Embed Size (px)
Citation preview

FIRST AID IN CARDIAC ARREST
CPR and AED USE

Definition:•The immediate care given to a person who is injured or ill.
Principle goals:•Ensure the safety of rescuer and patient.•Identify the causes of injury.•Stabilize the neck and care for life threatening injuries.•Arrange for transportation.•Continue patient assessment
First Aid Review
Definition
CARDIAC ARREST: Abrupt cessation of
cardiac pump function which may be
reversible by a rapid intervention but
will lead to death in its absence.
DEATH: Irreversible cessation of all
biologic functions
At the end of this session participants should be able to demonstrate:
How to assess the collapsed victim
How to perform chest compression and rescue breathing (CPR)
How to operate an automated external defibrillator safely
How to place an unconscious breathing victim in the recovery position
Objectives

To remember

MECHANISMS OF CARDIAC
ARREST
50-80%: VF and PULSLESS VT
20-30%: Asystole, severe
bradycardia and pulseless electrical activity
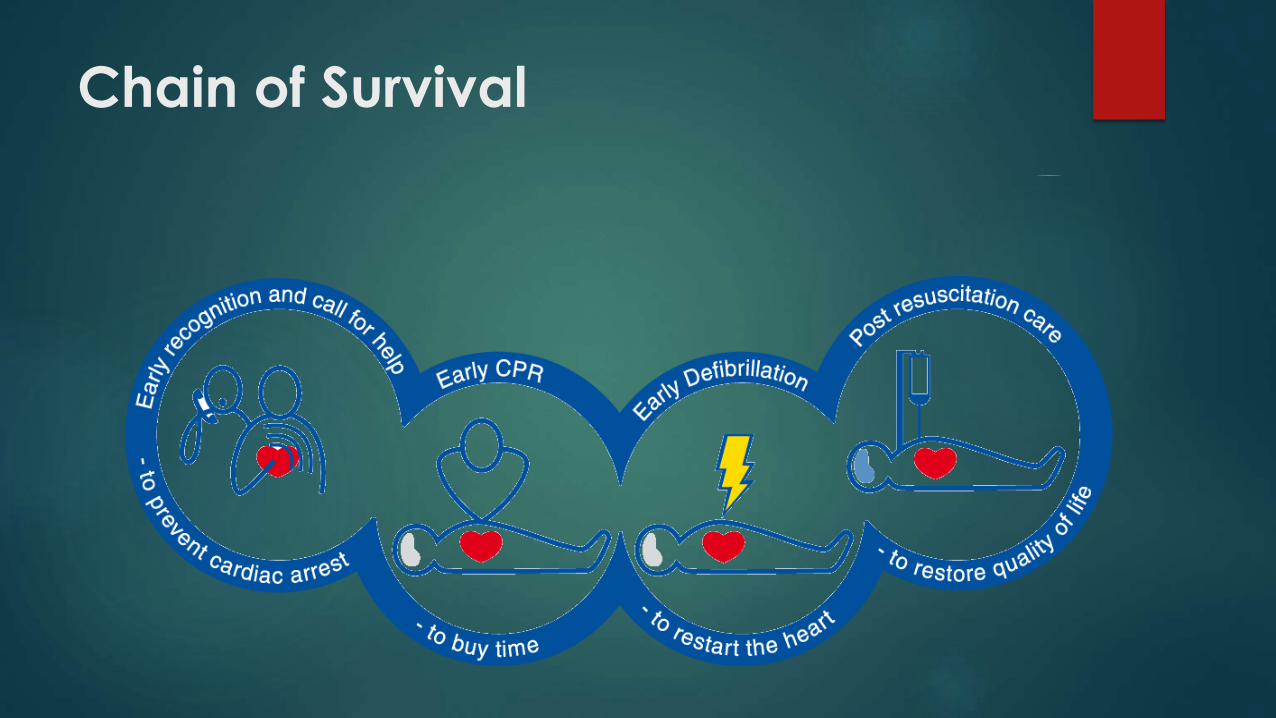
Chain of Survival

Check response
Shake shoulders gently
Ask “Are you all right?”
If he responds
• Leave as you find him.
• Find out what is wrong.
• Reassess regularly.
Recovery position
A position used for unconscious,
breathing casualties.
Maintains an open airway so the
casualty can breathe.

