Embed Size (px)
Citation preview

GOOD MORNING

EPIDEMIOLOGY OF PERIODONTAL DISEASES
GUIDED BY, DR.LALIT MATHUR DR.BALAJI MANOHAR DR.RAJESH PILLAI DR.RAVIKIRAN N DR.NEEMA SHETTY DR.ADITI MATHUR DR MEETU JAIN DR. BARKHA MAKHIJANI
Seminar Presented By :
Dr. ABHISHEK GAUR

EPIDEMIOLOGY OF PERIODONTAL DISEASES
It doesn't matter how beautiful
your theory is,
what matters is how smart you are…

CONTENTS :1. Introduction
2. Definitions
3. History
4. Aims Of Epidemiology
5. Ultimate Aim
6. Objectives
7. Definitions
8. Bias - Definition
9. EPIDEMIOLOGY OF PERIODONTITIS (elaborated)
10. Sensitivity & Specificity11. EPIDEMIOLOGICAL STUDY DESIGN
12. EPIDEMIOLOGICAL TRIAD
13. WHAT IS A PERIODONTAL DISEASE ?
14. RATE OF BONE LOSS
15. HOW IS PERIODONTITIS MEASURED ?
16. EPIDEMIOLOGICAL STUDIES
17. PREVALENCE OF PERIODONTAL DISEASES IN INDIA
18. Conclusion
19. references

Introduction :
Ever since the Beginning of this Universe, mankind has struggled constantly against disease and the struggle is never ending. Continuously, day by day, new Diseases & health Problems come into existence which needs discovery of basic facts about the disease & the curative as well as Preventive measures in pursuit of its eradication.
An aggressive approach towards all this achieved by
“Epidemiology”

Definitions :
That Branch of medical Science which treats epidemics.(Thomas Parkin, 1873)
The science of the mass phenomena of infectious diseases.(Frost, 1927)
The study of the distribution & determinants of disease frequency in man.
(MacMohan, 1960)
The study of the distribution & determinants of health related states or events in specified populations, and the application of this study to the control of health problems
(John M. Last, 1988)
History :
1) THOMAS SYDENHAM (17th Century)
- Founder of Epidemiology
- History Of Disease
2) JOHN SNOW (1854)
-Father Of Epidemiology
3) WILLIAM BUDD (1811-1880)
-Physician & Epidemiologist
-Pioneer in The isolation of Infectious Diseases
4) W.H. FROST
First Professor of Epidemiology (U.S.)

AIMS OF EPIDEMIOLOGY
1) To describe the distribution & magnitude of Health disease problems in Human populations.
2) To Identify aetiological factors in the pathogenesis of disease.
3) To provide the data essential to the planning, implementation & evaluation of Services for the prevention, control of treatment of disease and to the setting up of priorities among those services.

ULTIMATE AIM :
1) To eliminate or reduce the health problem or its consequences.
2) To promote Health & Well Being of society as a whole.

OBJECTIVES :
1) To identify the etiology or the cause of a disease and the risk factors.
2) To determine the extent of disease found in the community.
3) To study the natural history & prognosis of disease.
4) To evaluate new preventive & therapeutic measures and new modes of Health Care delivery.
5) To provide the foundation for developing policy & regulatory decisions relating to environmental problems.

Some Definitions used :
Prevalence : Prevalence is the proportion of persons in a population who have the disease of interest at a given point in or period of time.
It is calculated by dividing the number of persons in the population who have the disease, by the number of persons in the population.
Information about Prevalence can be useful for estimating the need for health care resources. For example, Prevalence data on dental disease are used for estimating the number of new general dentists and specialists that dental school should train.
Carranza (10th Edition)

Incidence :
(also referred as risk or cumulative incidence)
It is the average percentage of unaffected persons who will develop the disease of interest during a given period of time.
Incidence can be viewed as the risk or probability that a person will become a case.
It is calculated by dividing the number of new cases of disease by the number of persons in the population who are at risk for the disease.
(Carranza, 10th Edition)

Probing Pocket Depth :
Distance from the gingival margin to the location of the tip of a periodontal probe inserted in the pocket with moderate probing force
Probing Attachment Level (PAL)
Or
Clinical Attachment Level (CAL) :
The distance from the Cemento – Enamel Junction (CEJ) to the location of the inserted probe tip is known as Probing Attachment Level (PAL) or Clinical Attachment Level (CAL).

EPIDEMIOLOGY OF PERIODONTITIS
Chronic periodontitis is the most common form of destructive periodontal diseases and shows a slow disease progression characterized by bursts of disease activity separated by quiescent periods of varying durations.
Aggressive periodontitis encompasses aggressive, rapidly progressive forms of periodontitis, which often commence during adolescence and early adulthood.
Pre-pubertal periodontitis, juvenile periodontitis & rapidly progressive periodontitis all are considered forms of aggressive periodontitis.

