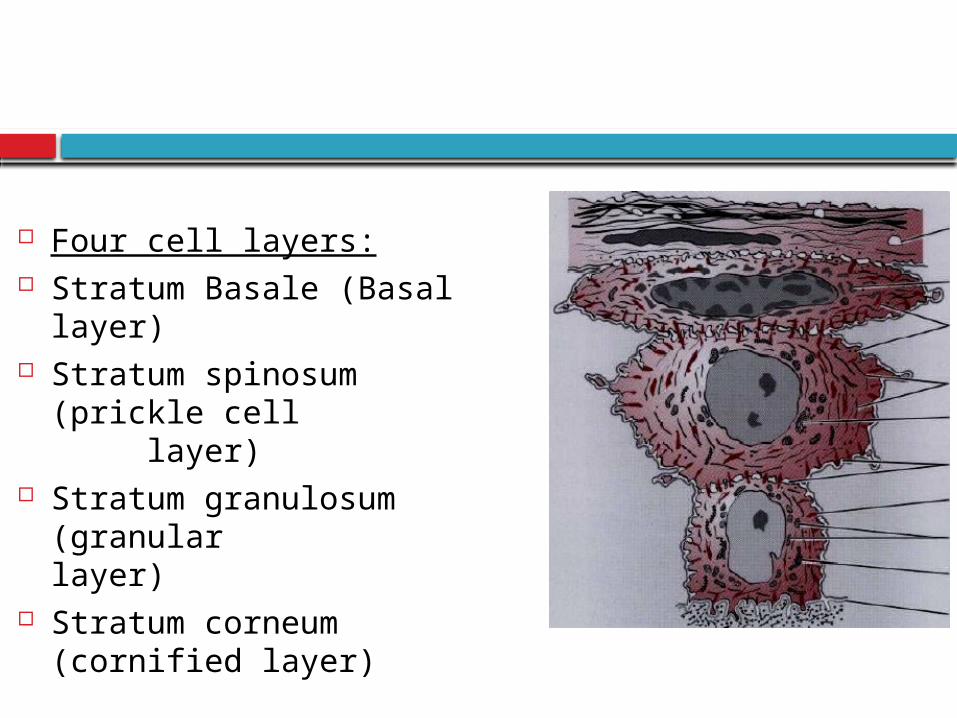
Four cell layers: Stratum Basale (Basal layer) Stratum spinosum (prickle
cell layer)
Stratum granulosum (granular
layer) Stratum corneum (cornified
layer)
Principal cell: keratinocytes
Clear cells / Nonkeratinocytes:
Langerhans cells
Merkels cells
Melanocytes
Inflammatory cells
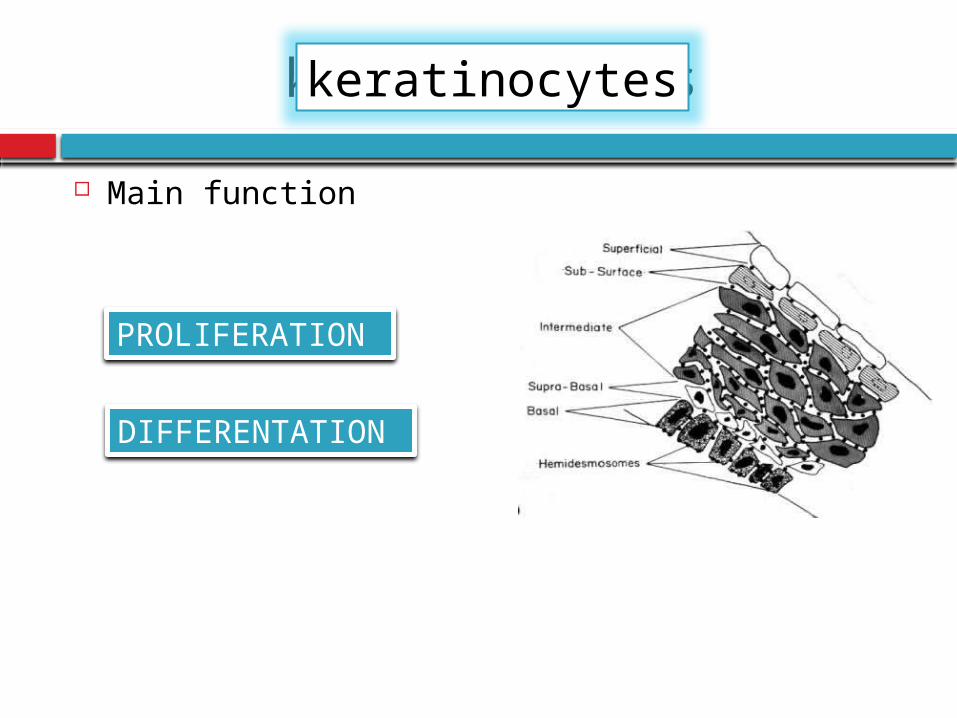
keratinocytes
Main function
PROLIFERATION
DIFFERENTATION
keratinocytes
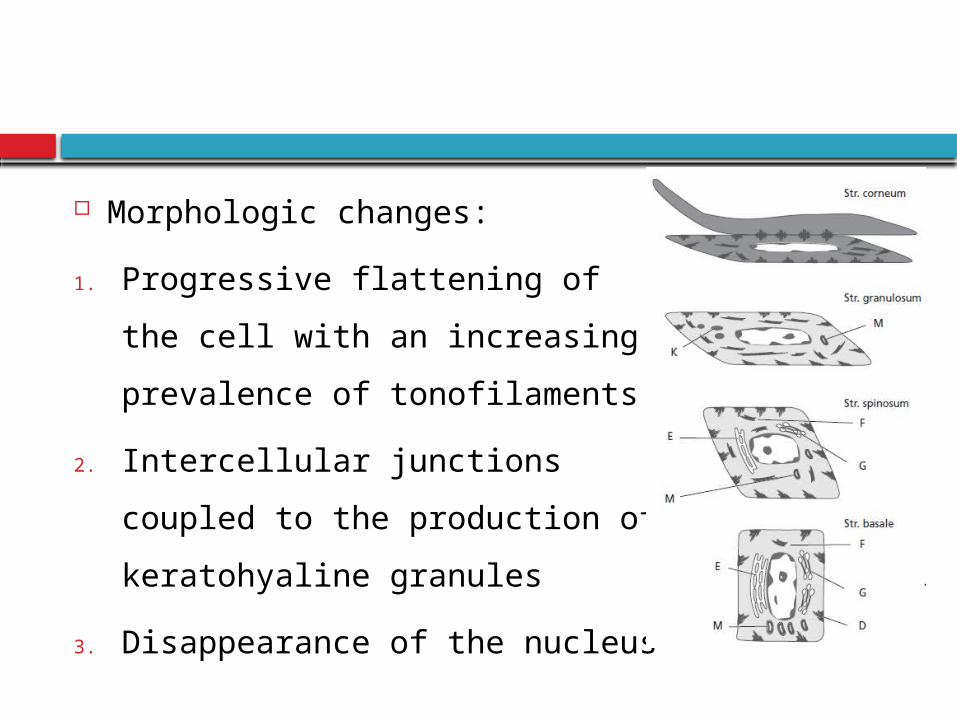
Morphologic changes:
1. Progressive flattening of the cell
with an increasing prevalence of
tonofilaments
2. Intercellular junctions coupled
to the production of
keratohyaline granules
3. Disappearance of the nucleus
Schroeder 1981
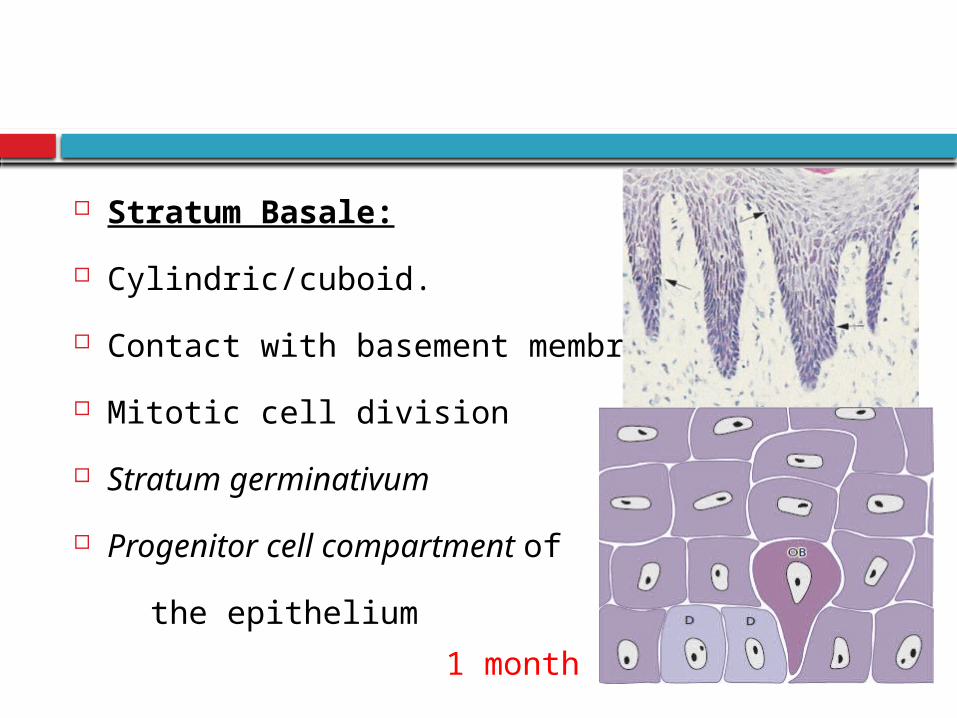
Stratum Basale:
Cylindric/cuboid.
Contact with basement membrane
Mitotic cell division
Stratum germinativum
Progenitor cell compartment of
the epithelium
1 month
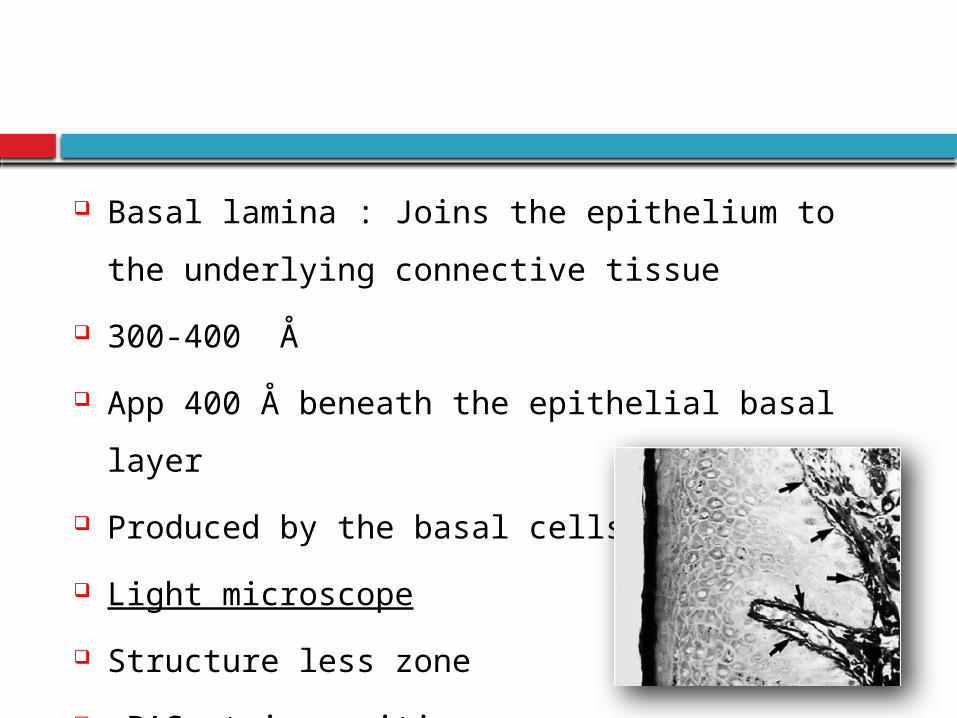
Basal lamina : Joins the epithelium to the
underlying connective tissue
300-400 Å
App 400 Å beneath the epithelial basal layer
Produced by the basal cells
Light microscope
Structure less zone
PAS stain positive
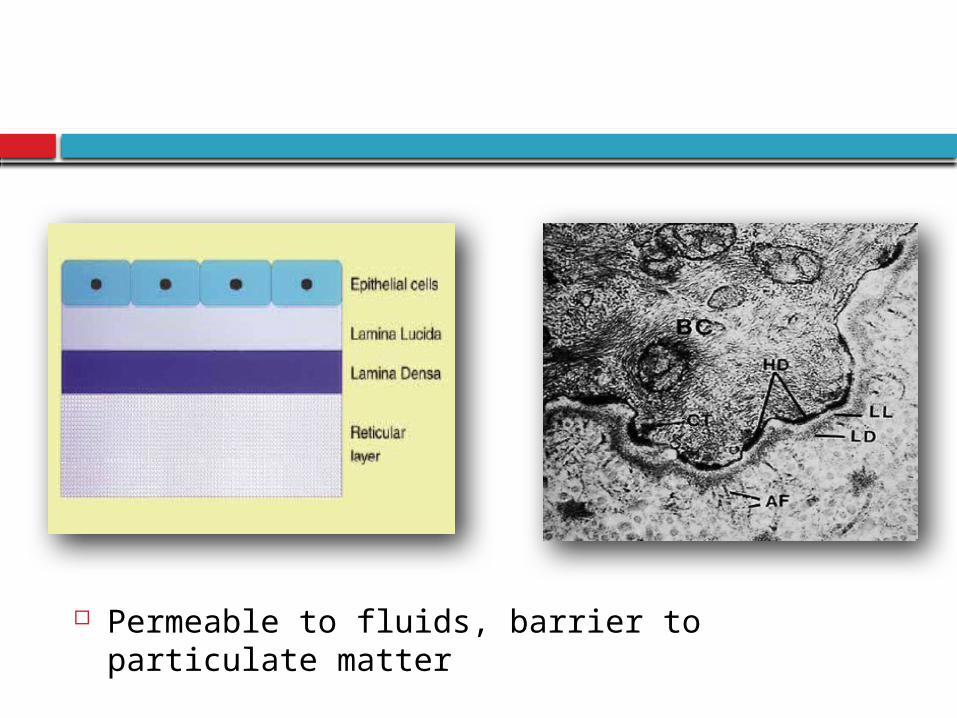
Permeable to fluids, barrier to particulate matter
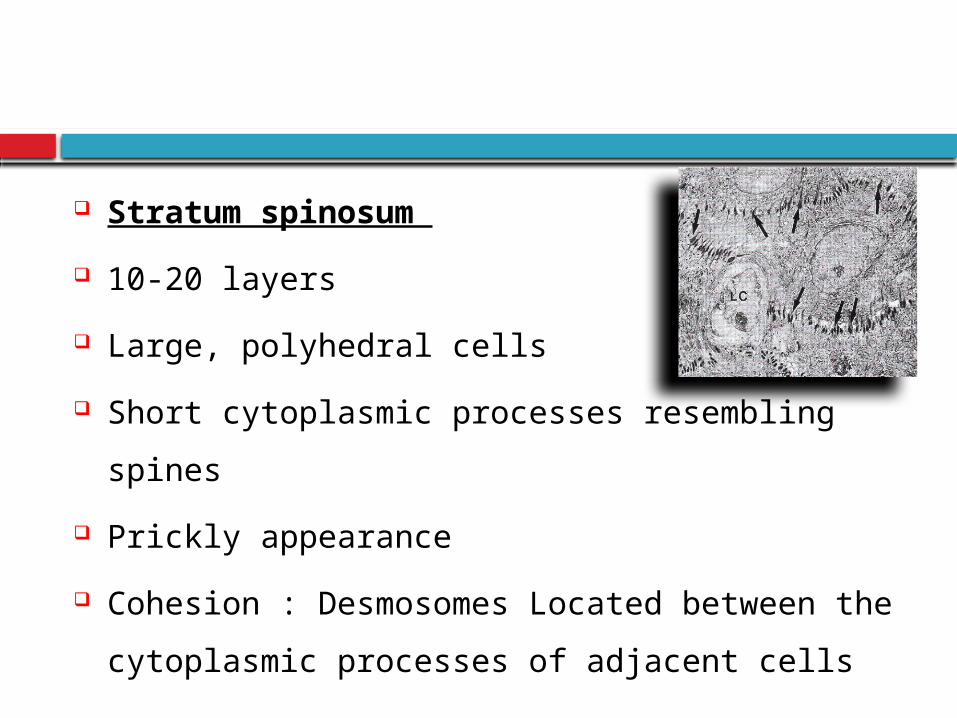
Stratum spinosum
10-20 layers
Large, polyhedral cells
Short cytoplasmic processes resembling spines
Prickly appearance
Cohesion : Desmosomes Located between the
cytoplasmic processes of adjacent cells
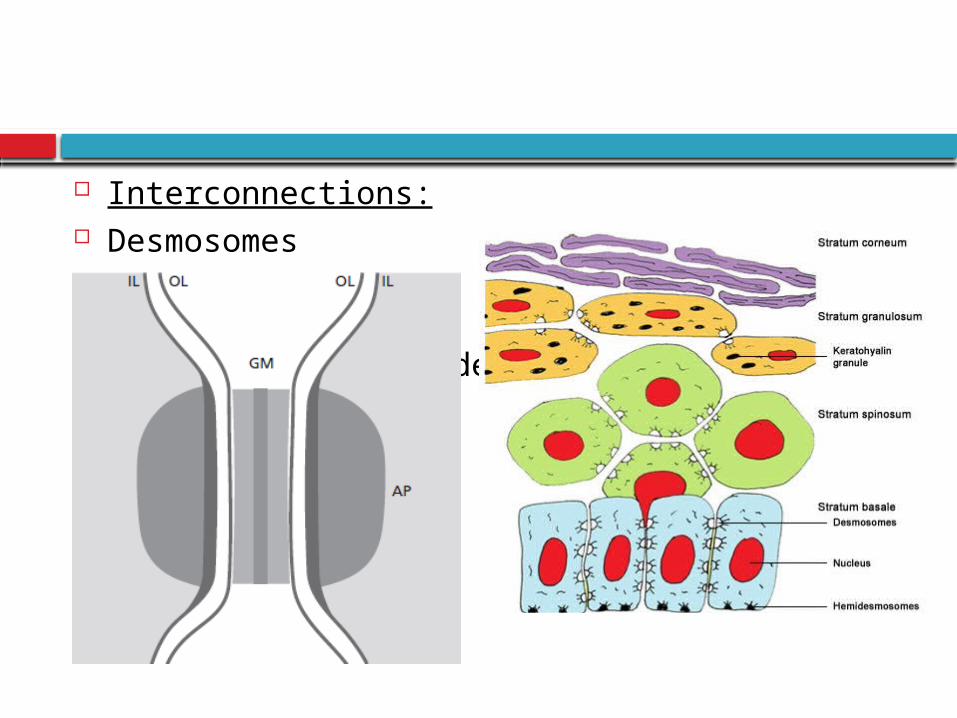
Interconnections: Desmosomes Tight junctions
(Zonae occludens)
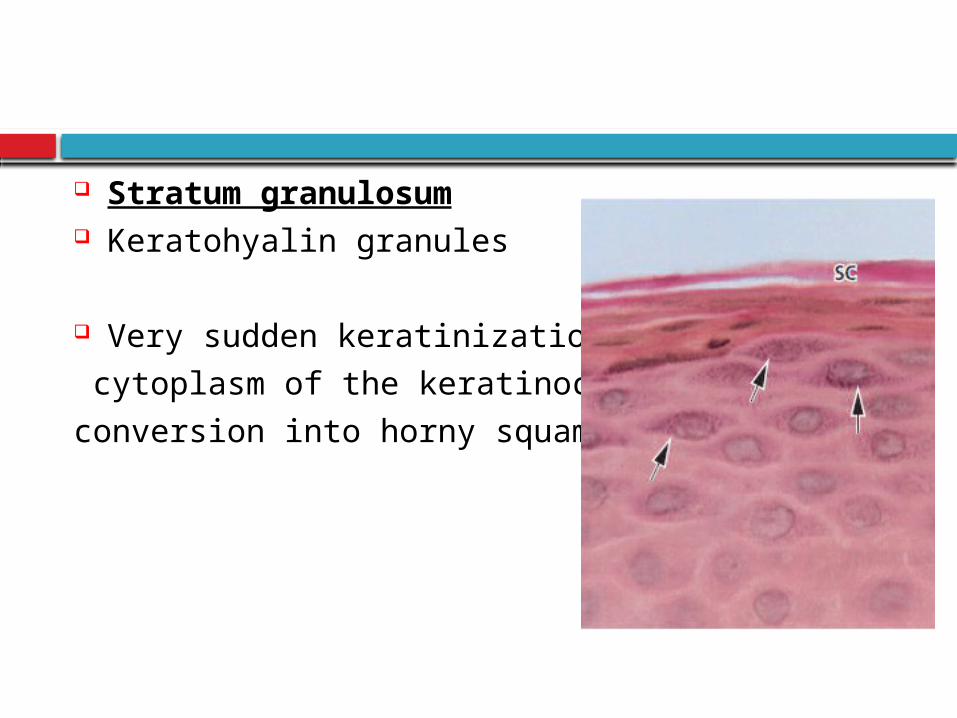
Stratum granulosum Keratohyalin granules
Very sudden keratinization of the
cytoplasm of the keratinocyte &
conversion into horny squame
Stratum corneum
Filled with keratin
Apparatus for protein synthesis & energy
production lost
Complete keratinization Orthokeratinized
Parakeratinized epithelium
Nonkeratinized epithelium
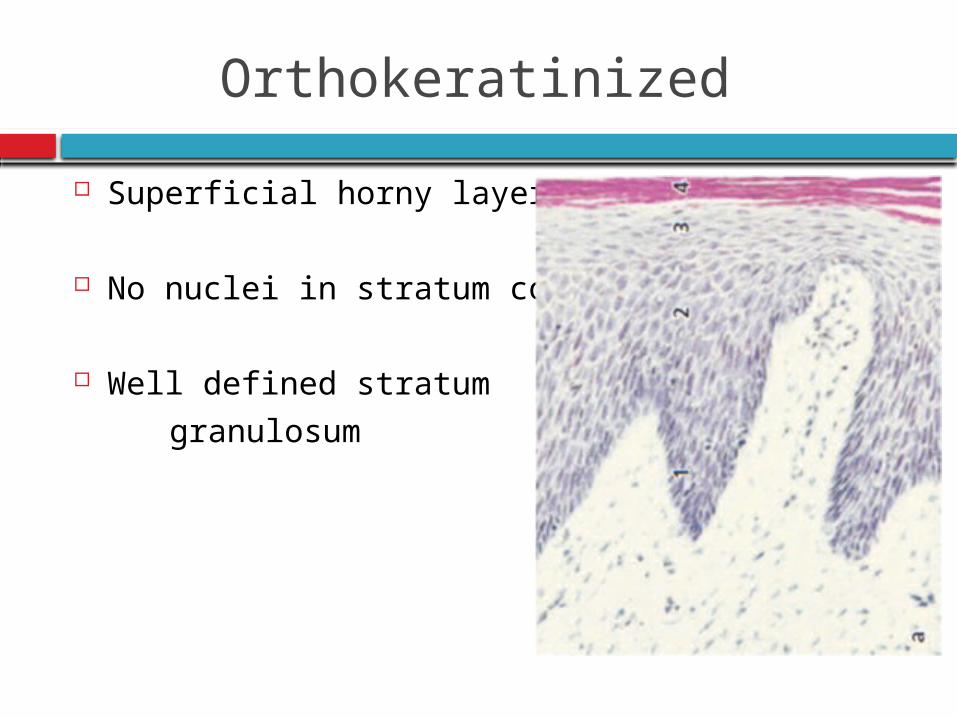
Orthokeratinized
Superficial horny layer
No nuclei in stratum corneum
Well defined stratum
granulosum
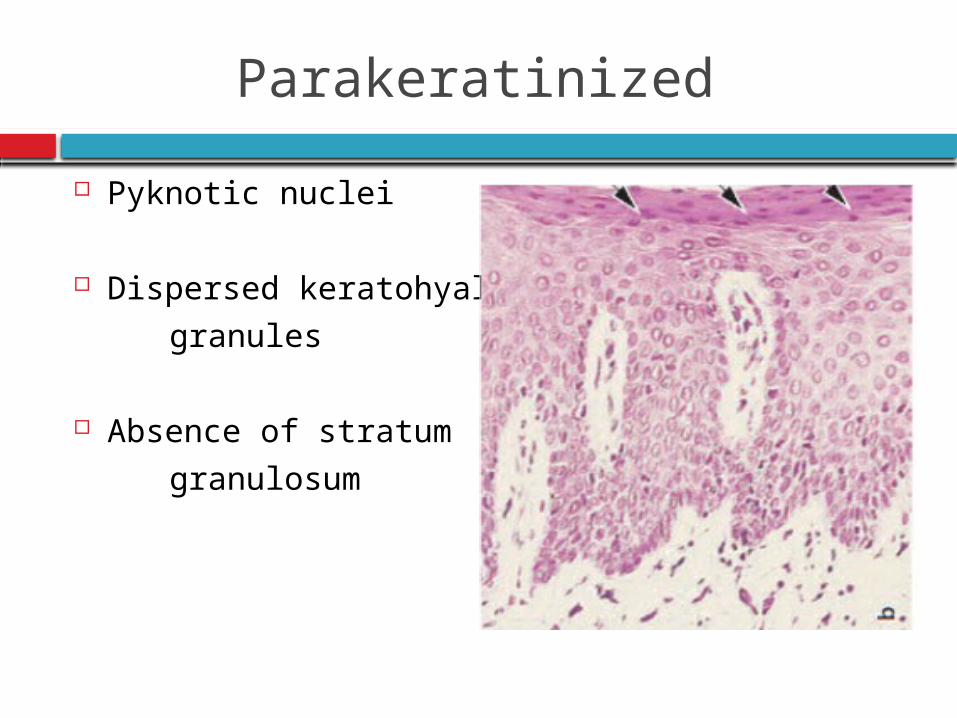
Parakeratinized
Pyknotic nuclei
Dispersed keratohyaline
granules
Absence of stratum
granulosum
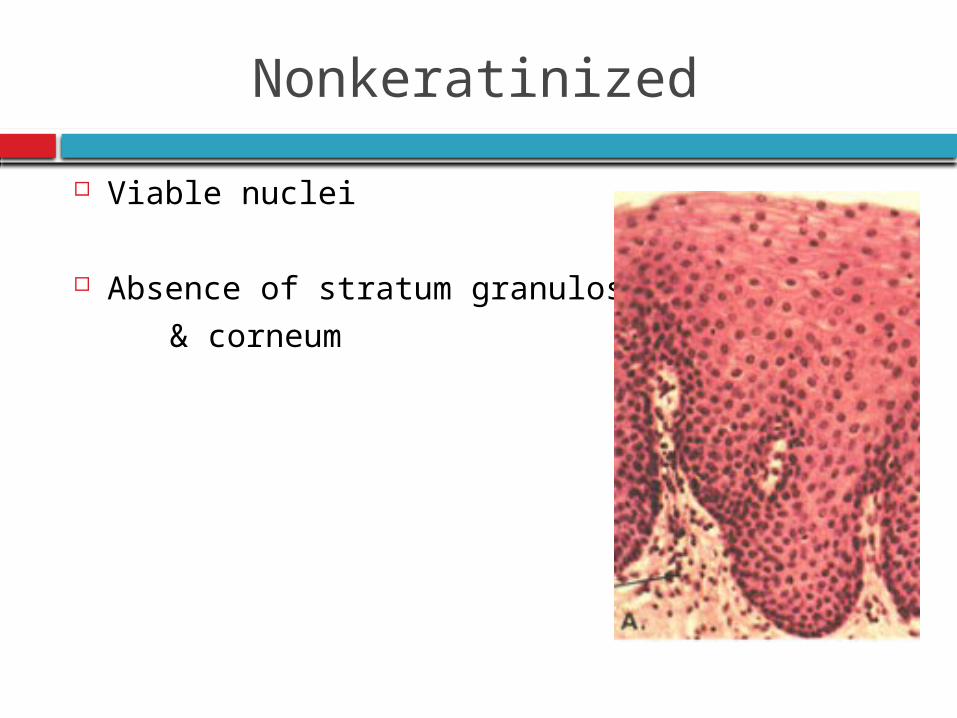
Nonkeratinized
Viable nuclei
Absence of stratum granulosum
& corneum
keratinization
Immunohistochemistry, Gel electrophoresis,
Immunoblot technique
Keratin proteins different polypeptide subunits
Basal cells: K19 (40 KD)
Stratum corneum: K1 (68 KD)
Other proteins: Keratolinin Involucrin Filaggrin
In sudden transition Keratohyalin granules Filaggrin Matrix of Corneocyte
Precursors of chemical resistant structure- EnvelopePrecursors packed in keratohyaline granules
Cytoplasmic organelles: Deeper strata
Numerous mitochondria
Succinic dehydrogenase
Nicotineamide-adenine dinucleotide
Cytochrome oxidase
Active Tricarboxyliccycle
Activity towards cell surface: Pentose shunt Glucose-6-phosphatase
Ribonucleic acid (RNA)
Synthesis of keratinization proteins
Uppermost cells: Stratum spinosum
Keratinosomes/Odland bodies
Acid phosphatase:Enzyme involved in the
destruction of organelle membranes
Degree of keratinization
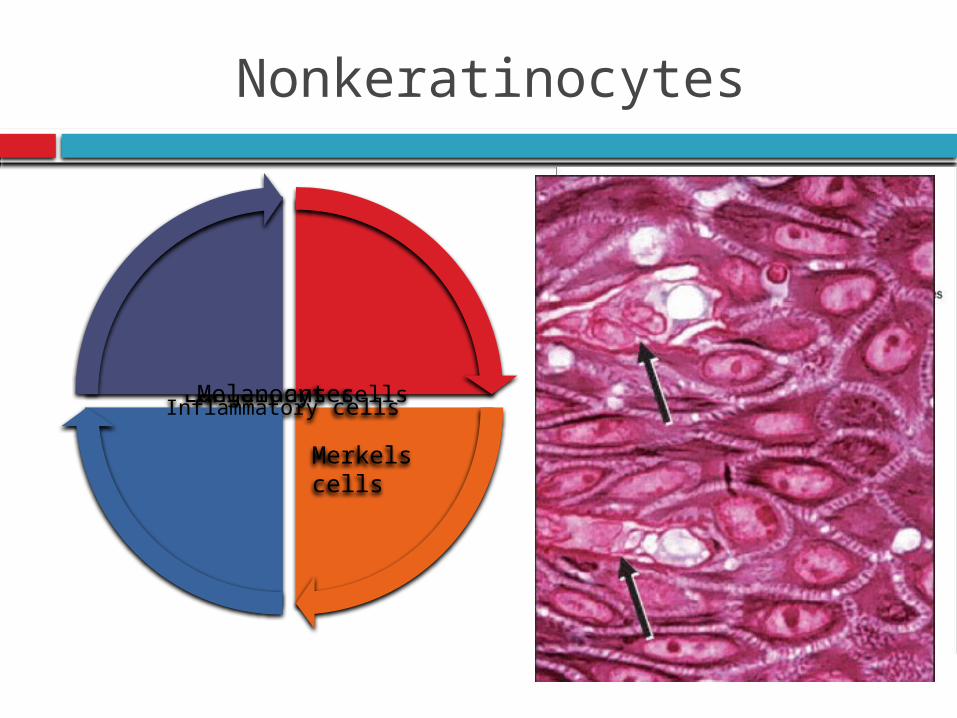
Nonkeratinocytes
Langerhans cells
Inflammatory cells
Melanocytes
Merkels cells
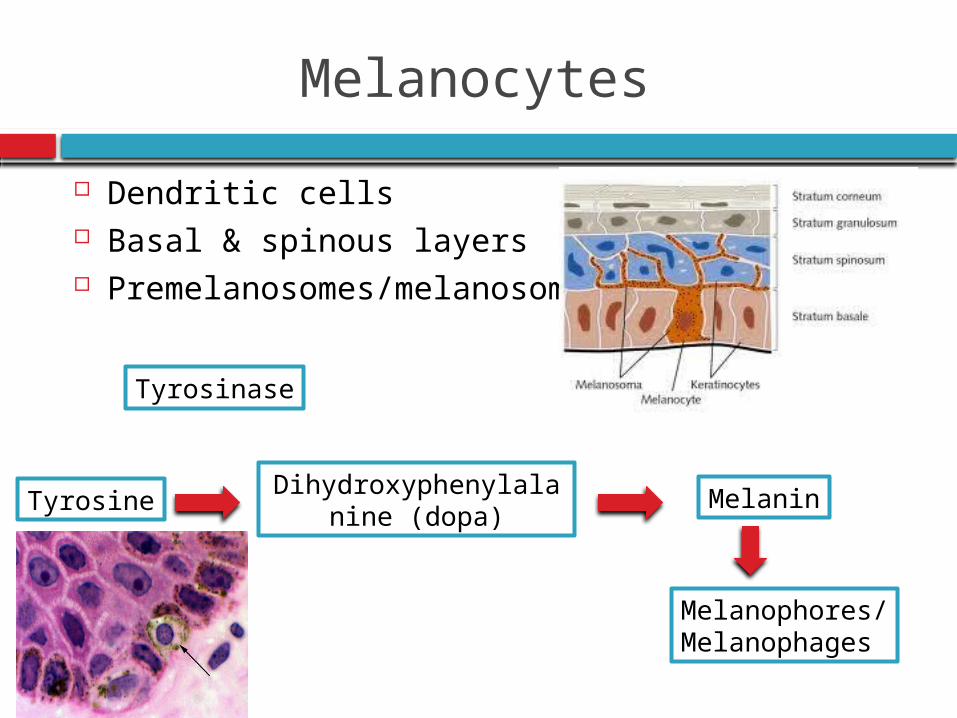
Melanocytes
Dendritic cells Basal & spinous layers Premelanosomes/melanosomes
Tyrosine
Tyrosinase