Primary Survey: ABCD
Airway
Breathing
Circulation
Defibrillation
Always assess and manage before moving on to the next step!
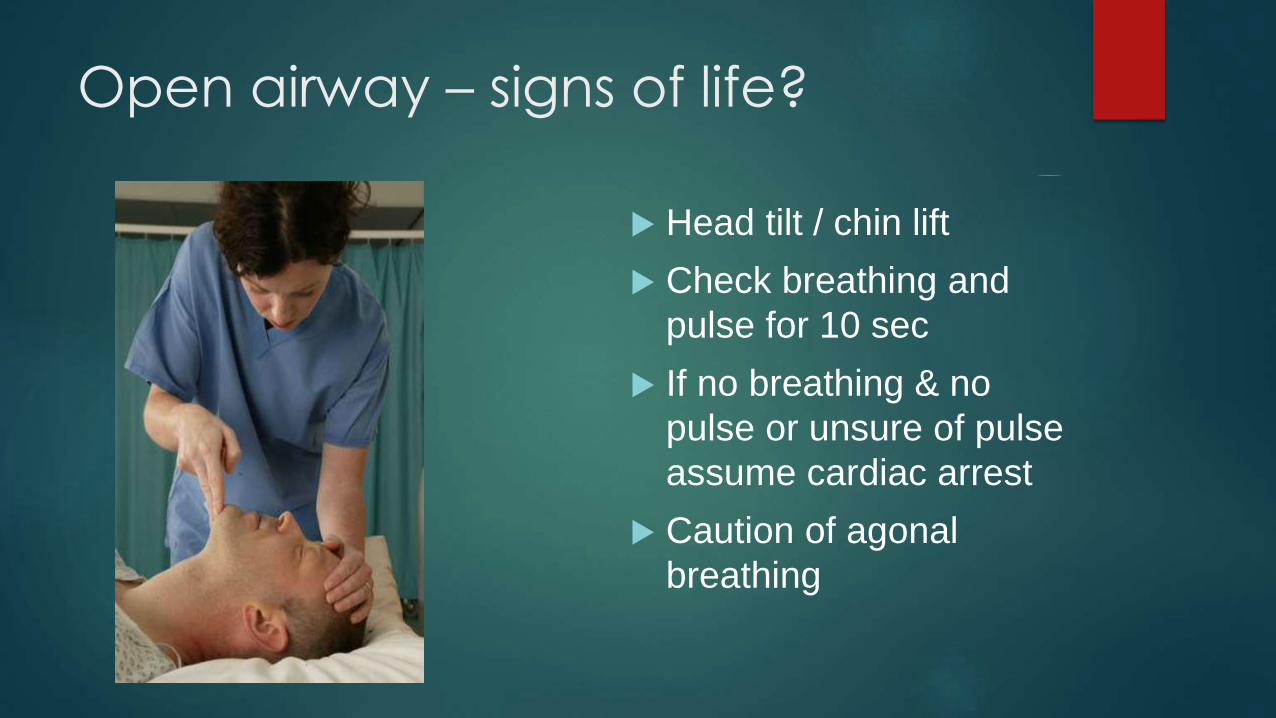
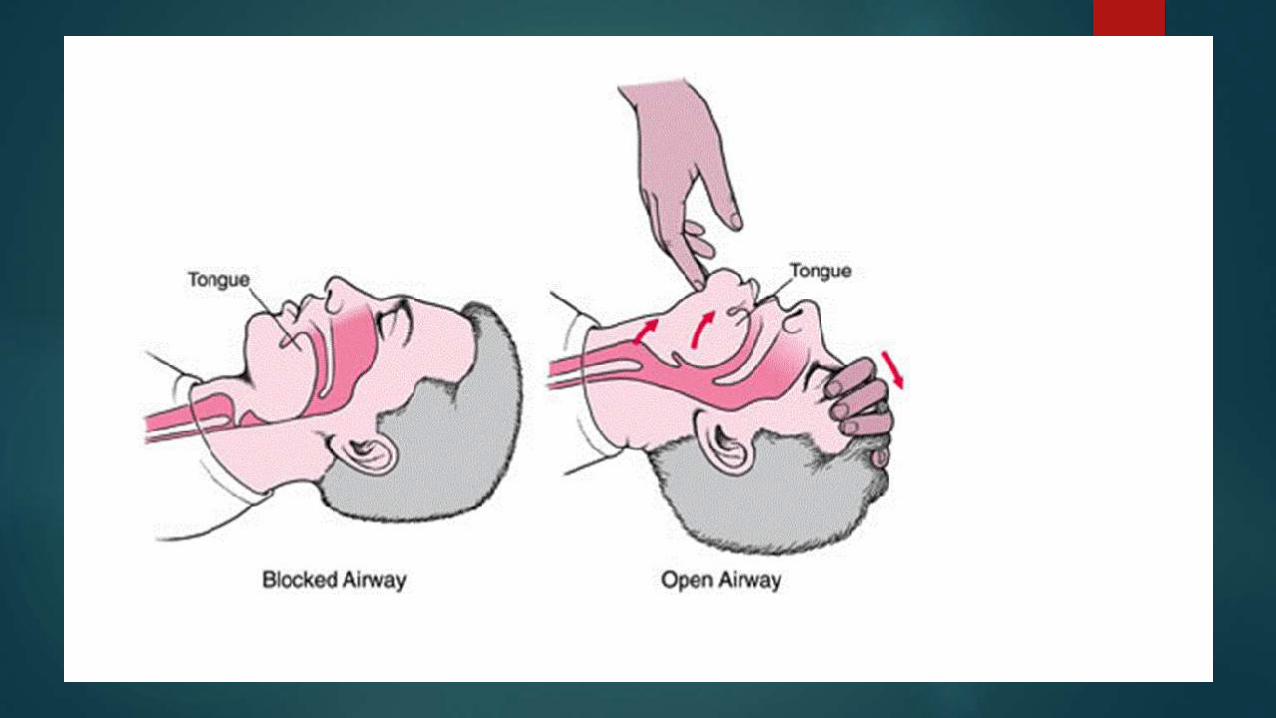
Open airway – signs of life?
Head tilt / chin lift
Check breathing and
pulse for 10 sec
If no breathing & no
pulse or unsure of pulse
assume cardiac arrest
Caution of agonal
breathing