MelaninDihydroxyphenylalanine (dopa)
Melanophores/Melanophages
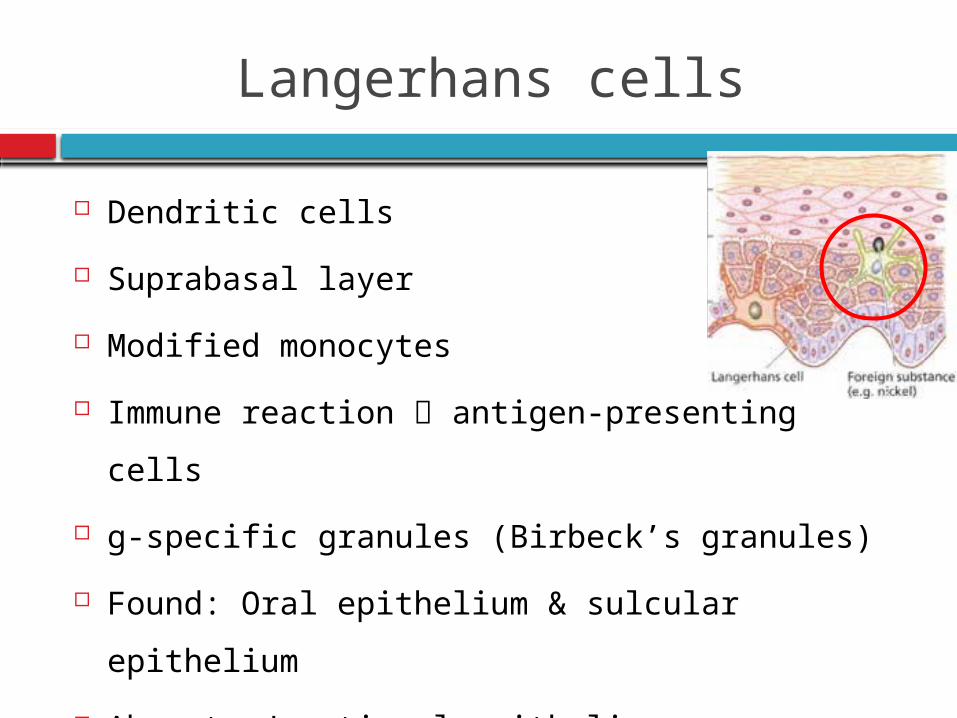
Langerhans cells
Dendritic cells
Suprabasal layer
Modified monocytes
Immune reaction antigen-presenting cells
g-specific granules (Birbeck’s granules)
Found: Oral epithelium & sulcular epithelium
Absent: Junctional epithelium
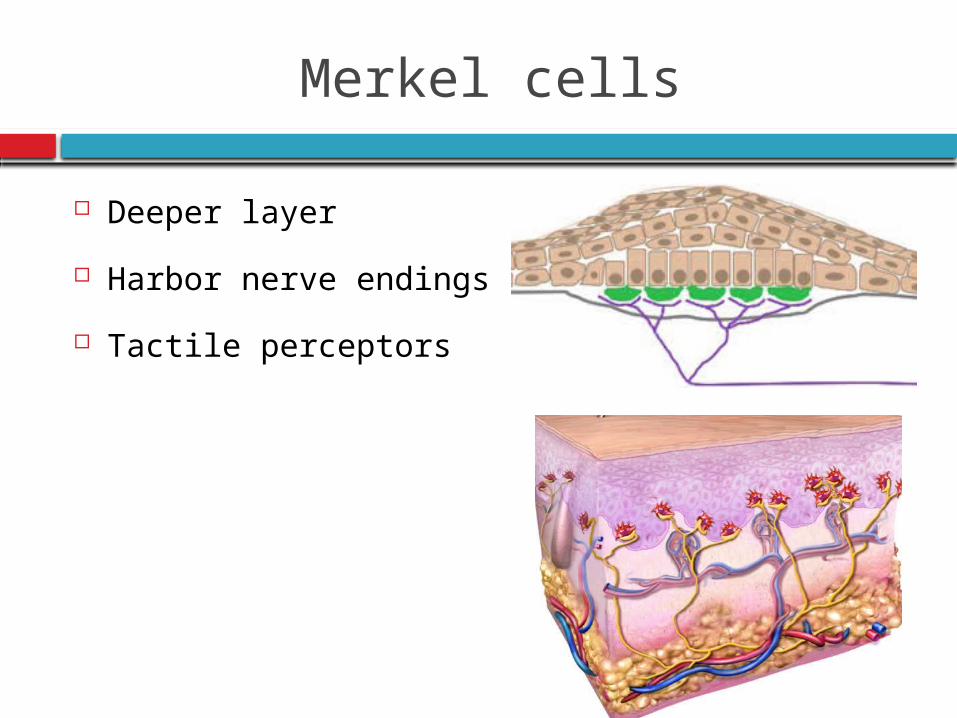
Merkel cells
Deeper layer
Harbor nerve endings
Tactile perceptors
Inflammatory cells
Clinical normal areas of mucosa
Lymphocytes : Most frequent
Associated with langerhans cells
Polymorphonuclear leukocytes
Mast cells
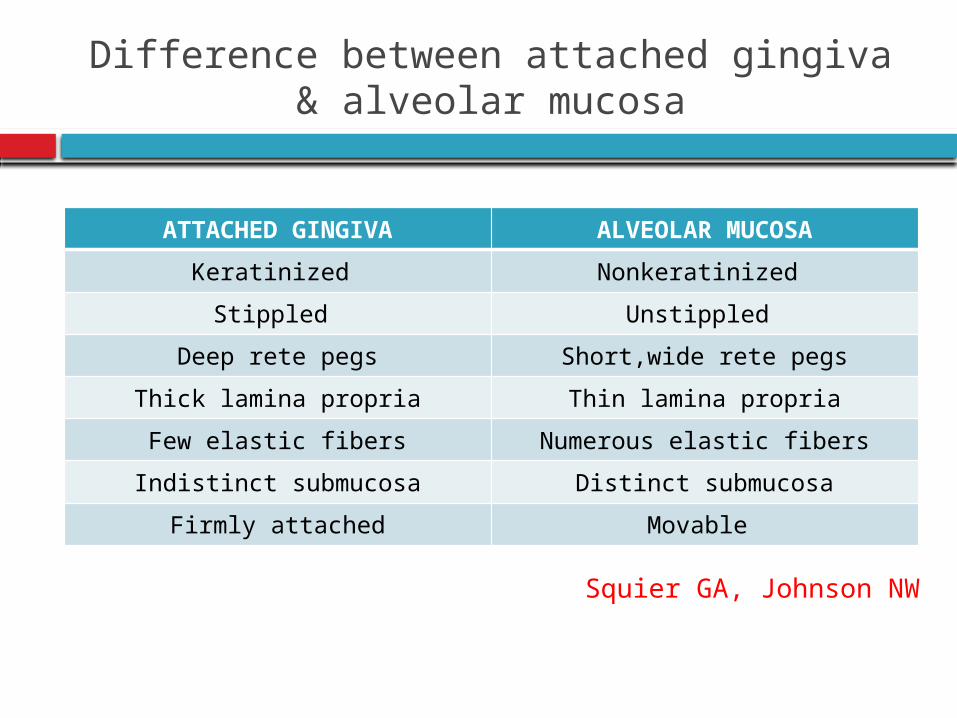
Difference between attached gingiva & alveolar mucosa
ATTACHED GINGIVA ALVEOLAR MUCOSA
Keratinized Nonkeratinized
Stippled Unstippled
Deep rete pegs Short,wide rete pegs
Thick lamina propria Thin lamina propria
Few elastic fibers Numerous elastic fibers
Indistinct submucosa Distinct submucosa
Firmly attached Movable
Squier GA, Johnson NW
Extracellular matrix
Glycoproteins, lipids, water Proteoglycans: Hyaluronan, decorin, syndecan CD 44 – cell surface
Hakkinen L Cell adhesion molecules: ICAM-1, β1 integrin family
Cawford Serves: Cell adhesion Adhesion to tooth surface & basement
membrane Diffusion of water, nutrients & toxic materials
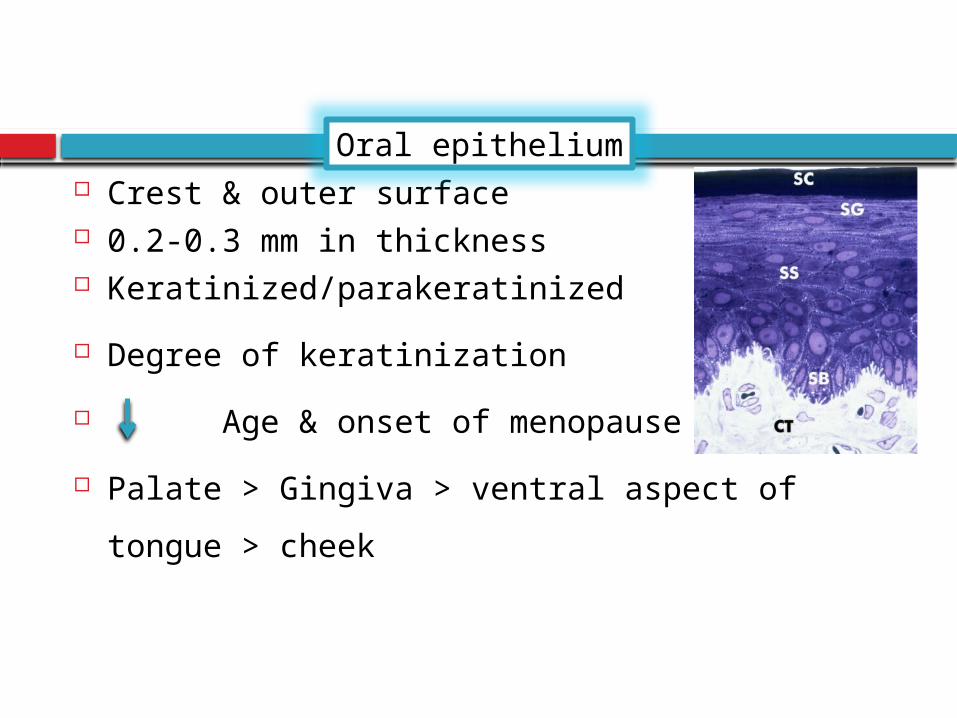
Crest & outer surface 0.2-0.3 mm in thickness Keratinized/parakeratinized
Degree of keratinization
Age & onset of menopause
Palate > Gingiva > ventral aspect of tongue >
cheek
Oral epithelium
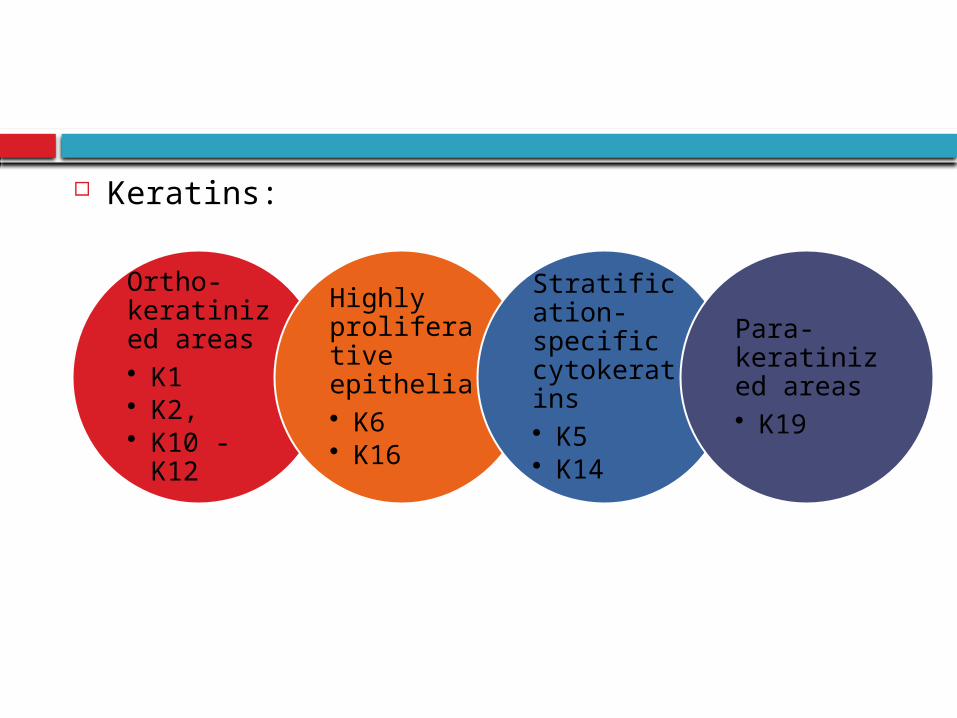
Keratins:
Ortho-keratinized areas• K1• K2, • K10 - K12
Highly proliferative epithelia• K6• K16
Stratification-specific cytokeratins• K5• K14
Para-keratinized areas• K19
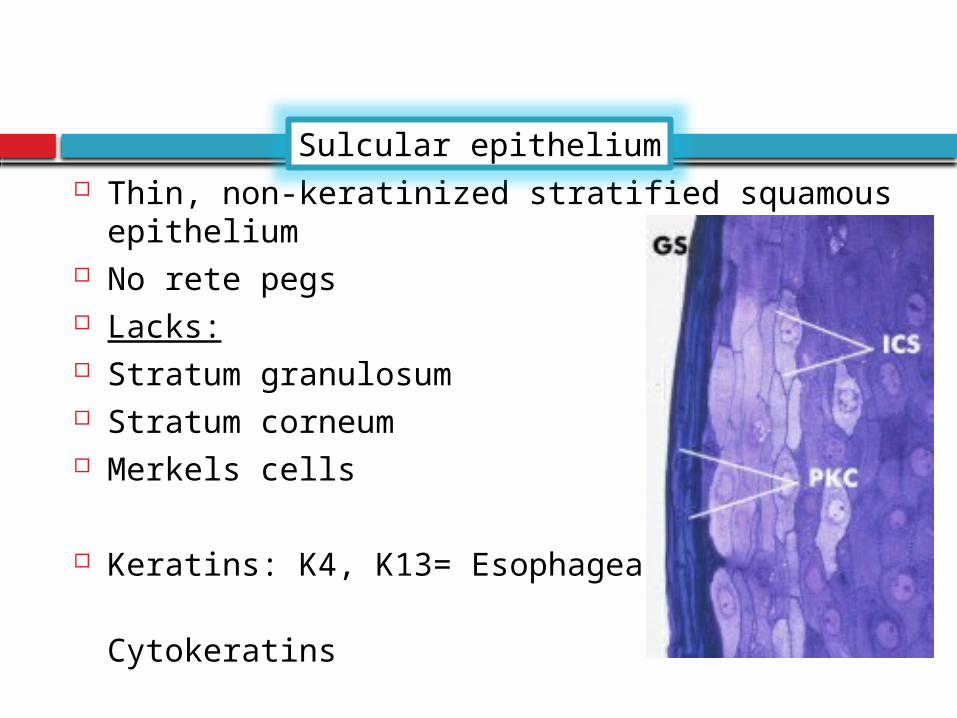
Thin, non-keratinized stratified squamous epithelium
No rete pegs Lacks: Stratum granulosum Stratum corneum Merkels cells
Keratins: K4, K13= Esophageal-type
Cytokeratins
Sulcular epithelium
Enzymes: low degree of activity Acid phosphatase staining negative Semipermeable membrane
Potential to keratinize: It is reflected & exposed to oral cavity Bral &
Caffesse Absence of bacterial flora
Caffesse
The junctional epithelium is the epithelial component of the dentogingival unit that is in contact with the tooth surface. The innermost cells of the JE form & maintain a tight seal against the mineralized tooth surface, the so called epithelial attachment
Schroeder & Listgarten, 1977
Collar-like band of stratified squamous nonkeratinizing epithelium
Glickman
Junctional epithelium
Junctional epithelium
Gingival fibers
Dentogingival unit
Current concepts of dentogingival junction
Upto 1912 Min information regarding junction between tooth & epithelium
Attachment = CT fibers inserting into cementum & bone
GV Black 1915 Presence of subgingival space extending upto CEJ under a loose fitting gingiva
Gottlieb 1921 Presence of a firm attachment (Organic union) between gingiva & tooth = Epithelial attachment /epithelansatz
Orban 1931 during eruption REE forms epithelial attachment
Waerhaug 1952 Gingiva seperated from tooth by a capillary space forming a “Epithelial cuff”
Epithelial attachment Epithelial cuff
Orban 1956 Agreed to both concepts & gave term
“Attached epithelial cuff”
Stern 1962 Demonstrated the DGJ in rat incisors consisting of Basal Lamina & Hemidesmosomes
The above concepts were incorrect
Junctional Epithelium, a tissue capable of forming & renewing itself continuously throught life
Term JE = Anderson & Stern in 1966