If signs of life present
Look
ListenFeel

Breathing
Keeping the airway open, look, listen, and feel for normal breathing.
• Look for chest movement.
• Listen at the victim's mouth for breath sounds.
• Feel for air on your cheek.
In the first few minutes after cardiac arrest, a victim may be barely
breathing, taking infrequent, noisy, gasps. Do not confuse this with
normal breathing.
Look, listen, and feel for no more than 10 sec to determine if the
victim is breathing normally. If you have any doubt whether
breathing is normal, act as if it is not normal.
Decision to start CPR
Decision to start CPR is made if a victim is
unresponsive and not breathing normally.
Pulse check is no longer required, and is NOT
recommended for lay persons.
Pulse check has been shown to be unreliable,
with unacceptably high rates of false positives
and negatives.
START CPR
If he is breathing normally:
Turn him into the recovery position.
Send or go for help, or call for an ambulance.
Check for continued breathing.
If he is not breathing normally:
• Ask someone to call for an ambulance or, if you are on your own, do this yourself; you may need to leave the victim.
Start chest compression as follows:
Kneel by the side of the victim.
Place the heel of one hand in the centre of the victim’s chest.
Chest Compressions
Place hands on the center of the chest, rather than the ‘rib
margin’ method.
100/min for all victims (except newborns).
Allow chest to recoil to normal position after each
compression.
Use equal compression and relaxation times.
Limit interruptions in chest compressions, even for rhythm
check, shock delivery, advanced airway, or vascular
access.