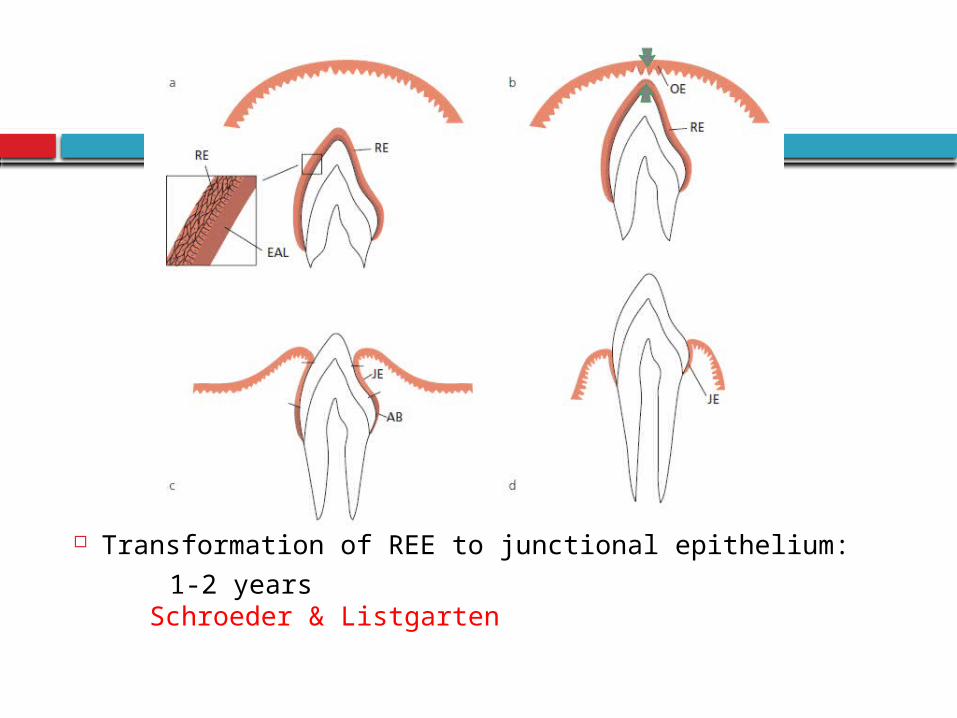
Transformation of REE to junctional epithelium:
1-2 years Schroeder & Listgarten
Tencate 1966
Secondary junctional epithelium
Undifferentiated basal cells originating from oral gingival epithelium
Primary junctional epithelium
Reduced enamel epithelium
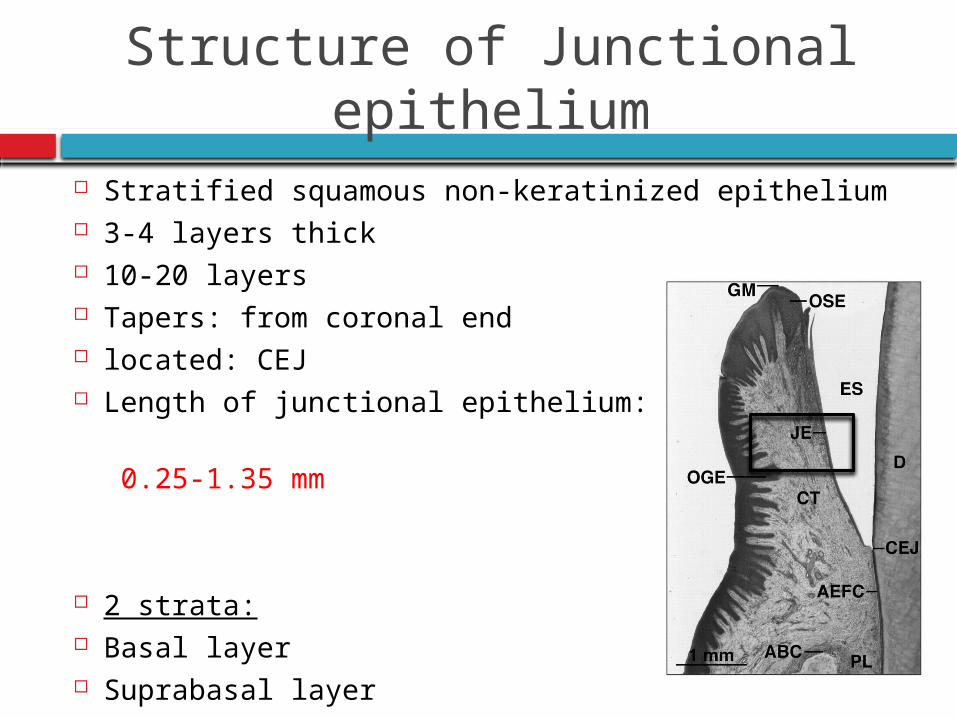
Structure of Junctional epithelium
Stratified squamous non-keratinized epithelium 3-4 layers thick 10-20 layers Tapers: from coronal end located: CEJ Length of junctional epithelium:
0.25-1.35 mm
2 strata: Basal layer Suprabasal layer
Basal cells = face gingival CT
Suprabasal cells = tooth surface
also called as DAT cells (Directly Attached to
Tooth)
Salonen 1989
Lymphocytes & macrophages
Sensory nerve fibers
Byers and Holland 1977, Maeda et
al,1994
Keratins: K19
Stratification specific: K5 & K14
Lack of expression:
Morgan et al : Junctional area is the only stratified
nonkeratinized epithelium in the oral cavity that
does not synthesize K4 or K13
Lack of K6 & K16 : Though turnover of the cells is
very high
Interconnections
Few desmosomes only Occasional gap junctions
Schroeder & Listgarten, 1977 Saito et al, 1981 Hashimoto et al, 1986
Wide fluid-filled intercellular spaces
Schroeder& Münzel-Pedrazzoli, 1970
3 Zones: Apical zone germinative characteristics
Middle zone higher density of hemidesmosomes
role in adhesion
Coronal zone numerous intercellular space
increased permeability
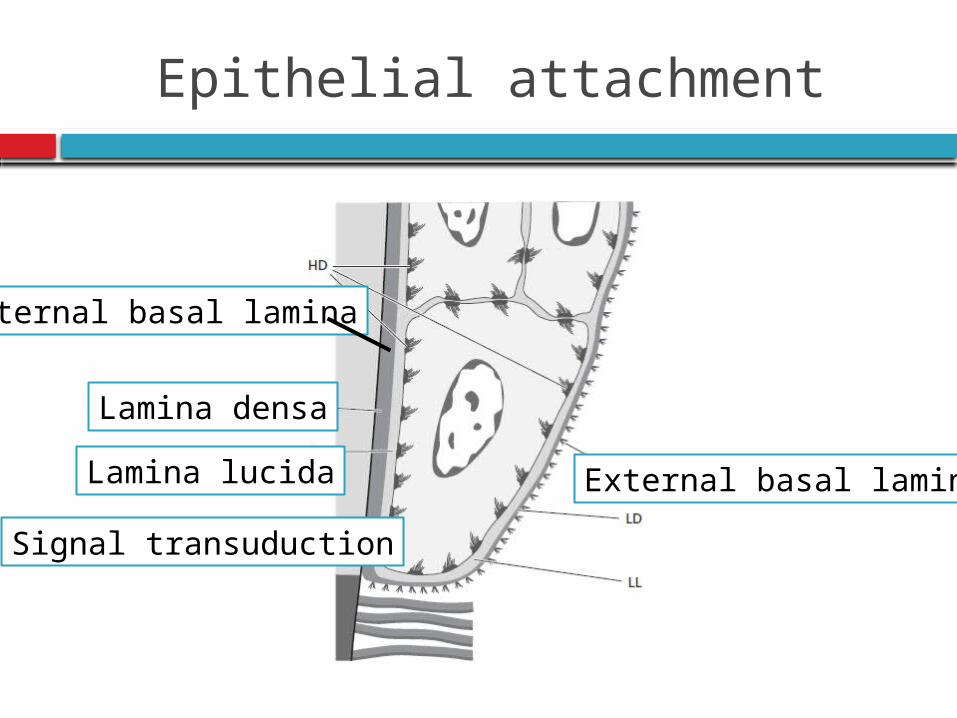
Epithelial attachment
Internal basal lamina
External basal laminaLamina lucida
Lamina densa
Signal transuduction
Histochemical evidence Neutral
polysaccharide
Thonard JC
Basal lamina:
Laminin: similar to endothelial & epithelial cells
Lack type IV & VII collagen, perlecan,lamina
fibroreticularis. Salonen &
Santti 1985
Dynamics of junctional epithelium
Turnover is very high protective & regeneration
Earlier thought epithelial cells facing external
basal lamina divide rapidly
Evidence DAT cells high mitotic activity
DAT cells Role in tissue dynamics & reparative
capacity of JE
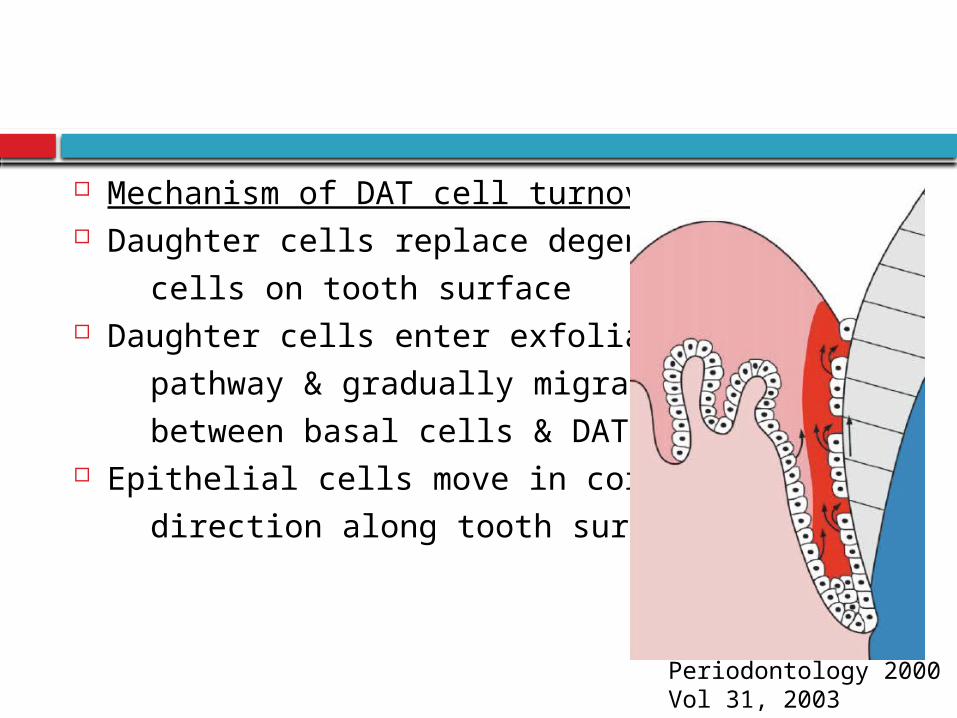
Mechanism of DAT cell turnover: Daughter cells replace degenerating
cells on tooth surface Daughter cells enter exfoliation
pathway & gradually migrate coronally
between basal cells & DAT cells Epithelial cells move in coronal
direction along tooth surface
Periodontology 2000Vol 31, 2003
Structural & functional features:
Firm attachment: epithelial barrier
Immunologic host defense: Gingival fluid,
inflammatory cells
Rapid cell turnover Endocytic capacity equal to that of macrophages
and neutrophils
Cho.Garant.2000
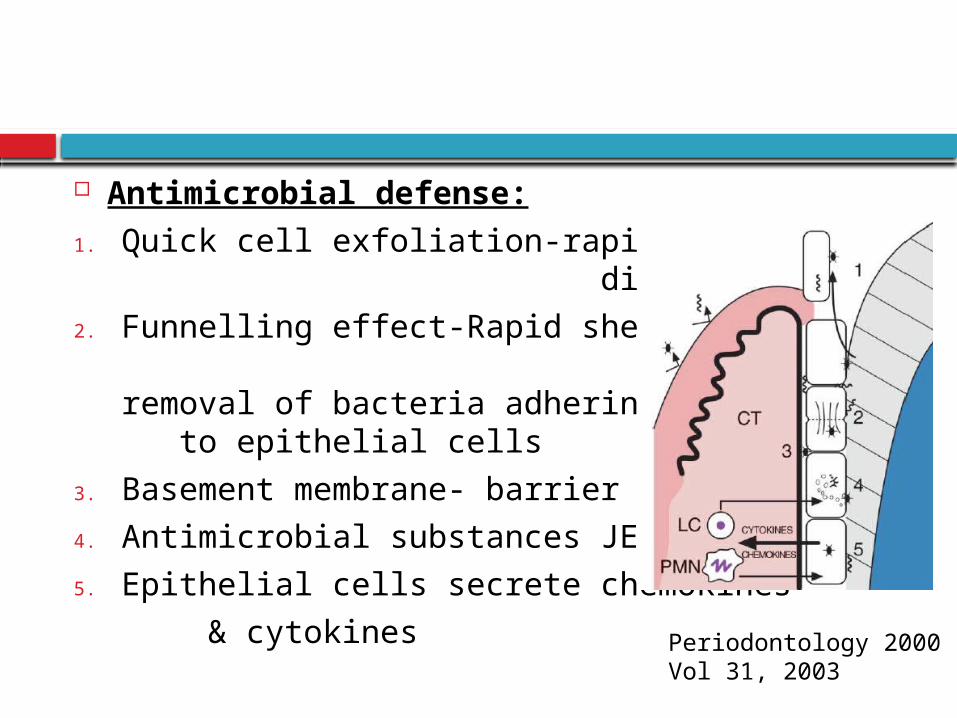
Antimicrobial defense:
1. Quick cell exfoliation-rapid cell division
2. Funnelling effect-Rapid shedding & effective removal of bacteria adhering to epithelial cells
3. Basement membrane- barrier
4. Antimicrobial substances JE cells
5. Epithelial cells secrete chemokines
& cytokinesPeriodontology 2000Vol 31, 2003
Renewal of Gingival epithelium
Mitotic activity: 24 hr periodicity
Highest Morning
Nonkeratinized areas
Gingivitis
Lowest Evening
New cell formatio
n
Shedding of old
cells
Cell turnover time:
Palate, tongue, cheeks: 5-6 days
Gingiva: 10-12 days
Junctional epithelium: 1-6 days
Beagrie G S
Epithelial repair & regeneration
Gingivectomy & incisional wounds:
Undamaged epithelial cells from wound margin, migrates within hours of
injury
Migrate over exposed connective tissue
New hemidesmosomes are formed
1-2 days = epithelial surface is 2-3 cell thick & str basale forms
By day 5 = wound is fully covered
By day 7 = epithelium has matured & new str corneum formation
Green RJ
et al
Periodontal flaps: heals long junctional epitheliumStahl SS et al
Dental cuticular structure
A thin, acellular structure with a homogeneous matrix, sometimes enclosed within clearly demarcated, linear borders
ListgartenCoatings of developmental
origin
Formed as part of tooth development
Reduced enamel epithelium
Coronal cementum
Dental cuticle
Acquired coatings
Exogenous origin
Saliva
Bacteria
Calculus
Surface stains
Gingival crevicular fluid
Seeps through the thin sulcular epithelium
Cleanse material from the sulcus
Improve adhesion of the epithelium to the tooth
Antimicrobial properties
Antibody activity

GINGIVA
CONTENTS Introduction Macroscopic features Microscopic features
Gingival epithelium
Oral epithelium
Sulcular epithelium
Junctional epithelium Renewal of gingival epithelium Cuticular structures Gingival crevicular fluid Gingival connective tissue Gingival fibres Blood supply, nerve supply and lymphatics Correlation of clinical & microscopic features Age changes
Gingival connective tissue
Collagen fibers 60%
Fibroblast 5%
Vessels, nerves & matrix 35%
CT lamina propria
1. Papillary layer
2. Reticular layer
Cellular Extracellular
• Fibroblasts
•Mast cells
•Macrophages
•Inflammatory cells
• Fibers
•Ground substance
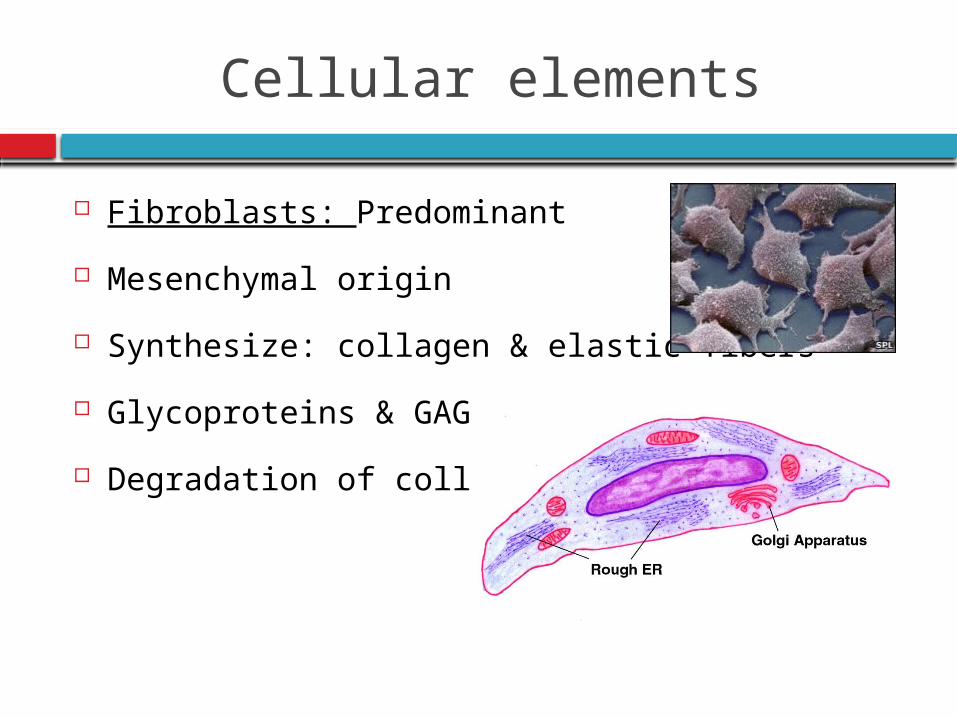
Cellular elements
Fibroblasts: Predominant
Mesenchymal origin
Synthesize: collagen & elastic fibers
Glycoproteins & GAG
Degradation of collagen
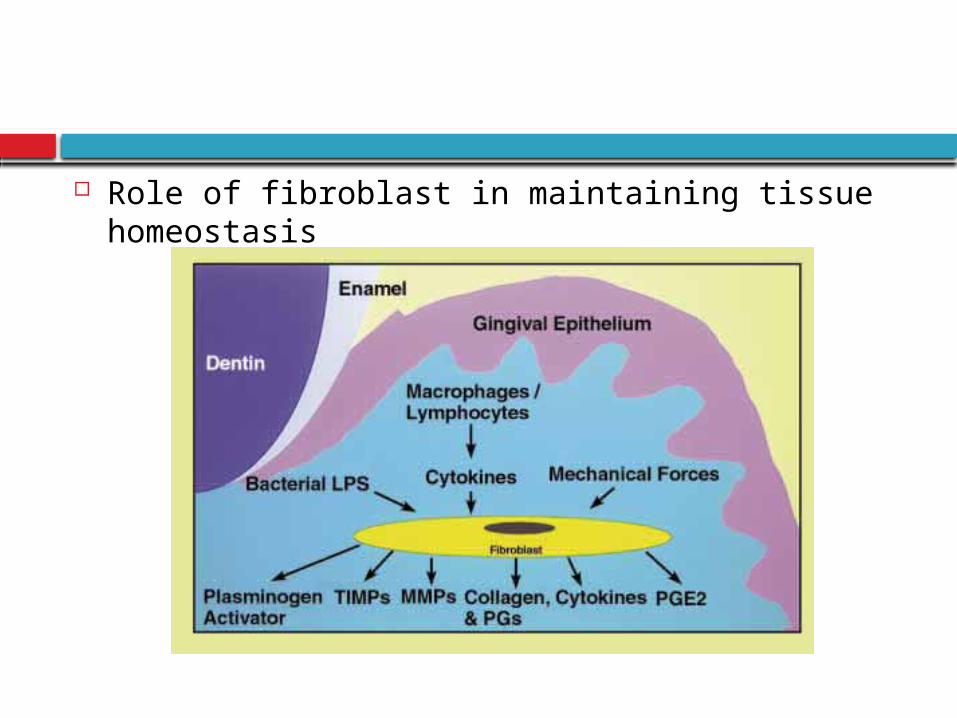
Role of fibroblast in maintaining tissue homeostasis
Mast cells:
Numerous, located perivascular region
Vasoactive substances:
Histamine
Heparin
Proteolytic enzymes
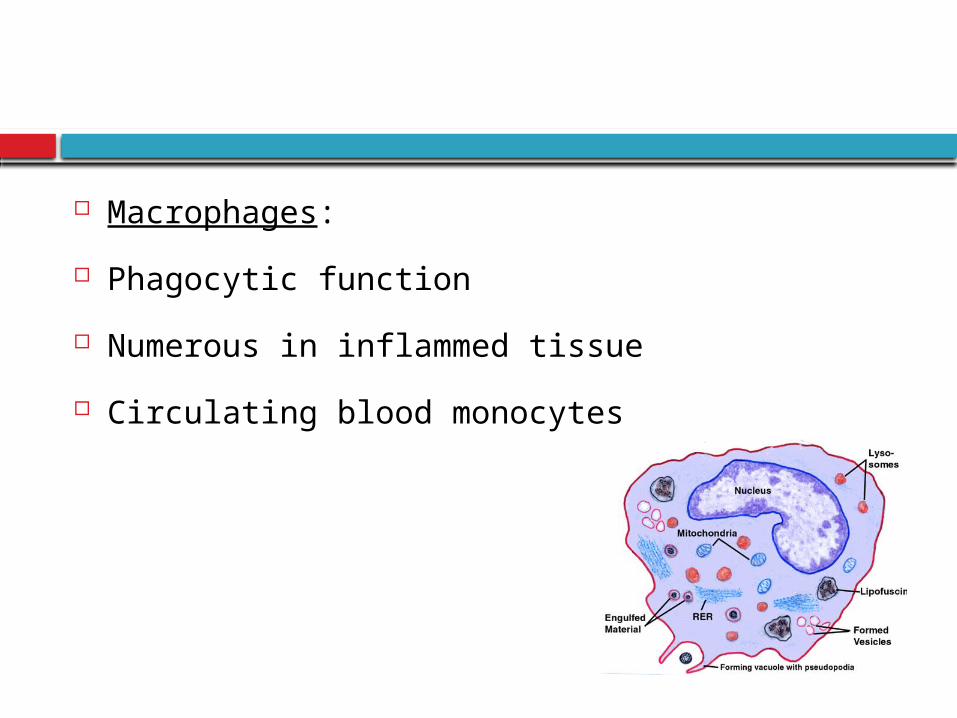
Macrophages:
Phagocytic function
Numerous in inflammed tissue
Circulating blood monocytes
Inflammatory cells:
Polymorphonuclear leukocytes
Lymphocytes
Plasma cells
Clinically normal gingiva : Small foci of plasma
cell & lymphocytes : base of the sulcus
Neutrophils : High numbers in gingival
connective tissue & sulcus
Recently erupted teeth in children : Area below
the junctional epithelium of healthy gingiva : T-
lymphocytes Early defense recognition system
As time elapses : B-lymphocytes & plasma cells
Specific antibodies against already recognized
antigens, always present in the sulcus of
clinically normal gingiva
Fibers
Fibers
Collagen
Reticulin Oxytalan
Elastic
Collagen fibers
Predominate
Type I collagen
Cross banding 700 Å
Fibroblast
Cementoblasts
Osteoblasts
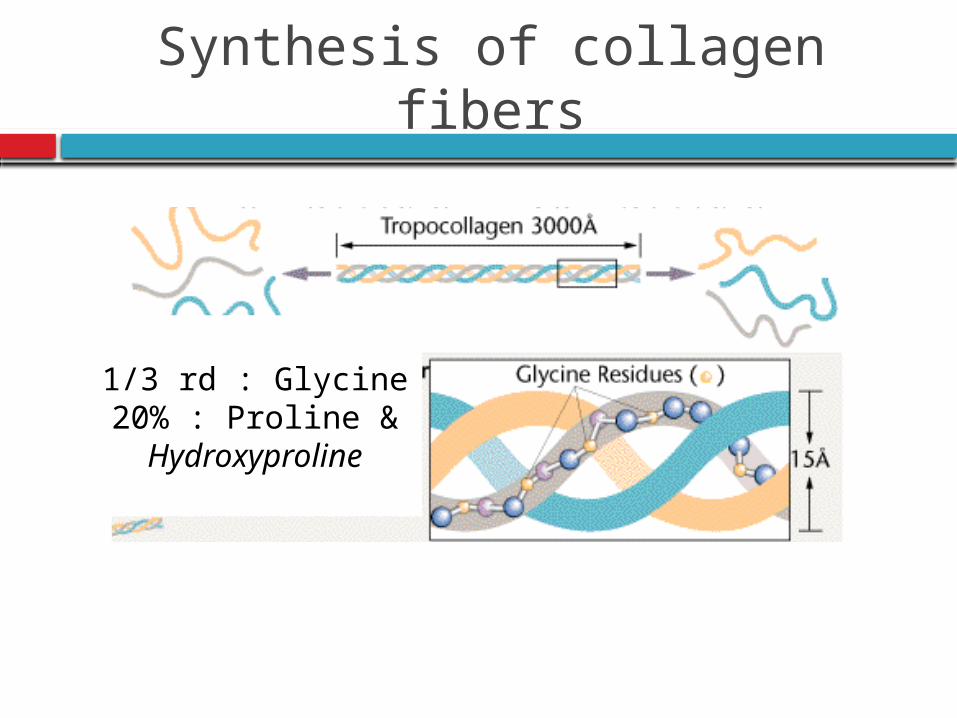
Synthesis of collagen fibers
1/3 rd : Glycine 20% : Proline & Hydroxyproline
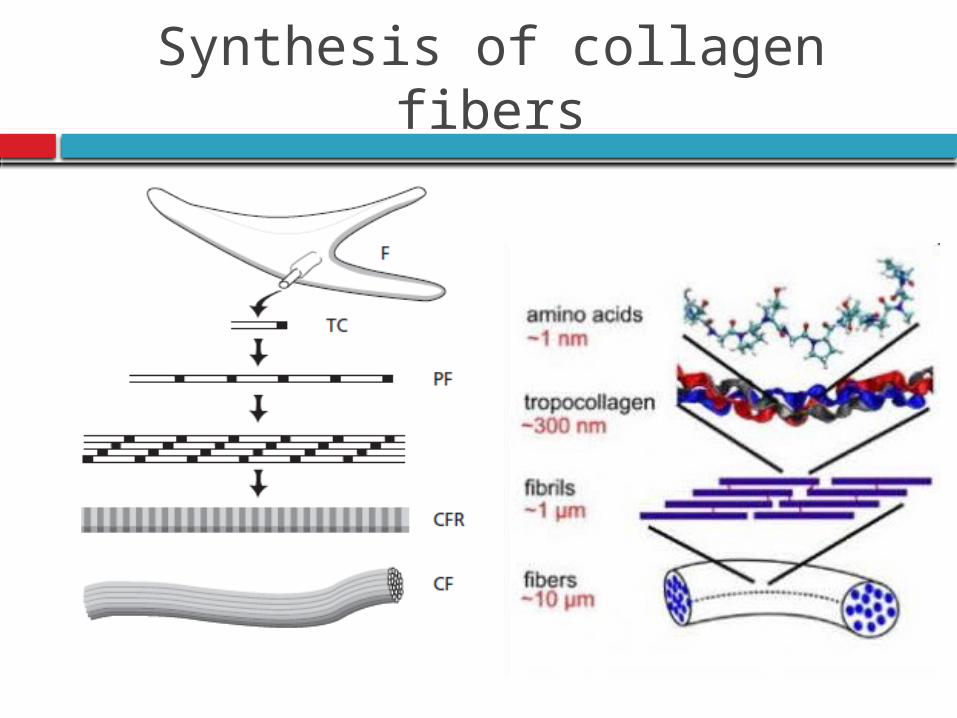
Synthesis of collagen fibers
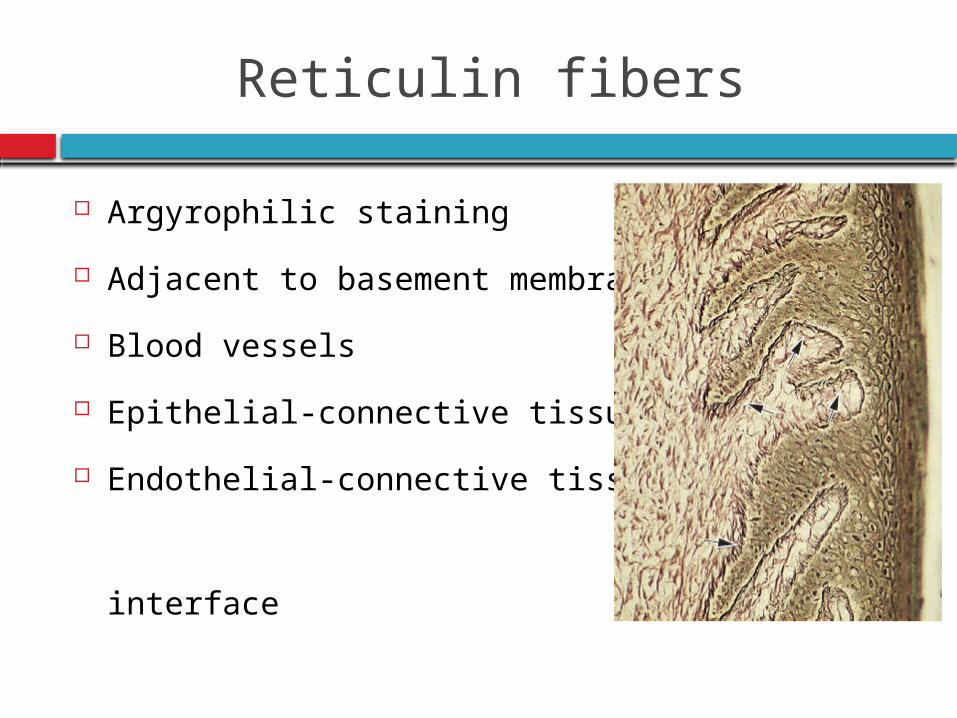
Reticulin fibers
Argyrophilic staining
Adjacent to basement membrane
Blood vessels
Epithelial-connective tissue
Endothelial-connective tissue
interface
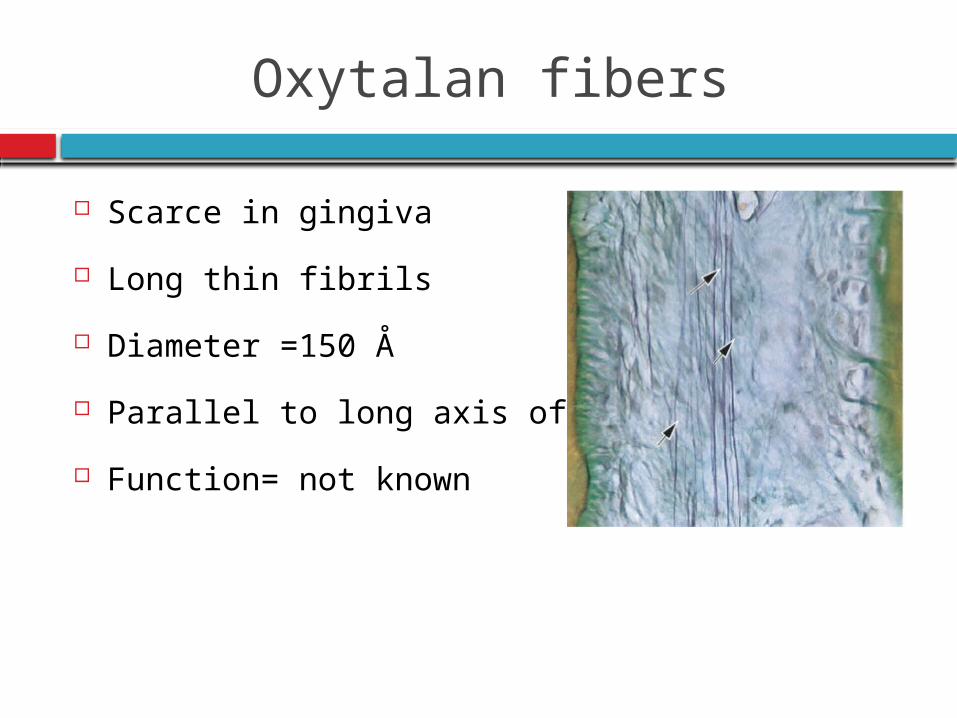
Oxytalan fibers
Scarce in gingiva
Long thin fibrils
Diameter =150 Å
Parallel to long axis of tooth
Function= not known
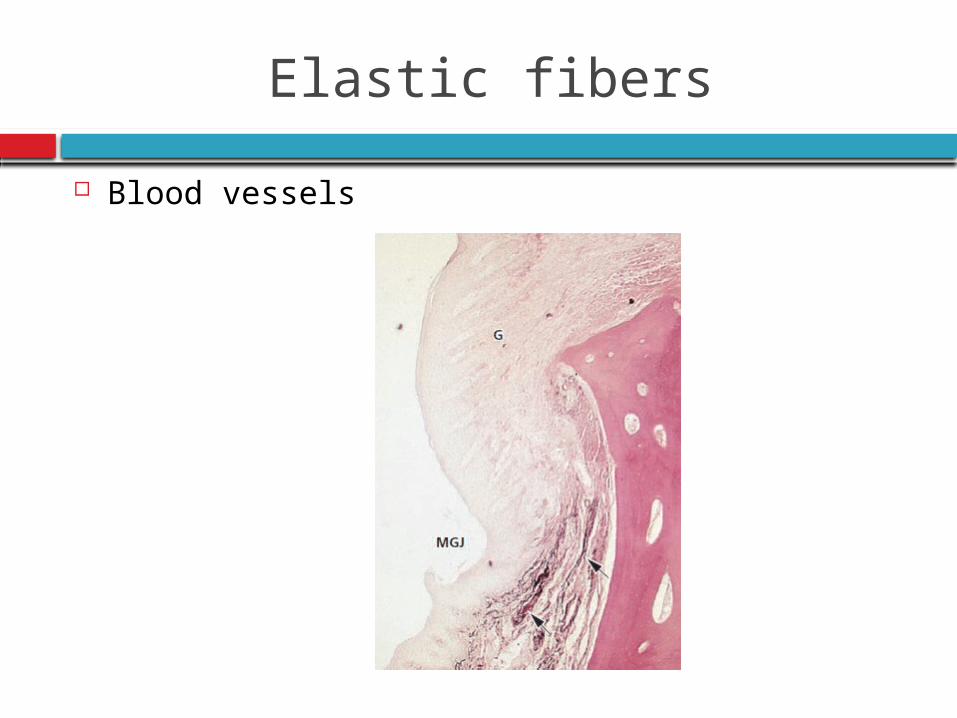
Elastic fibers
Blood vessels
Functions:
To brace marginal gingiva firmly against the tooth
To provide the rigidity necessary to withstand the
forces of mastication without being deflected away
from tooth surface
To unite the free marginal gingiva with the