30 chest compressions
Heel of hand in centre
of chest
Interlock fingers
Keep arms straight
Compress 4-5 cm depth
Rate of 100 min-1
Allow chest to recoil
Cardio-pulmonary resuscitation (CPR)
is a means to provide temporary
support to the coronary and cerebral
circulation, till normal cardiac output is restored

PERSON COLLAPSES
Check if he is unresponsive
Call emergency number
Get AED ( Automated External
Difibrillator )
Beginning the ABCD’s and CPR
Combine chest compression with rescue breaths
► After 30 compressions open the airway again using head
tilt and chin lift.
► Pinch the soft part of the victim’s nose closed, using the
index finger and thumb of your hand on his forehead.
► Allow his mouth to open, but maintain chin lift.
► Take a normal breath and place your lips around his
mouth, making sure that you have a good seal.
► Blow steadily into his mouth whilst watching for his chest to
rise; take about one second to make his chest rise as in
normal breathing; this is an effective rescue breath.
► Maintaining head tilt and chin lift, take your mouth away
from the victim and watch for his chest to fall as air comes
out.
►If your rescue breaths do not make the chest rise as in
normal breathing, then before your next attempt:
► Check the victim's mouth and remove any visible
obstruction.
► Recheck that there is adequate head tilt and chin lift.
► Do not attempt more than two breaths each time before
returning to chest compressions.
► If there is more than one rescuer present, another should
take over CPR about every 2 min to prevent fatigue.
► Ensure the minimum of delay during the changeover of
rescuers.
Automated External
Defibrillator
AED
While there are many styles of AEDs they all work the same. The first
step is to turn the unit on and follow the voice prompts.
CPR/AED