cementum of the root & the adjacent attached
gingiva
Principal groups
Arnim S, Hargerman D. 1953
Secondary groups
Page R 1974
Principal group
Dentogingival Alveologingival DentoperiostealCircular Transeptal
Secondary
group
Periostogingival Interpapillary TransgingivalIntercircularIntergingivalSemicircular
Principal group
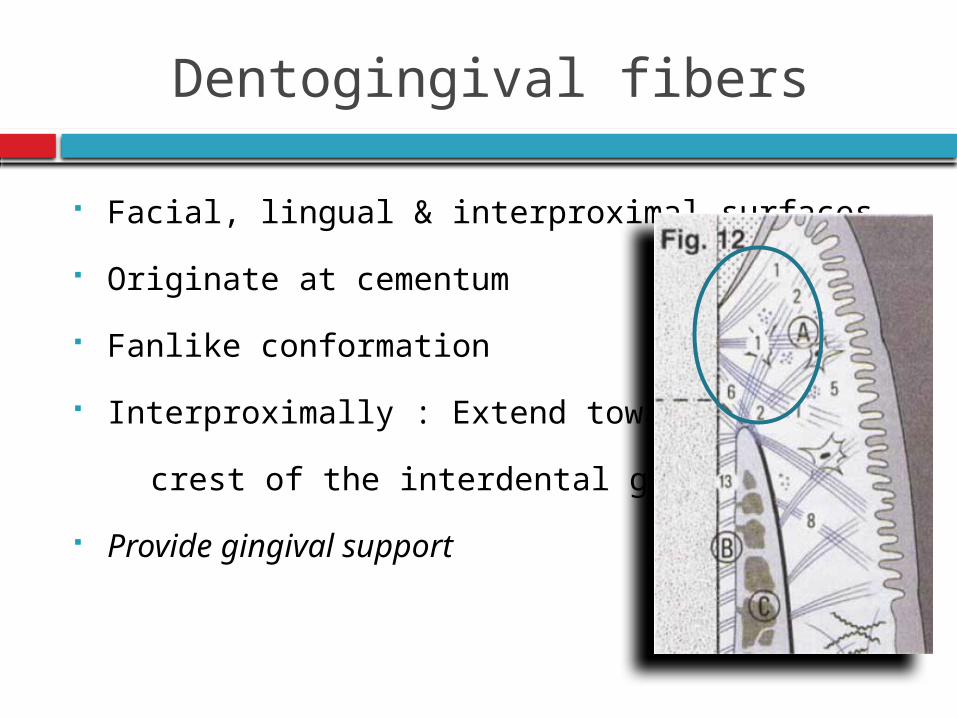
Dentogingival fibers
Facial, lingual & interproximal surfaces
Originate at cementum
Fanlike conformation
Interproximally : Extend towards
crest of the interdental gingiva
Provide gingival support
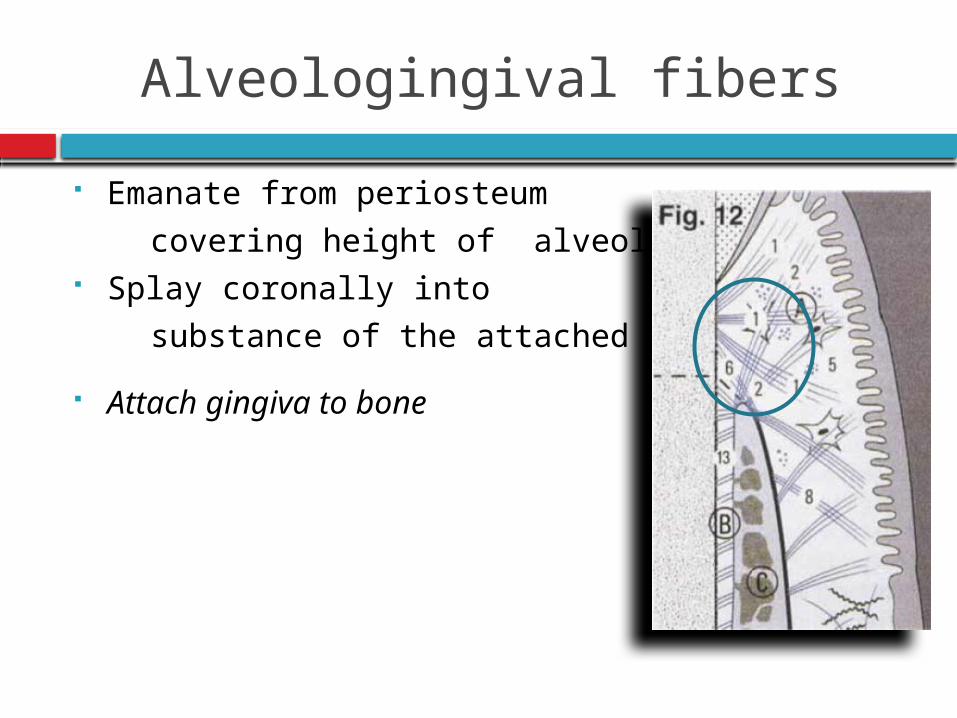
Alveologingival fibers
Emanate from periosteum
covering height of alveolar crest Splay coronally into
substance of the attached gingiva
Attach gingiva to bone
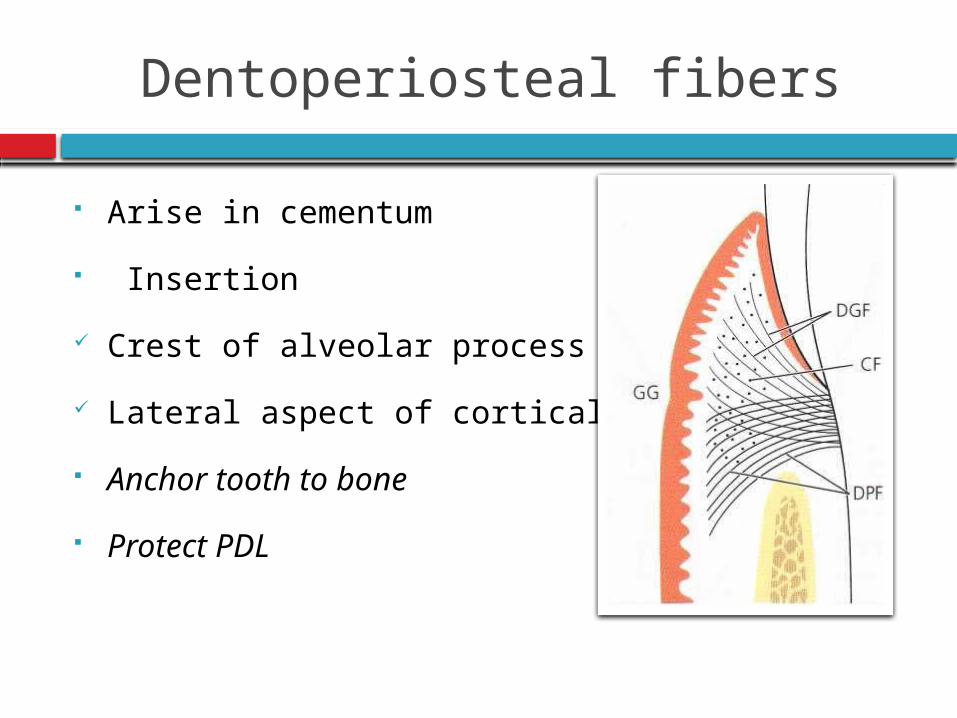
Dentoperiosteal fibers
Arise in cementum
Insertion
Crest of alveolar process
Lateral aspect of cortical plate
Anchor tooth to bone
Protect PDL
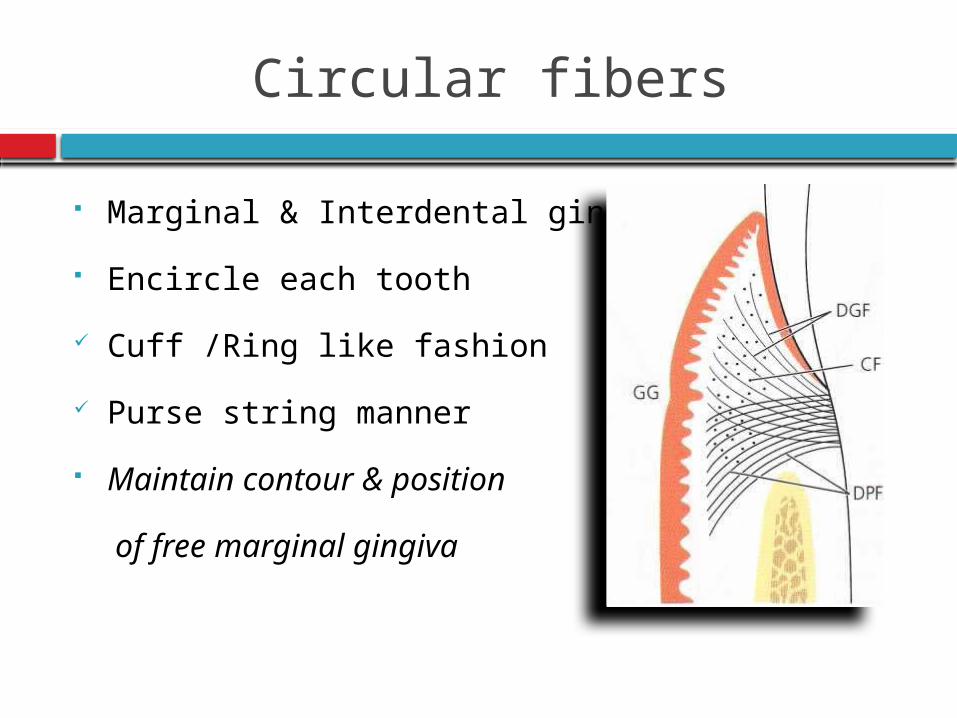
Circular fibers
Marginal & Interdental gingivae
Encircle each tooth
Cuff /Ring like fashion
Purse string manner
Maintain contour & position
of free marginal gingiva
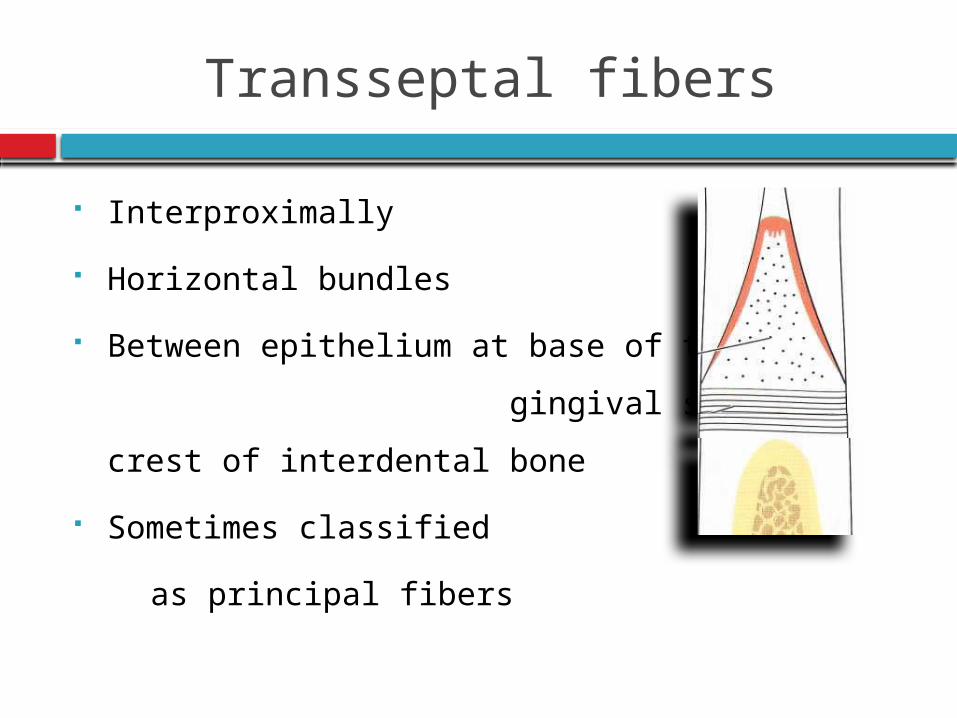
Transseptal fibers
Interproximally
Horizontal bundles
Between epithelium at base of the
gingival sulcus & crest of interdental bone
Sometimes classified
as principal fibers
Support for interdental gingiva
Secure positions of adjacent teeth
Protect interproximal bone
Maintain integrity of dentition within dental arch
Secondary group
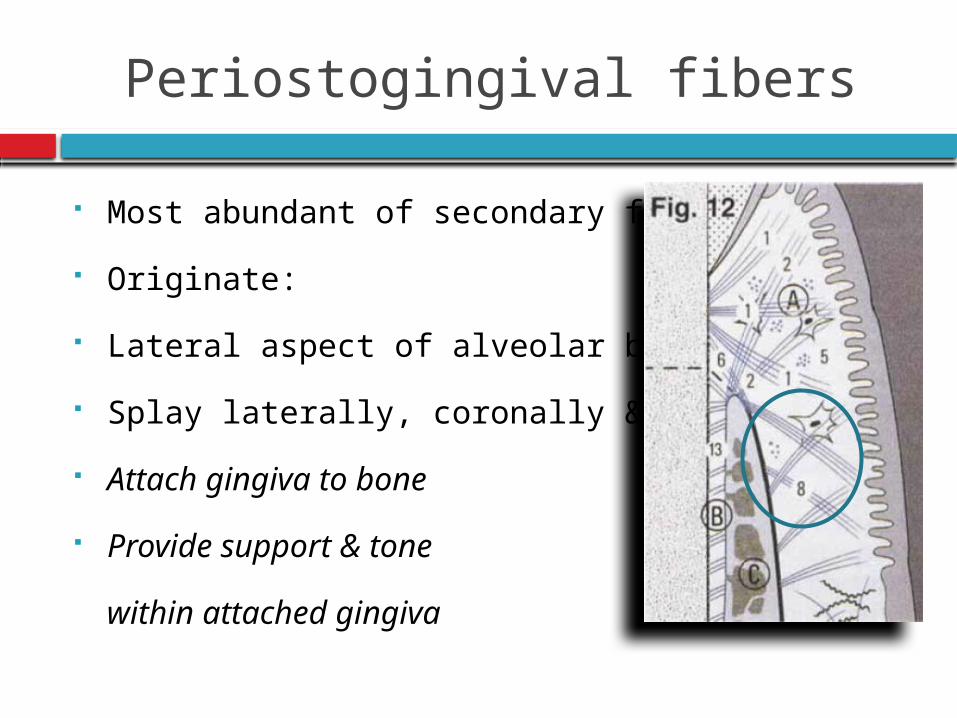
Periostogingival fibers
Most abundant of secondary fibres
Originate:
Lateral aspect of alveolar bone
Splay laterally, coronally & apically
Attach gingiva to bone
Provide support & tone
within attached gingiva
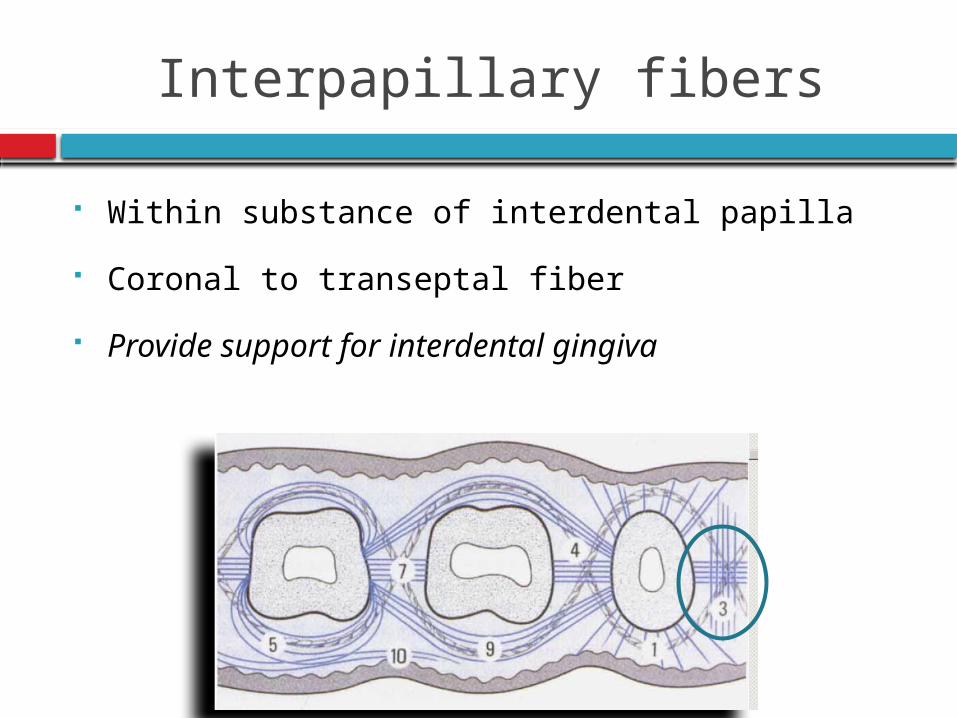
Interpapillary fibers
Within substance of interdental papilla
Coronal to transeptal fiber
Provide support for interdental gingiva
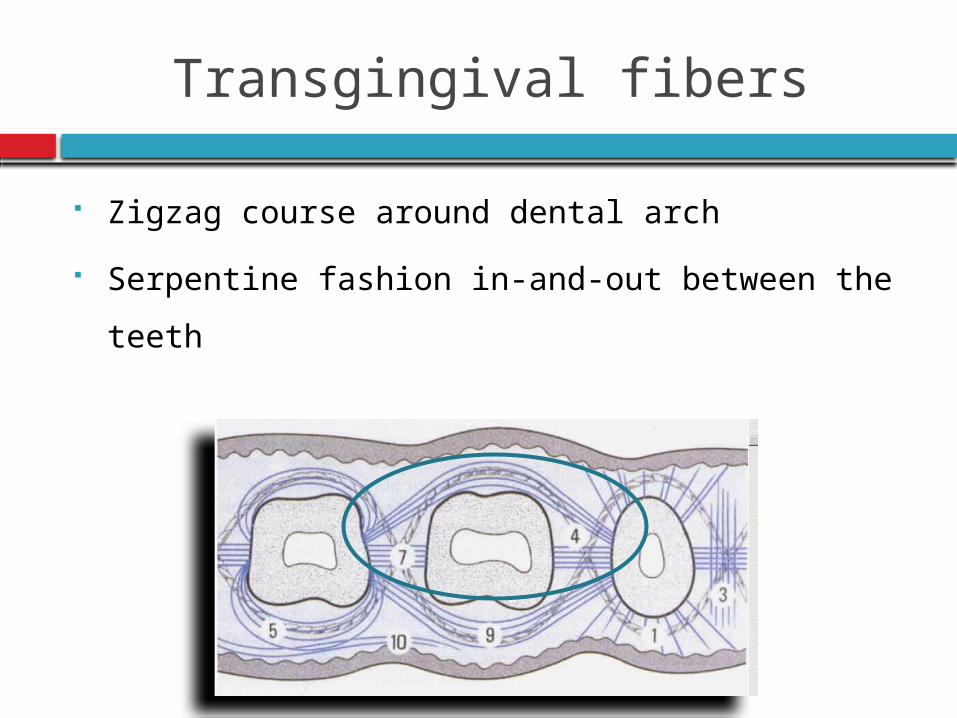
Transgingival fibers
Zigzag course around dental arch
Serpentine fashion in-and-out between the teeth
Coronal to CEJ
Maintain tissue consistency, enhance arch
alignment & provide additional support for
marginal gingiva
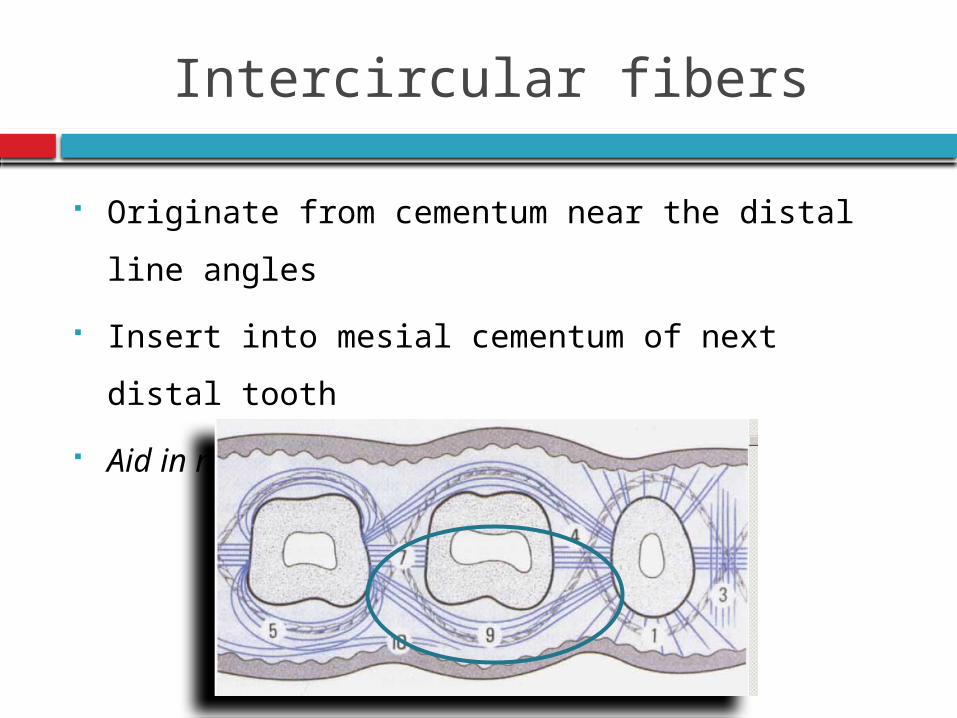
Intercircular fibers
Originate from cementum near the distal line
angles
Insert into mesial cementum of next distal tooth
Aid in maintaining arch integrity
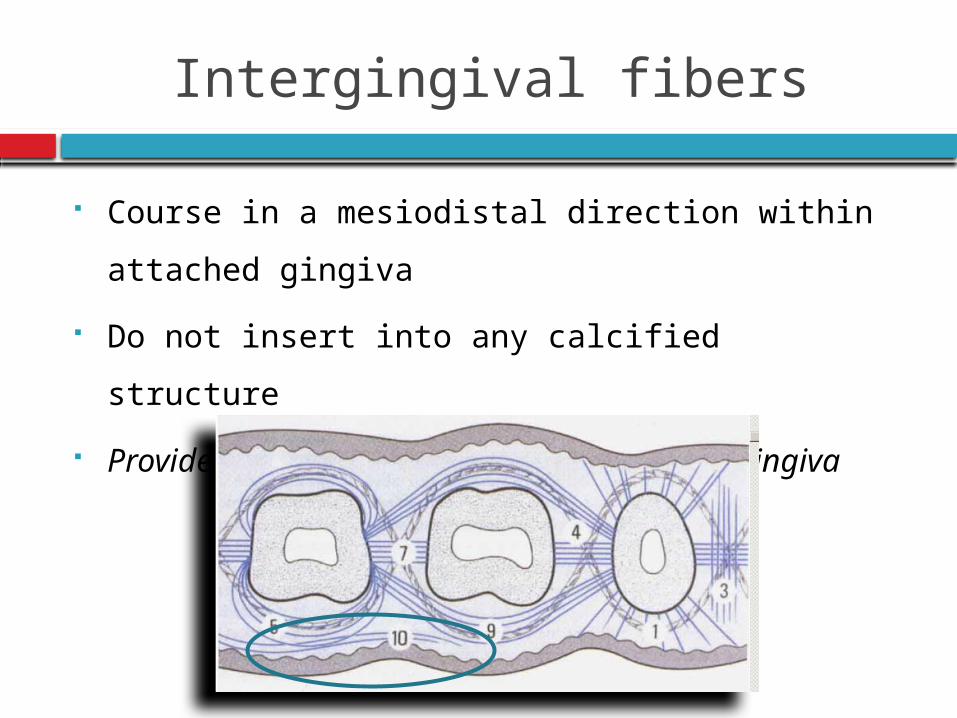
Intergingival fibers
Course in a mesiodistal direction within attached
gingiva
Do not insert into any calcified structure
Provide form, support &contour of attached
gingiva
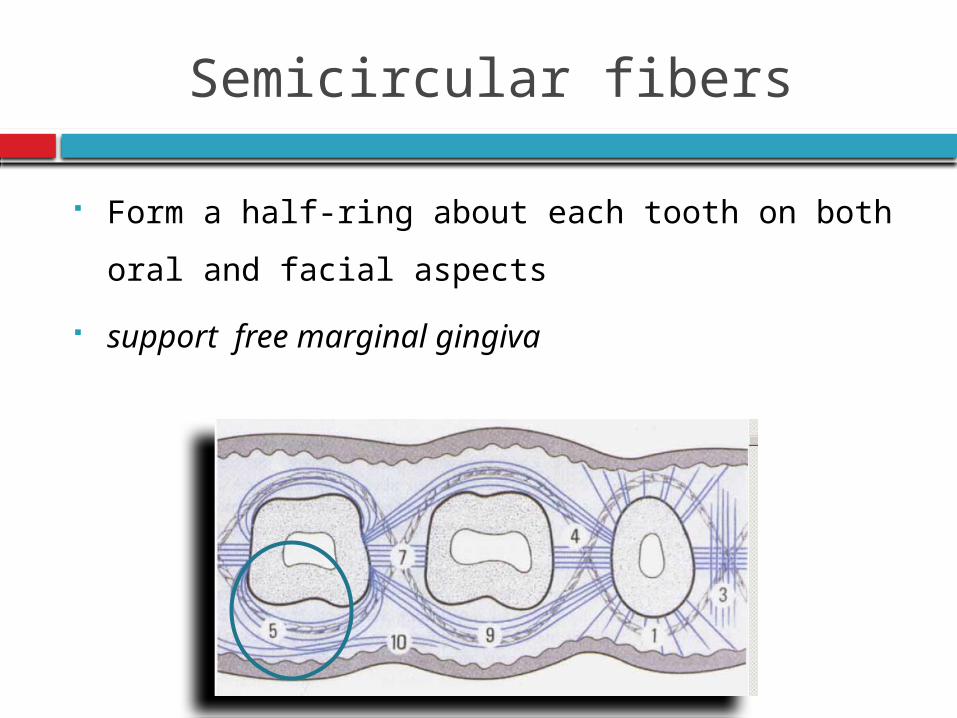
Semicircular fibers
Form a half-ring about each tooth on both oral
and facial aspects
support free marginal gingiva
Ground substance
Fills the space between fibers & cells
Amorphous
Water
Proteoglycan
Glycoprotein
Glycosaminoglycans
Dermatan sulfate (60%)
Chondroitin sulfate (30%)
Hyaluronan and Heparan sulfate (10%)
Decorin, Biglycan, Versican, Syndecan, CD-44 &
Perlecan
Glycoprotein
Fibronectin
Distributed throughout gingival connective
tissues
Localized over collagen fibers
Binds fibroblasts to fibers
Mediate cell adhesion & migration
Osteonectin, Vitronectin, Elastin & Tenascin
Present diffusely
Near the subepithelial basement membrane in
the upper connective tissue & capillary blood
vessels
Laminin
Basal laminae
Attach it to epithelial cells
Repair of gingival connective tissue
High turnover rate