What is an AED?
Automated external defibrillator – is an computerized defibrillator
it can analyze heart rhythm
recognize shockable rhythm
advise the operator whether the rhythm should be shocked
very easy to use
AED’s computer chips analyze the rate, size and wave shape of human cardiac rhythm.
will not shock a properly functioning heart
will not shock a heart that has stopped – VF is not present
Defibrillation
Most frequent initial rhythm in witnessed sudden cardiac
arrest is ventricular fibrillation (VF) or pulseless ventricular
tachycardia (VT) which rapidly deteriorates into VF
The only effective treatment for VF is electrical defibrillation
Probability of successful defibrillation diminishes rapidly
over time
VF rapidly converts to asystole if not treated
Universal steps of AED use
Place AED parallel to patients left ear Power on the AED first
Some automatically turn on when opened
Attach the AED to the patients chest with electrode pads Remove clothing – to bear chest
Be kind to females
Dry patient or shave chest in area of electrode placement if needed
Place one pad above right nipple and one to the side and below the left nipple. (CPR is continued up to the point of placing the pads on)
Analyze rhythm Make sure everyone is clear (must say “stand clear of the victim”).
No contact
Push analyze
Charge AED if shock is required (some machine charge automatically)
Universal steps of AED use
Shock if indicated – (after checking everyone is clear
again)
Begin CPR for five cycles then analyze again
If shock is advisable again you clear everyone and
shock
If shock is not advisable – continue with CPR
If victim has pulse and is breathing put into recovery
position.
DO NOT take off pads or turn off AED until prompted by EMS
Special Considerations
Water Must remove victim from water or wet surface
Dry before attaching pads
Metal surfaces Is victim lying on metal surface? – if so move victim
The metal surface may cause the shock form the AED to hit you.
Children Children 8 and older use as soon as possible
Children 1-8 – CPR for two minutes before using AED
Transdermal medications Remove patch and wipe clean before attaching AED pads
Implanted pacemakers and defibrillators Do not place an AED electrode directly over implanted device.
Move at least one inch to the side of device
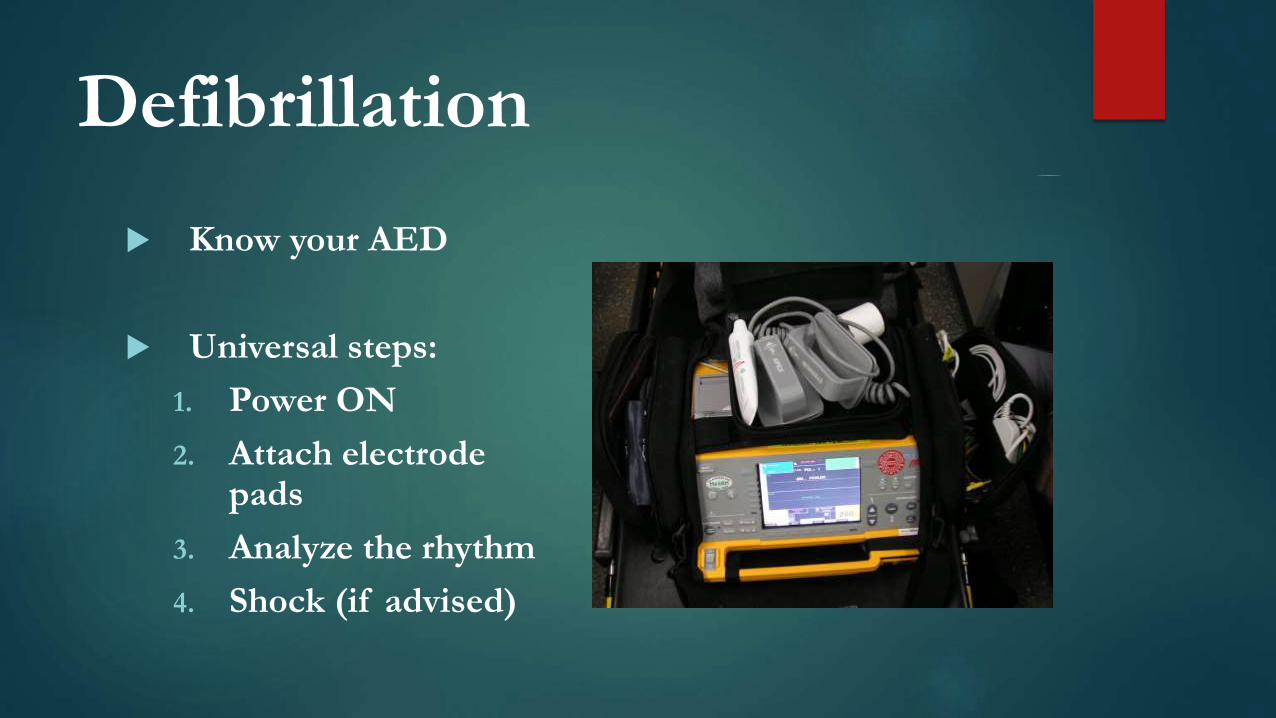
Defibrillation
Know your AED
Universal steps:
1. Power ON
2. Attach electrode pads
3. Analyze the rhythm
4. Shock (if advised)
Keep clear
5H’s and 5T’s
The H’s and T’s of ACLS is a mnemonic used to
help recall the major contributing factors to
pulseless arrest including PEA, Asystole,
Ventricular Fibrillation, and Ventricular
Tachycardia. These H’s and T’s will most
commonly be associated with PEA, but they will
help direct your search for underlying causes to
any of arrhythmias associated with ACLS
4H’s and 4T’s
The H’s include:
Hypovolemia,
Hypoxia,
Hyper/hypokalemia,
Hypothermia.
The T’s include:
Toxins,
Tamponade(cardiac),
Tension pneumothorax,
Thrombosis (coronary and
pulmonary),
Take Home Points
Assess and manage at every step before moving on to
the next step
Rapid defibrillation is the ONLY effective treatment for
VF/VT
Search for and treat the cause
Treat the patient not the monitor
Reassess frequently
Minimize interruptions to chest compressions