Remarkably good healing and regenerative
capacity
Generally shows little evidence of scarring after
surgical procedures
Rapid reconstruction of the fibrous architecture of
tissues
Melcher 1976
Within hours
Wound site stabilized by fibrin clot formation
Heavy infiltrate of neutrophils
Within 3 days
Granulation tissue evident
Heavily infiltrate of inflammatory cells
Fibrin clot is slowly degraded
Day 7
Rich in newly formed granulation tissue
Collagen fibers align parallel along root surface
Day 14
Collagen fibers show signs of attachment to root
surface
3 weeks
Fully functional connective tissue attachment
Reformation of Sharpey’s fibers
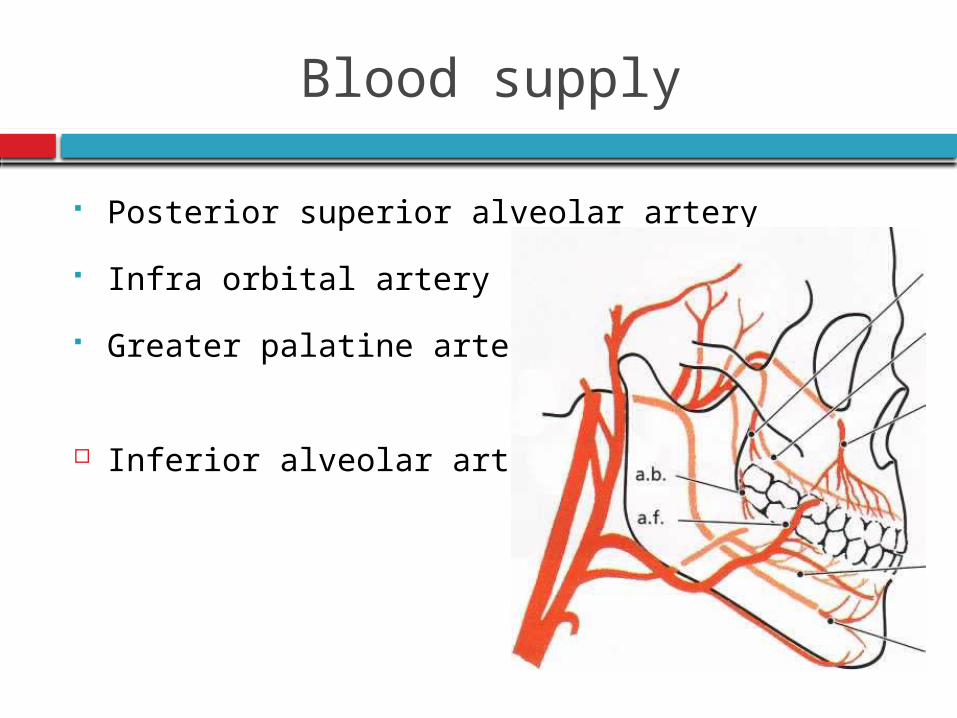
Blood supply
Posterior superior alveolar artery
Infra orbital artery
Greater palatine artery
Inferior alveolar artery
Supraperiosteal arterioles
Arterioles from crest of interdental septa
Vessels of PDL
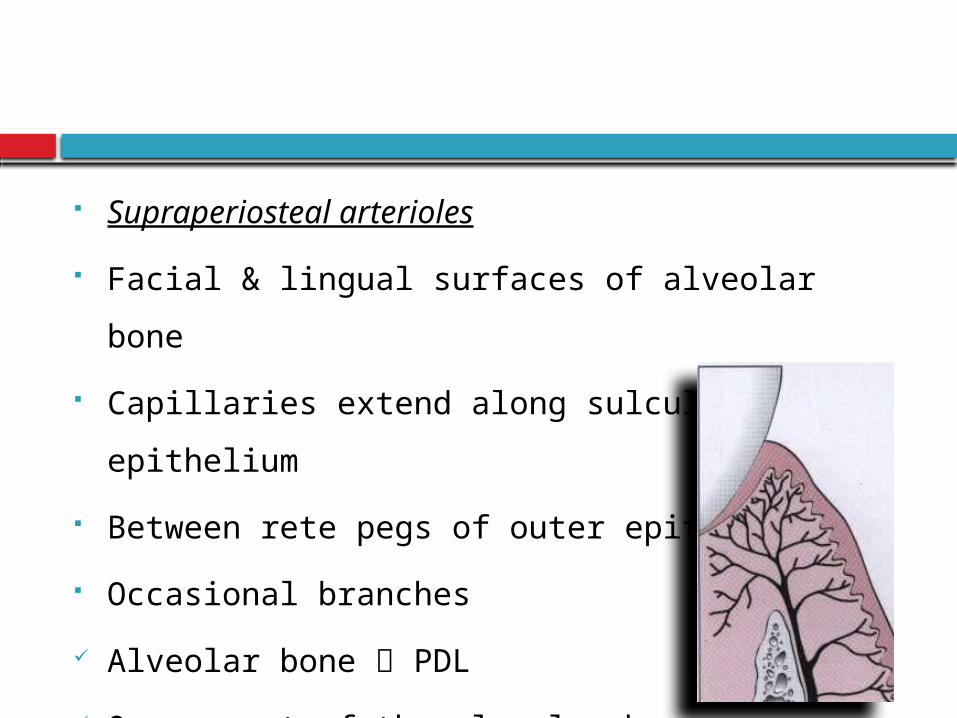
Supraperiosteal arterioles
Facial & lingual surfaces of alveolar bone
Capillaries extend along sulcular epithelium
Between rete pegs of outer epithelium
Occasional branches
Alveolar bone PDL
Over crest of the alveolar bone
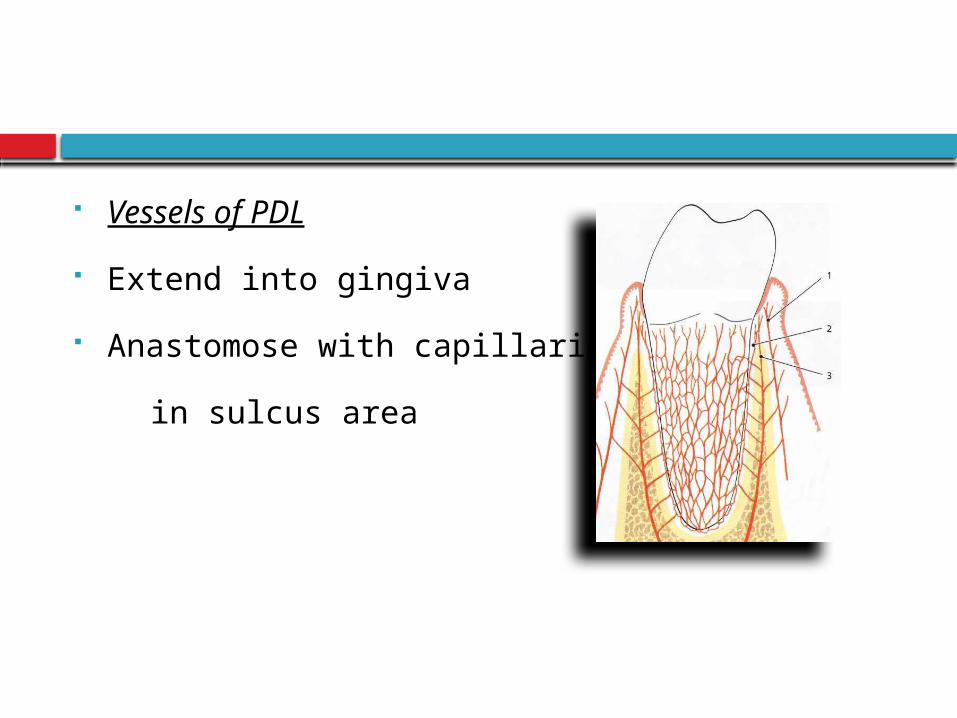
Vessels of PDL
Extend into gingiva
Anastomose with capillaries
in sulcus area
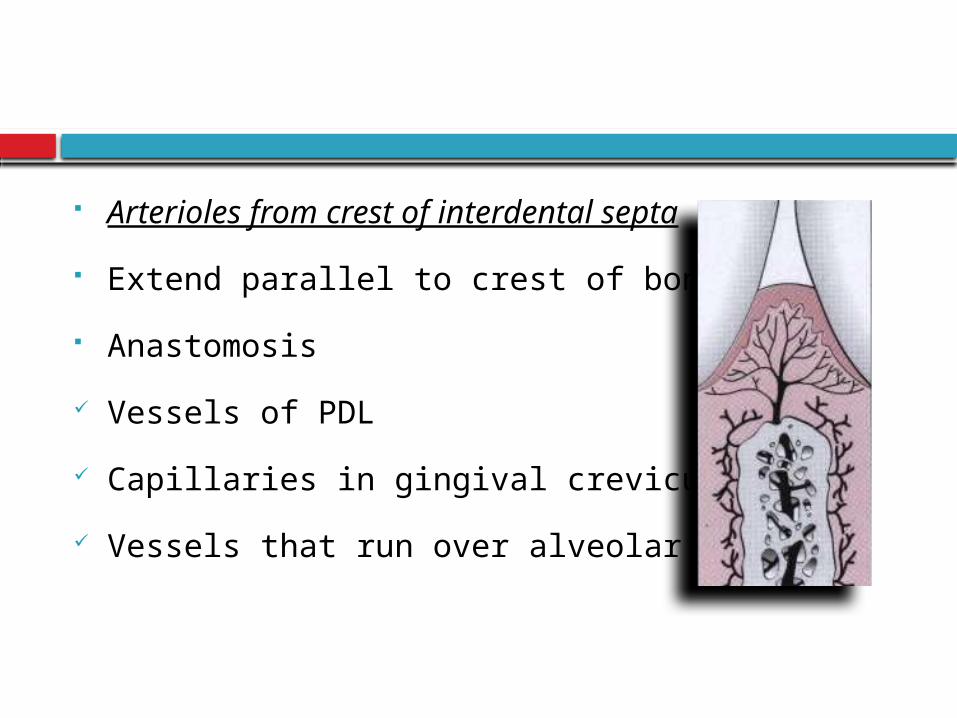
Arterioles from crest of interdental septa
Extend parallel to crest of bone
Anastomosis
Vessels of PDL
Capillaries in gingival crevicular areas
Vessels that run over alveolar crest
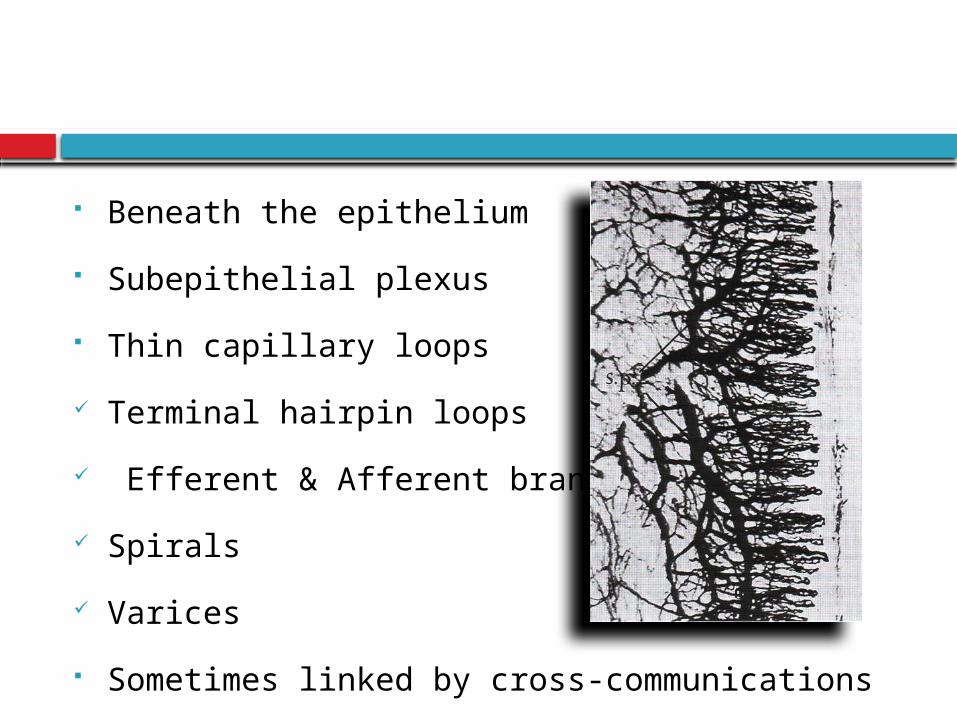
Beneath the epithelium
Subepithelial plexus
Thin capillary loops
Terminal hairpin loops
Efferent & Afferent branches
Spirals
Varices
Sometimes linked by cross-communications
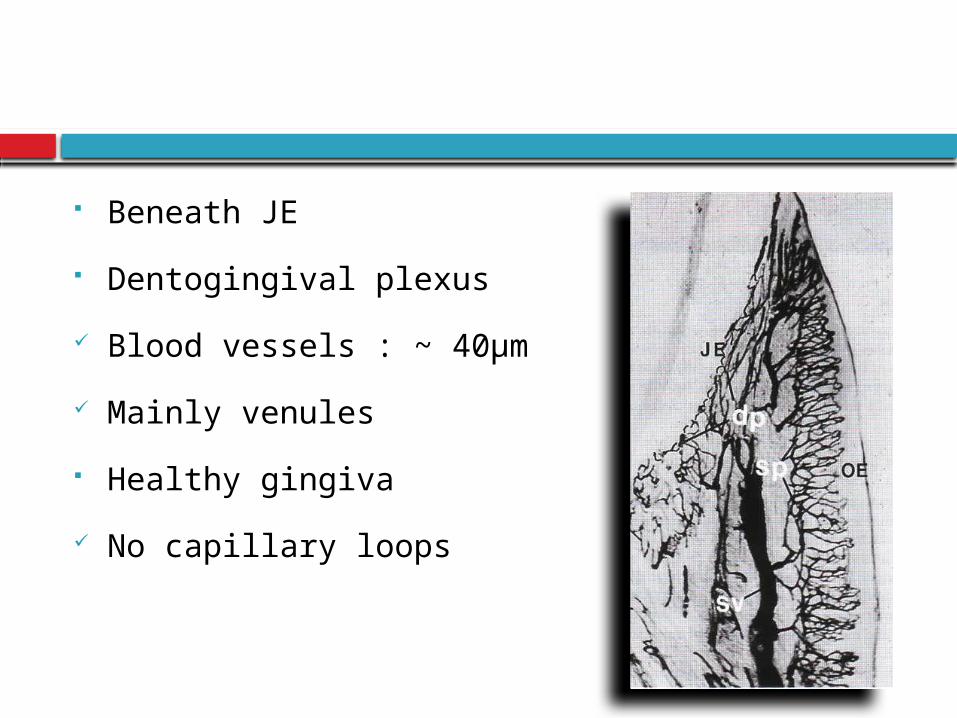
Beneath JE
Dentogingival plexus
Blood vessels : ~ 40µm
Mainly venules
Healthy gingiva
No capillary loops
Sulcular epithelium : Flat anastomosing plexus
Col area : Mixed pattern of anastomosing
capillaries & loops
Absence of inflammation
Regular, repetitive & layered pattern
Inflamed gingival vasculature
Irregular vascular plexus pattern
Lymphatics
Remove excess fluids, cellular and protein
debris, microorganisms & other elements
Control diffusion
Resolution of inflammatory processes
Lymphatics of connective tissue papillae
Collecting network external to periosteum
Regional lymph nodes
Lymphatics beneath JE
PDL
Accompany blood vessels
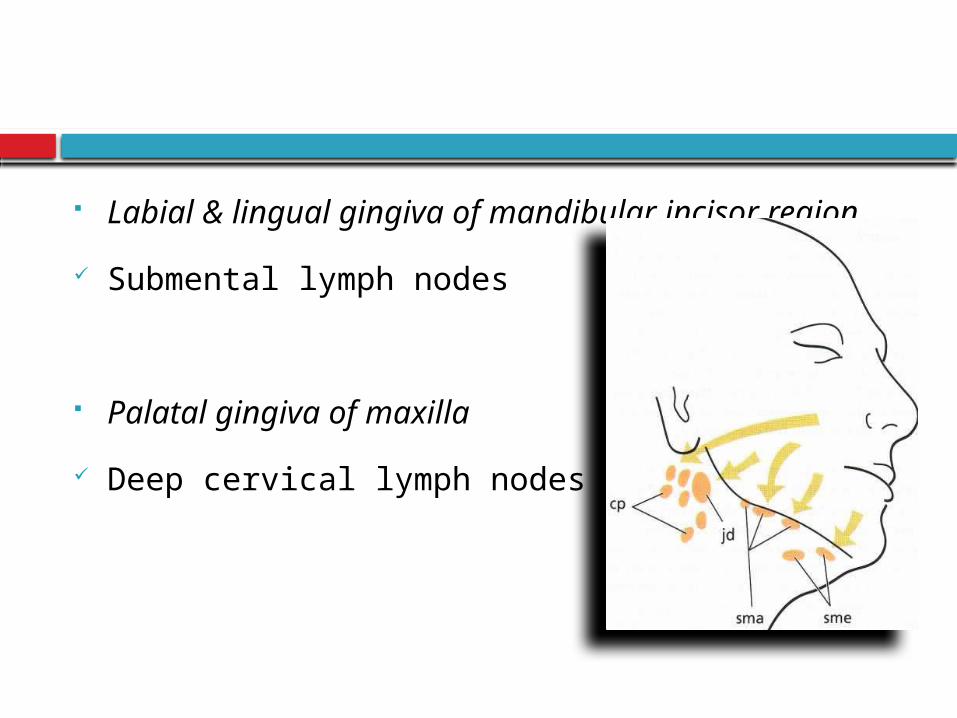
Labial & lingual gingiva of mandibular incisor
region
Submental lymph nodes
Palatal gingiva of maxilla
Deep cervical lymph nodes
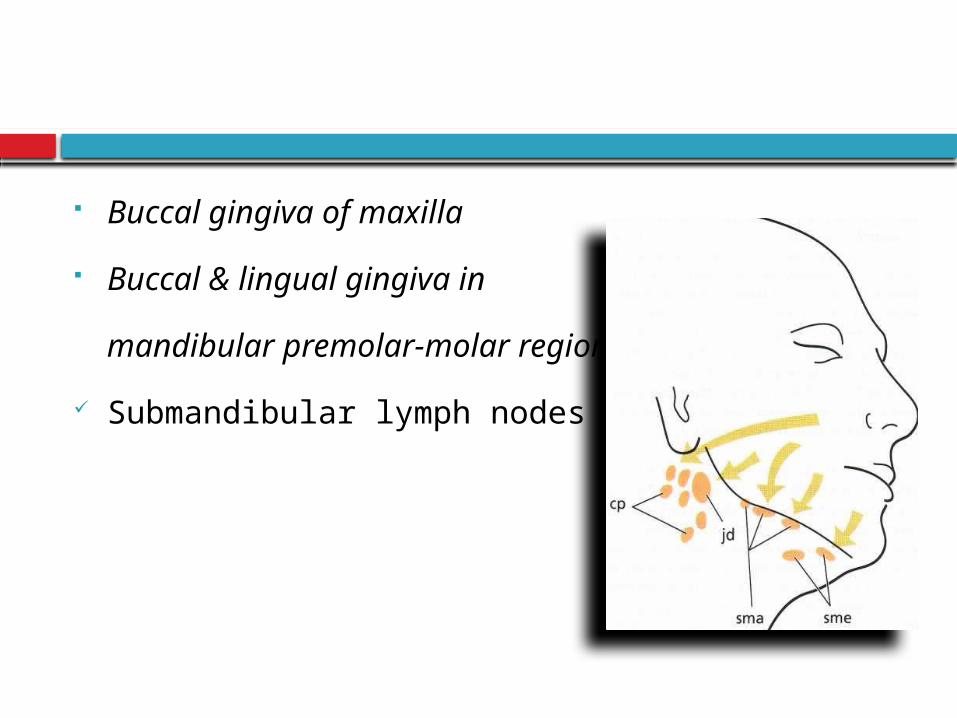
Buccal gingiva of maxilla
Buccal & lingual gingiva in
mandibular premolar-molar region
Submandibular lymph nodes
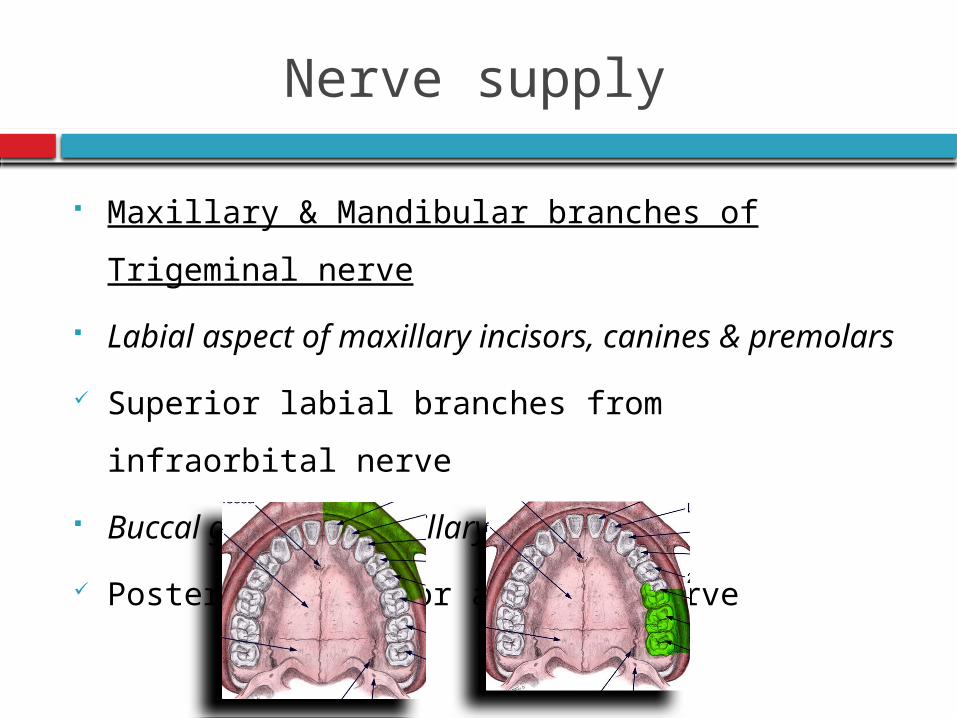
Nerve supply
Maxillary & Mandibular branches of Trigeminal
nerve
Labial aspect of maxillary incisors, canines &
premolars
Superior labial branches from infraorbital nerve
Buccal gingiva in maxillary molar region
Posterior superior alveolar nerve
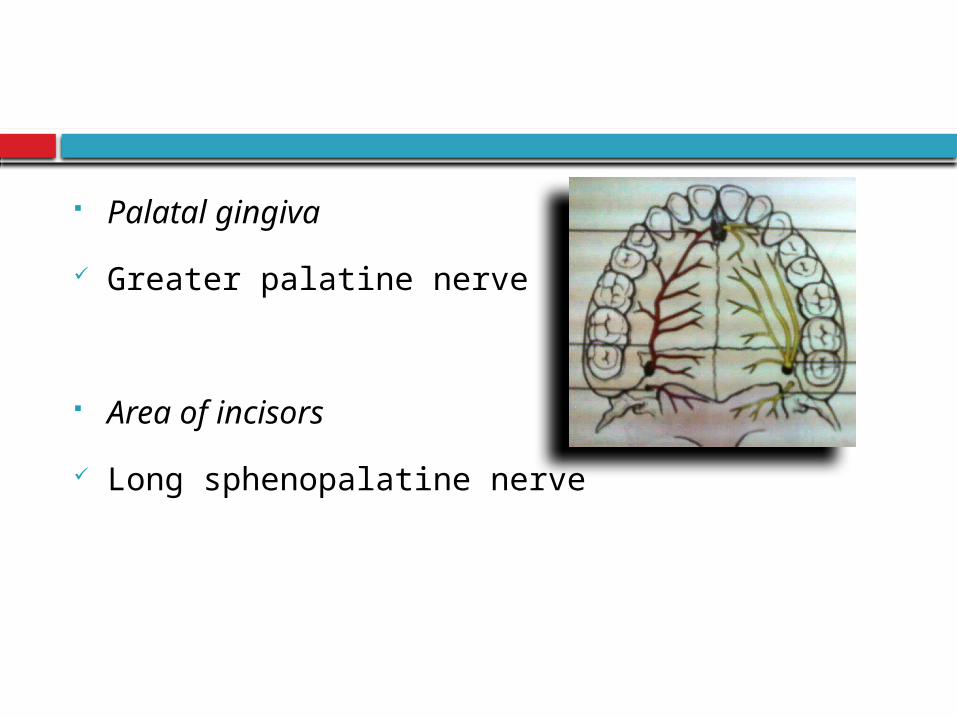
Palatal gingiva
Greater palatine nerve
Area of incisors
Long sphenopalatine nerve
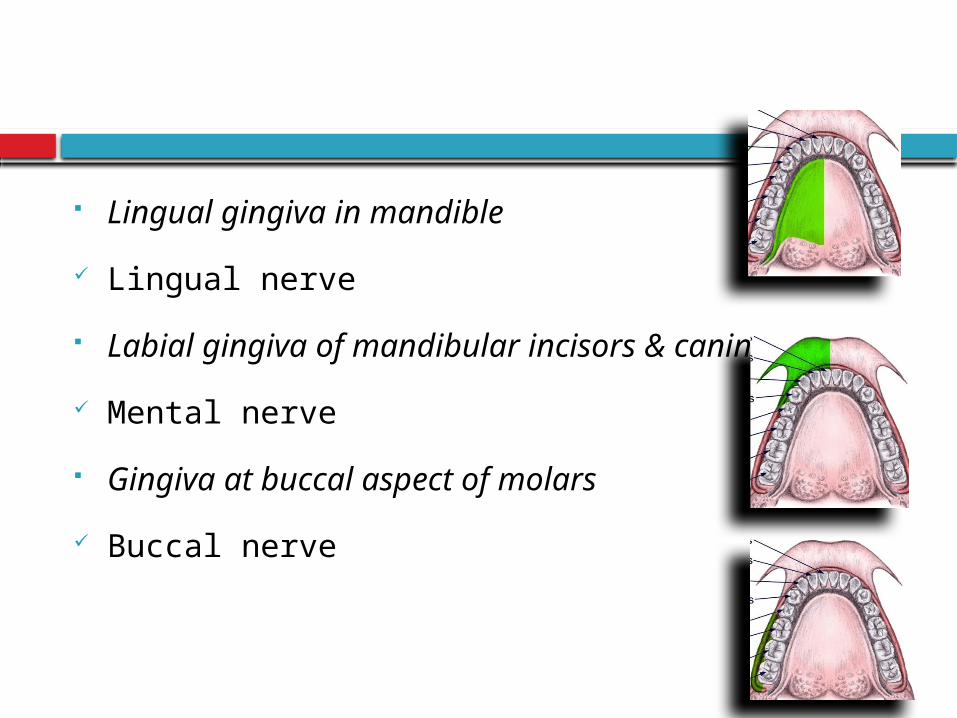
Lingual gingiva in mandible
Lingual nerve
Labial gingiva of mandibular incisors & canines
Mental nerve
Gingiva at buccal aspect of molars
Buccal nerve
Gingival connective tissues
Most nerve fibres : Myelinated
Blood vessels
Gingival innervation : Derived from fibers arising
from nerves in the PDL & from the labial, buccal,
and palatal nerves
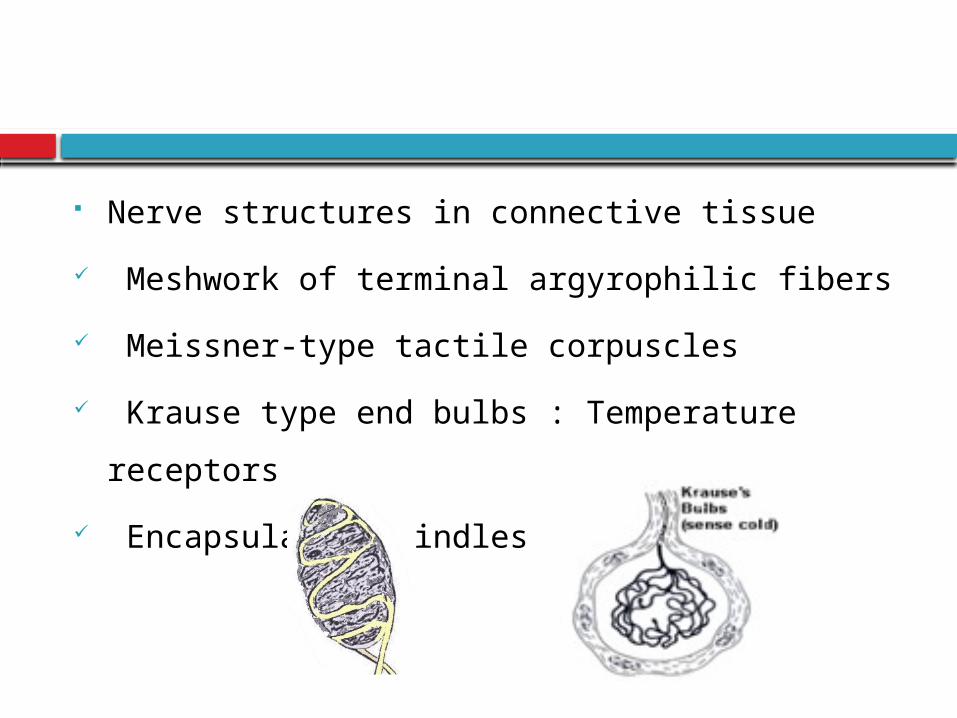
Nerve structures in connective tissue
Meshwork of terminal argyrophilic fibers
Meissner-type tactile corpuscles
Krause type end bulbs : Temperature receptors
Encapsulated spindles
Correlation of clinical & microscopic features
Color
Size
Contour
Shape
Consistency
Surface texture
Position
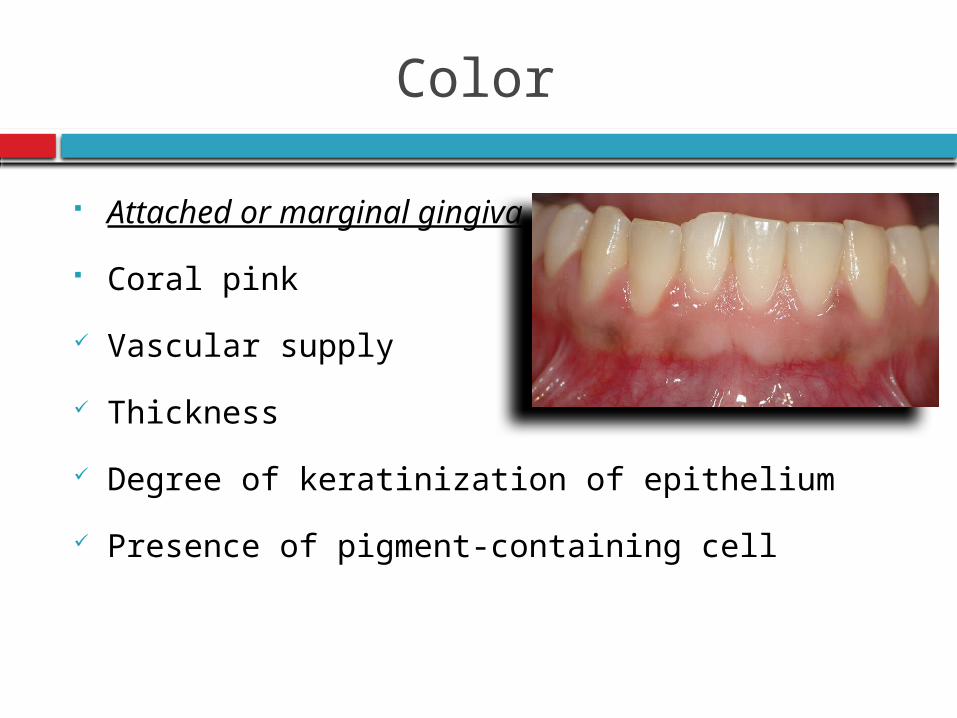
Color
Attached or marginal gingiva
Coral pink
Vascular supply
Thickness
Degree of keratinization of epithelium
Presence of pigment-containing cell
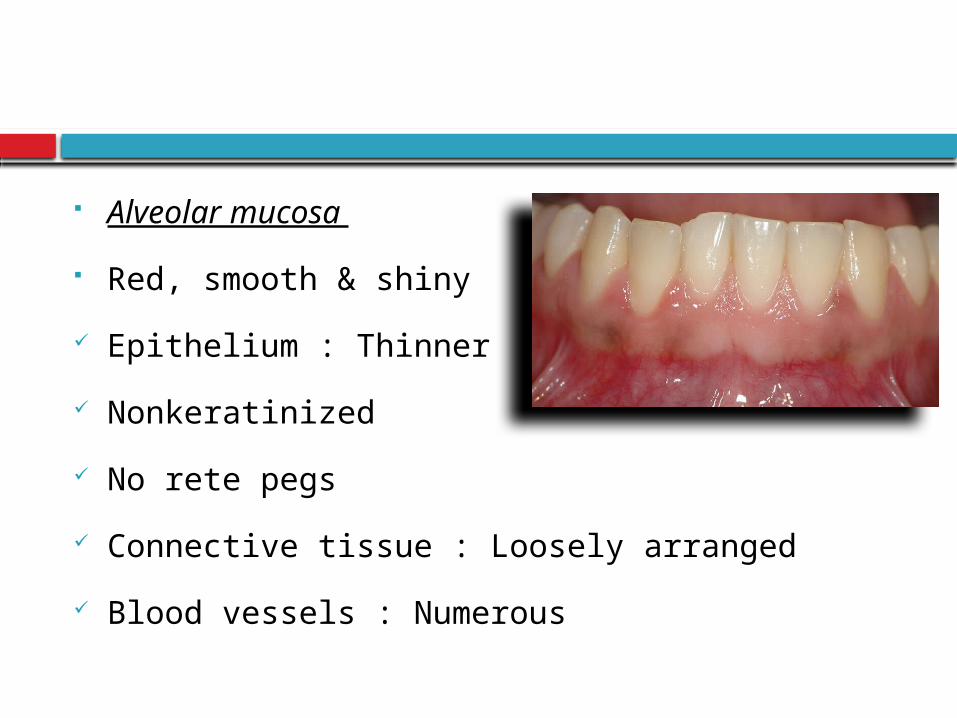
Alveolar mucosa
Red, smooth & shiny
Epithelium : Thinner
Nonkeratinized
No rete pegs
Connective tissue : Loosely arranged
Blood vessels : Numerous
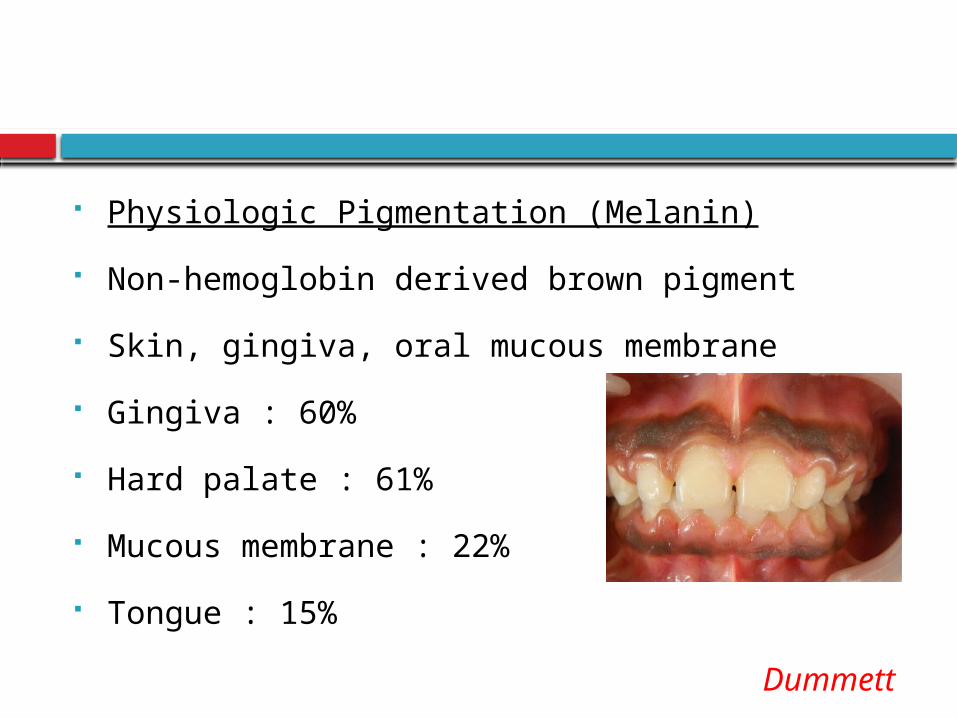
Physiologic Pigmentation (Melanin)
Non-hemoglobin derived brown pigment
Skin, gingiva, oral mucous membrane
Gingiva : 60%
Hard palate : 61%
Mucous membrane : 22%
Tongue : 15%
Dummett 1946
Diffuse, deep-purplish discoloration
Irregularly shaped brown & light brown patches
As early as 3 hours after birth
Size
Cellular &
Intercellular
elements
Vascular
supply
size
Contour
Shape of the teeth
Alignment in the arch
Location & Size of proximal contact
Facial & lingual gingival embrasures
Marginal gingiva : Scalloped outline
Flat surfaces : Straight line
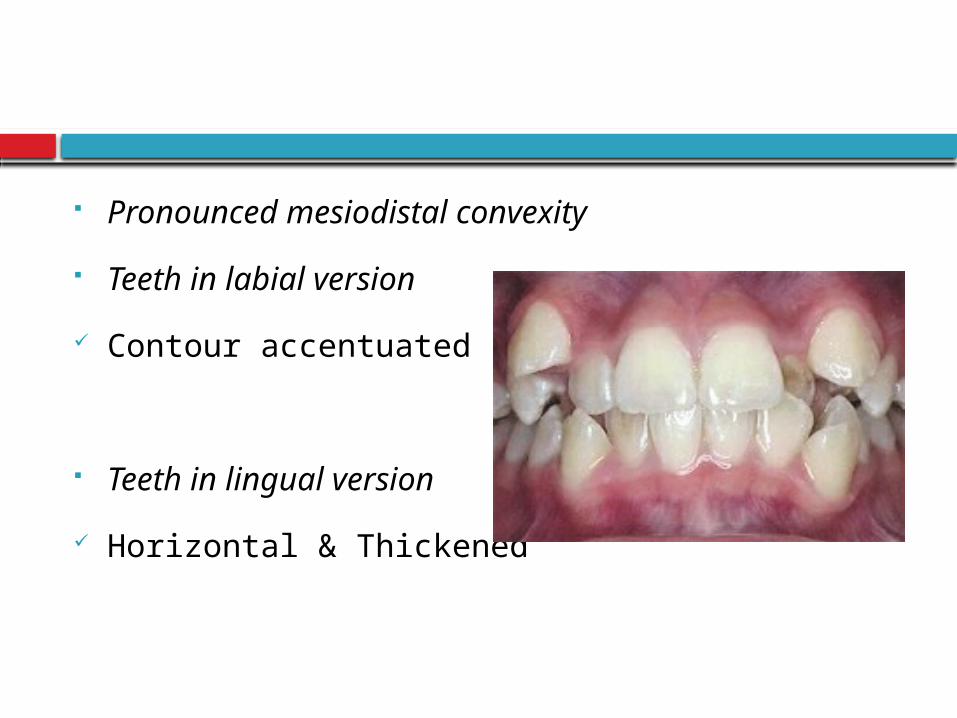
Pronounced mesiodistal convexity
Teeth in labial version
Contour accentuated
Teeth in lingual version
Horizontal & Thickened
Shape
Interdental gingiva
Contour of proximal tooth surfaces
Location & shape of gingival embrasures
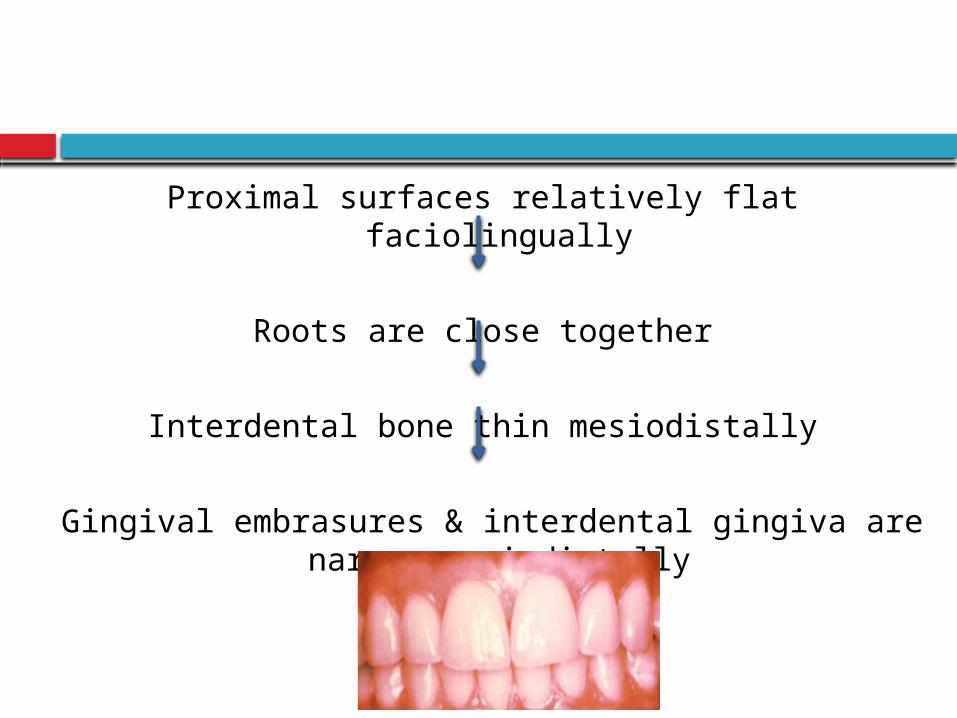
Proximal surfaces relatively flat faciolingually
Roots are close together
Interdental bone thin mesiodistally
Gingival embrasures & interdental gingiva are narrow mesiodistally
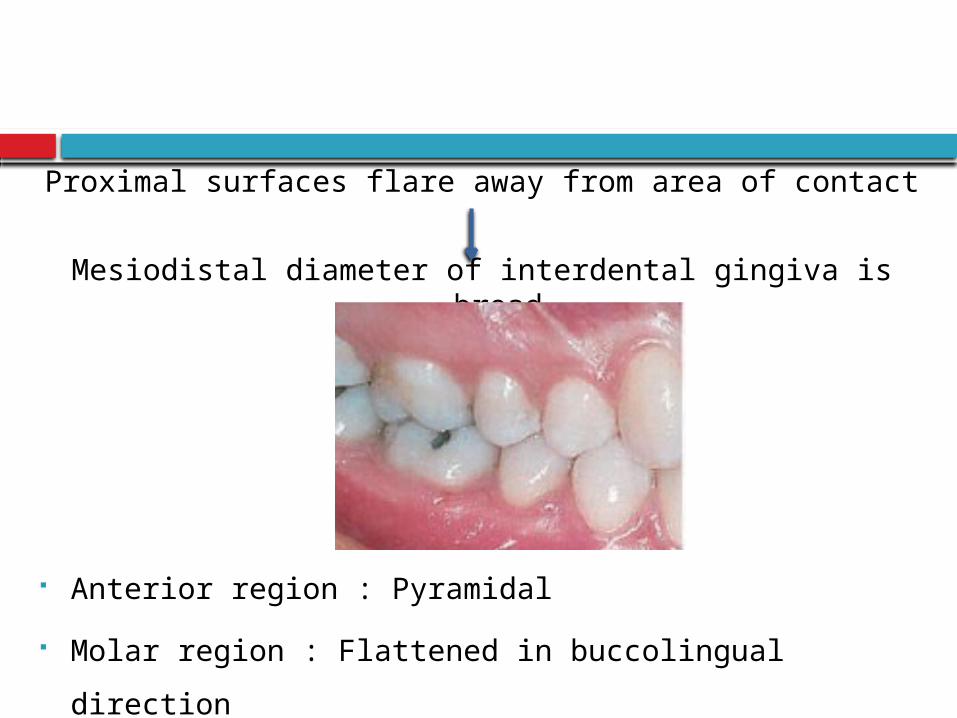
Proximal surfaces flare away from area of contact
Mesiodistal diameter of interdental gingiva is broad
Anterior region : Pyramidal
Molar region : Flattened in buccolingual direction
Consistency
Firm & Resilient
Tightly bound to underlying bone
Exception : Movable free margin
Collagenous lamina propria
Contiguity with mucoperiosteum
Gingival fibers
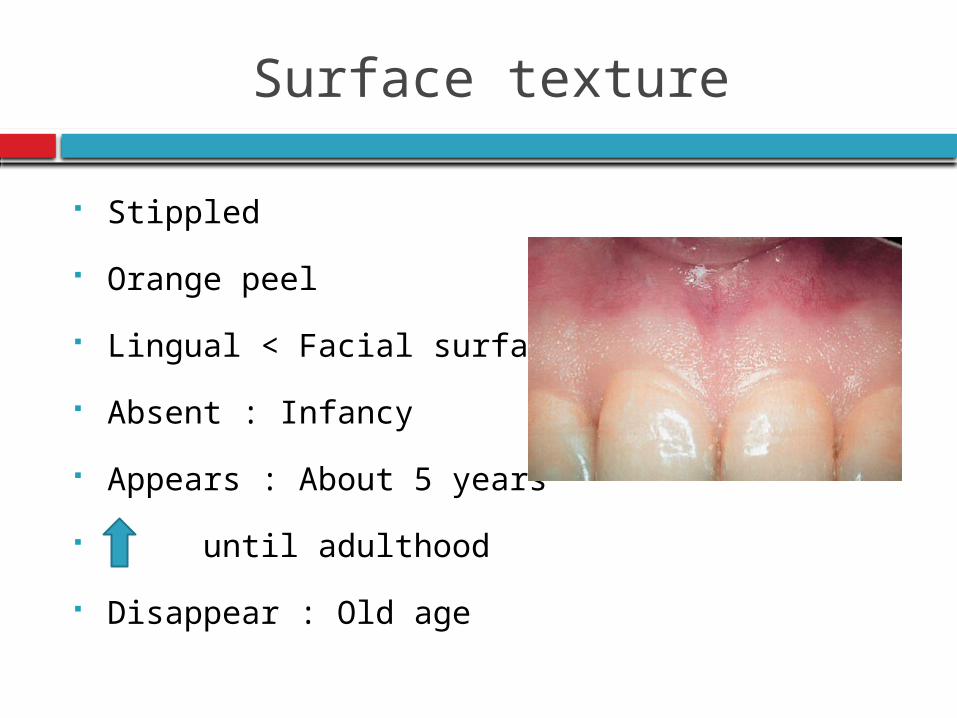
Surface texture
Stippled
Orange peel
Lingual < Facial surfaces
Absent : Infancy
Appears : About 5 years
until adulthood
Disappear : Old age
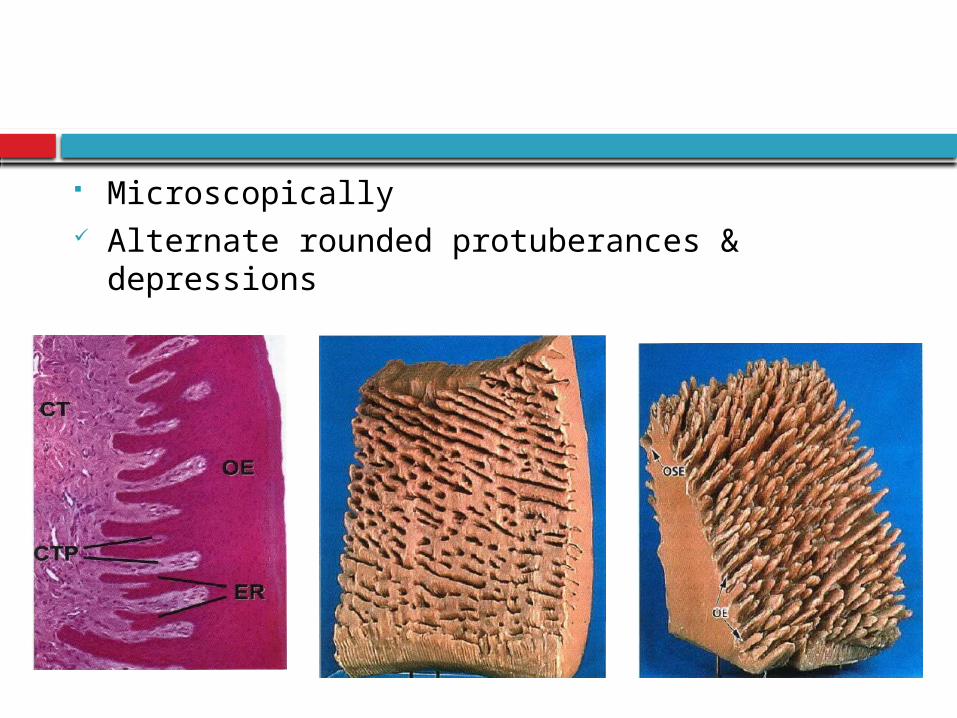
Microscopically Alternate rounded protuberances & depressions
Degree of keratinization
Low magnification : Rippled surface interrupted
by irregular depressions (50 µm)
Higher magnification : Cell micropits
Adaptive specialization/ Reinforcement for
function
Reduction or loss of stippling
Gingival disease
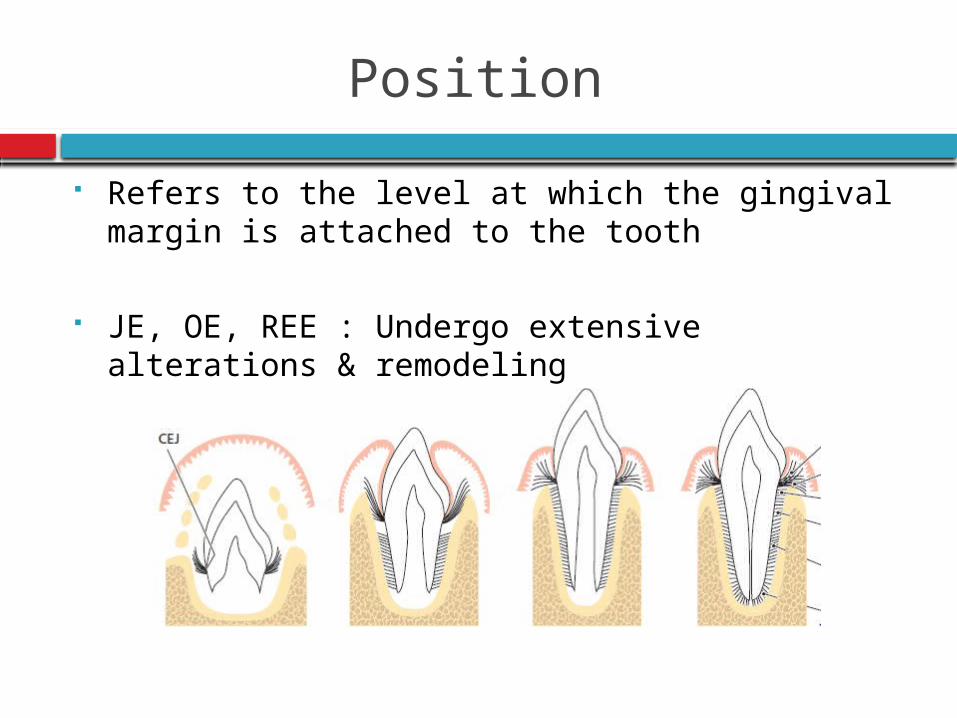
Position
Refers to the level at which the gingival margin is attached to the tooth
JE, OE, REE : Undergo extensive alterations & remodeling
Continuous Tooth Eruption
Gottlieb & Orban, 1933
Active eruption : Movement of the teeth in the
direction of the occlusal plane
Passive eruption : Exposure of the teeth by
apical migration of the gingiva
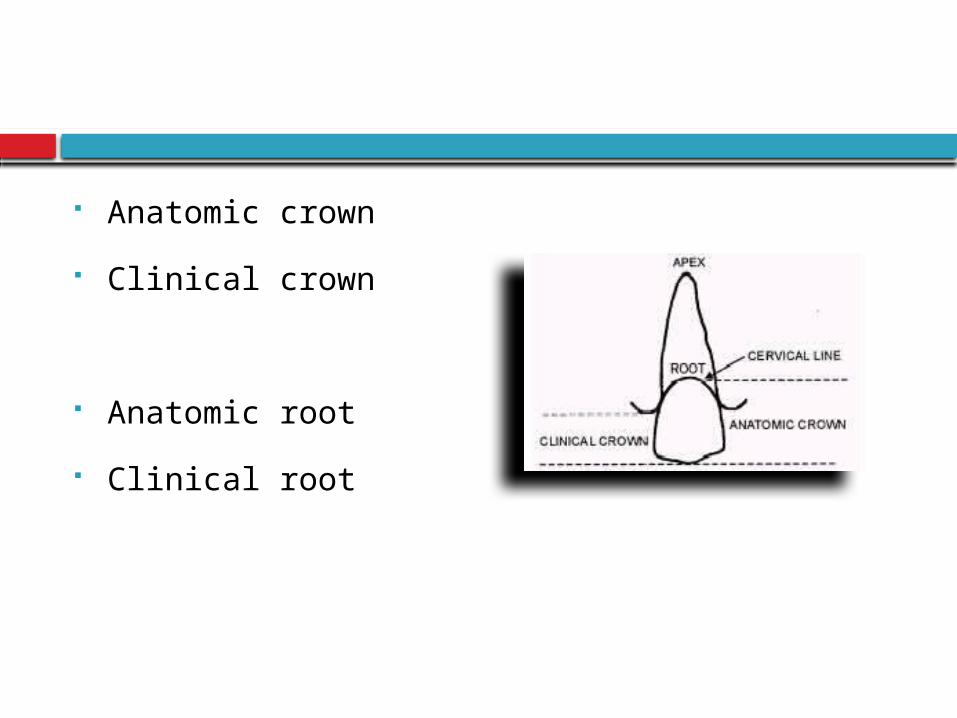
Anatomic crown
Clinical crown
Anatomic root
Clinical root
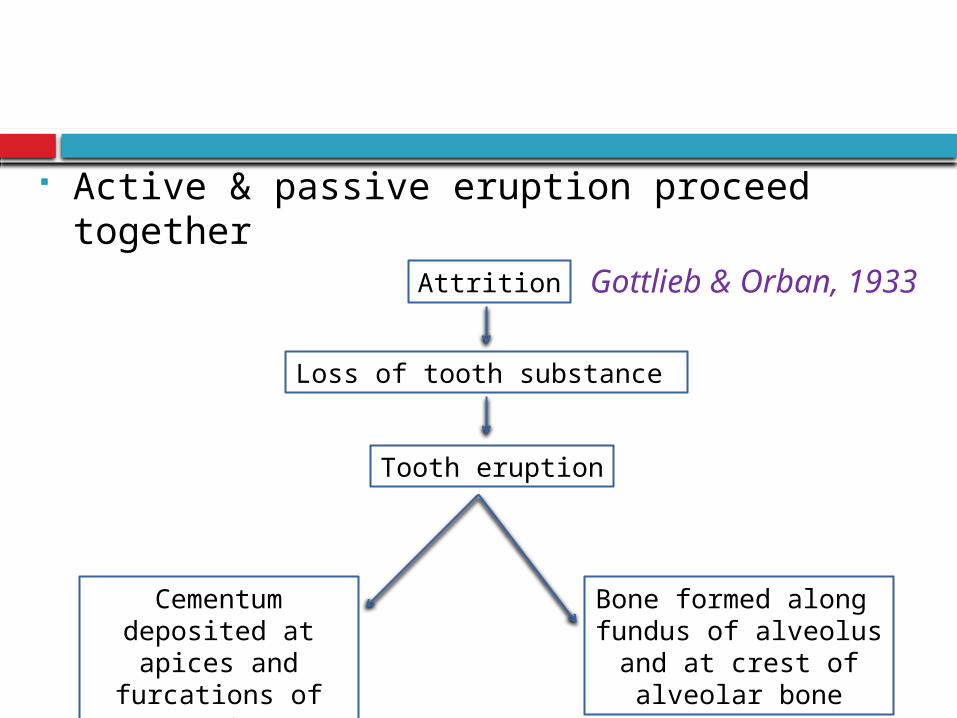
Active & passive eruption proceed together Gottlieb &
Orban, 1933 Attrition
Loss of tooth substance
Tooth eruption
Cementum deposited at apices and furcations of
roots
Bone formed along fundus of alveolus and at
crest of alveolar bone
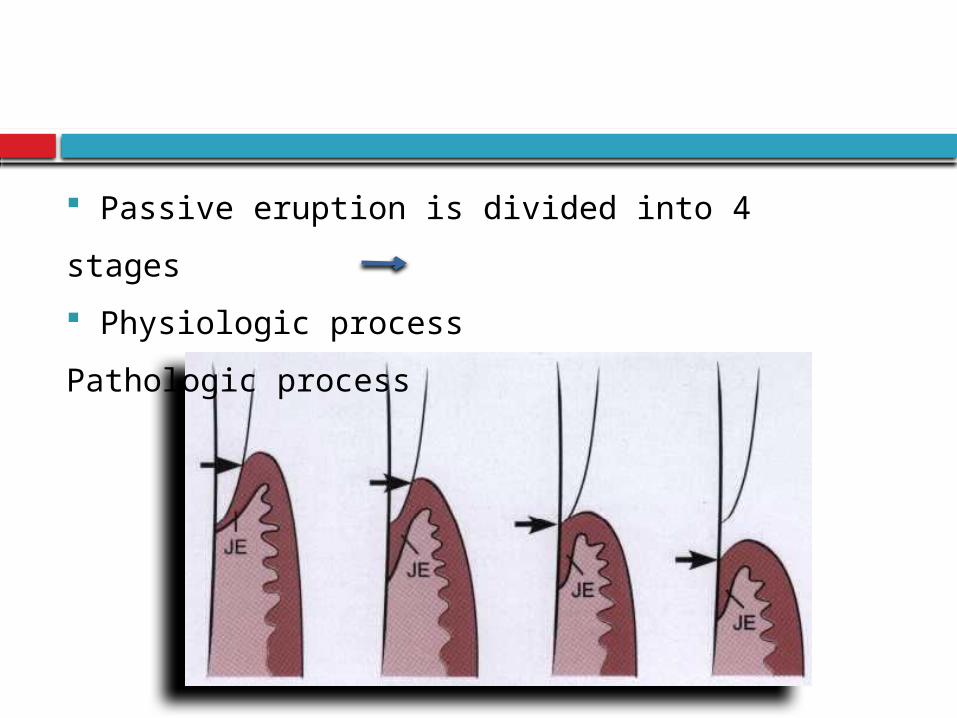
Passive eruption is divided into 4 stages
Physiologic process Pathologic
process
Age changes
Gingival Epithelium Thinning of epithelium
Shklar 1966
Decreased keratinization
Glickman 1950
Shape of the Rete pegs (Conflicting results) Flattening of rete pegs
Shklar 1966 Height of epithelial ridges increased
Wentz 1952 Formation of epithelial cross ridges
Loe & Karring 1972
↑ cell density
Meyer 1956,Ryan 1974 Morphology : Do not change
Wentz 1952 Regeneration time (Conflicting results) Mitotic activity ↑
Meyer 1956,Gargiulo 1961 Constant
Ryan 1974 Mitotic activity↓
Karring and Loe 1973
Location of JE
Health: Apical termination of JE located at CEJ
Dental plaque : Etiological factor in development
of gingivitis
Suami,1971
Absence of plaque : Periodontal breakdown does
not occur : periodontal pocket will not occur
Lindhe & Nyman 1975; Axellsson &
Lindhe 1978
Continuous presence of plaque & its quantity :
Development & course of periodontal disease
Contradicting studies
Apical migration of JE can occur in absence of plaque & inflammatory cells
Skilleni 1930, Rushton 1951, Beersten et al 1982
Continuous passive eruption theory
Gottlieb and Orban 1933
Age : Gradual physiological recession of gingiva concomitantly with apical migration of epithelium
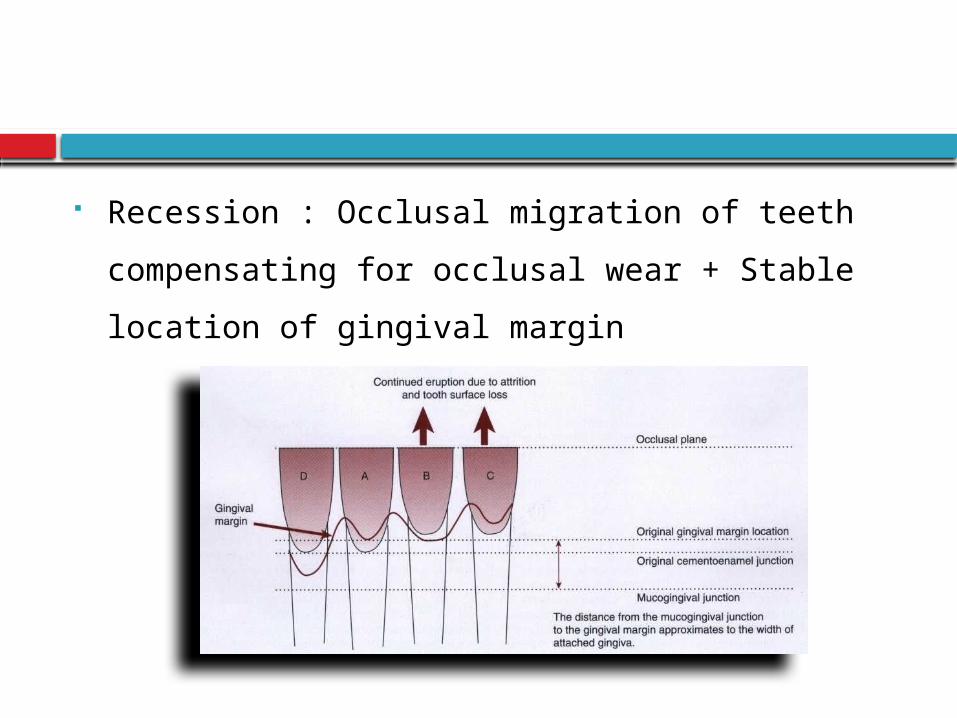
Recession : Occlusal migration of teeth
compensating for occlusal wear + Stable
location of gingival margin
In contrast Recession Mechanical trauma e.g. tooth brushing
Loe et al 1978 Extrusion of teeth
Batenhorst et al 1974
Occlusal movement of teeth does not imply apical
migration of JE
Manson 1963, Anneroth & Ericsson 1967, Loe 1967
Gingival Connective Tissue
Coarser & dense
Rate of maturation changes
Cellular elements
Rate of collagen synthesis
Soluble - Insoluble collagen
Mechanical strength
Denaturing temperature
Collagen stabilization
Conclusion
knowledge of architecture of the gingiva, how the tissue
structure develops & how it relates to function is fundamental
importance for understanding the disease process, and for
devising effective therapeutic strategies
Newman MG, Takei HH, Klokevold PR, Carranza FA. Carranza’s Clinical Periodontology. Saunders Elsevier;10th Edition.
Lindhe, Karring, Lang: Clinical Periodontology & Implant Dentistry. Blackwell Munksgaard; 5th Edititon.
P. Mark Bartold, Laurence J. Walsh & A. Sampath Narayanan. Molecular and cell biology of the gingiva. Periodontology 2000, Vol. 24, 2000, 28–55.
D.D. Bosshardt and N.P. Lang. The Junctional Epithelium: from Health to Disease. J Dent Res 2005; 84(1); 9-20.
Thomas M. Hassell. Tissues and cells of the periodontium. Periodontology 2000, Vol. 3, 1993, 9-38.
Van Der Velden. Effect of age on the periodontium. Journal of Clinical Periodontology 1984: 11; 281-294.
Marja T. Pollanen, Jukka I. Salonen & Veli-Jukka Uitto. Structure and function of the tooth–epithelial interface in health and disease. Periodontology 2000, Vol. 31, 2003, 12–31
Stern IB . Current concepts of the dentogingival junction: The epithelial and connective tissue attachments to the tooth. J Periodontol 1981;52:465-476.
References

![Relationship of Facial Skin Complexion with Gingiva …...Ibuski, reported that the color of the gingiva varied with the position of the papillary, marginal and attached gingiva [9]](https://img.pdfslide.us/doc/110x75/5e61b02ebfe26e503169c604/relationship-of-facial-skin-complexion-with-gingiva-ibuski-reported-that-the.jpg)