Sensitivity & Specificity :
When a diagnostic test for a disease or condition gives a Positive result, the result can be correct (true positive) or incorrect (false positive).
When a test gives a negative result, the result can be true (true negative) or false (false negative) (as shown in Table 1).
The ability of a test to give a correct answer is indicated by its Sensitivity and Specificity.
(Carranza 10th Edition)

TEST RESULT DISEASE NO DISEASE
Positive A(True Positive)
B(False Positive)
Negative C(False Negative)
D(True Negative)
Sensitivity A ÷ (A+C)
Specificity D ÷ (B+D)
Positive predictive value A ÷ (A+B)
Negative predictive value D ÷ (C+D)

Sensitivity :
Sensitivity of a Test is the Proportion of subjects with the disease who test positive.
A highly sensitive test is unlikely to be negative when someone has the disease.
The clinician should choose a highly sensitive test when the consequences of not identifying a person with a disease could be severe, such as during testing for Human Immunodeficiency Virus (HIV).
Specificity :
The specificity of a test is the proportion of subjects without the disease who is negative.
A highly specific test is unlikely to be positive when a person does not have the disease.
Specific tests are especially indicated when the misdiagnosis of disease in the absence of disease could harm a person emotionally, physically, or financially.

EPIDEMIOLOGICAL STUDY DESIGN
STUDY DESIGN
EXPERIMENTAL A.) COMMUNITY
INTERVENTION TRIALS
B.) RANDOMIZED CLINICAL TRIALS
C.) FIELD TRIALS
OBSERVATIONAL
ANALYTICAL
1.CASE CONTROL2.COHORT
3.CROSS SECTIONA
L4.
ECOLOGICAL

Descriptive studies1. Usually the first phase of an epidemiological investigation.
2. Concerned with observing the distribution of disease or health related characteristics in human population & identifying the characteristics with which the disease in question seems to be associated.
The various procedures involved are:
a) Defining the population to be studied
b) Defining the disease under study
c) Describing the disease by time, place and person
d) Measurements of disease
e) Comparing with known indices
f) Formulation of an etiological hypothesis

Analytical Studies:• Most often used in studies to determine the etiology of disease.• Establish that a causal relationship exists between a factor and a disease.
Case-Control Studies:• Retrospective study• Common first approach to test the causal hypothesis.• Involves 2 populations –
cases and controls• Case- control studies are basically
comparison studies.
1 EXPOSURE & OUTCOME
HAVEOCCURRED
BEFORESTART OF
STUDY
3. IT USES A CONTROL OR
COMPARISSION GROUP TO
SUPPORT OR REFUTE ANINFERENCE
2. THE STUDY
PROCEEDS BACKWARDS
FROM EFFECTTO CAUSE

Major advantages & disadvantages of case-control study
ADVANTAGES DISADVANTAGES
May study several exposures. Potential bias from sampling two populations
Short duration Does not establish sequence of events
Relatively inexpensive Potential bias in measuring predictors
Relatively small Potential survivor bias
Yields odds ratio (measure of association)
Does not yield incidence or true relative risk (measure of association)

Cross sectional studies• This study is usually carried out for descriptive purposes only, although their
results can sometimes be analyzed for association between disease outcome & exposure.
• Based on single examination of a cross-section of population at one point of time.
• This study is More useful for chronic than short lived disease.• It Also provides information about disease prevalence and natural history of
disease.
Major advantages & disadvantages of cross-sectional study
ADVANTAGES DISADVANTAGES
May study several outcomes Not feasible for rare diseases
Short duration Does not establish sequence of events
A good first step for a cohort Potential survivor bias
study
Potential survivor bias
Yields prevalence Does not yield incidence or true relative risk (measure of association)

Ecological studies• The unit of analysis is a group of persons rather than an
individual.• This study design has not been frequently used in the study
of periodontal diseases.
Experimental studies• In observational studies, the researcher is a spectator of the
natural course of the disease.• In contrast, in experimental studies the researcher has
control over the exposure of interest & assigns subjects to exposed or non-exposed groups, or to different treatment & no treatment groups.
• The researcher may also control the characteristics of the exposures & factors that may influence the subjects response to such an exposure.

Major advantages & disadvantages of experimental study
ADVANTAGES DISADVANTAGES
Can produce the strongest evidence for cause and effect
Costly in time and money
Only possible design for some research question (new drug)
Many research questions are not suitable: ethical barriers or outcome too rare
Can sometimes be faster and cheaper
Reduced generalizability (standardized interventions may be different than common practice)
Tend to restrict the scope and narrow the study question

Cohort study
• It is a prospective study.• A group of people are observed over a period of time,
during which some of the group develops the disease under study & some do not.
• “Cohort” is a group of persons who share a common experience within a defined time period ; for example, age ,occupation , pregnancy, etc.
• The association between exposure & disease outcome can then be determined.

Major advantages & disadvantages of cohort study
ADVANTAGES DISADVANTAGES
Establish sequence of events Often requires large sample sizes
Avoids bias in measuring predictors Not feasible for rare diseases
Avoids survivor bias Expensive
Can study several outcomes Long duration
More control over selection of subjects
More control over measurements
Yields incidence, relative risk (measure of association)

Strengths in Cohort vs. Case-control?Cohort study Case-control study
Rare exposure Quick & inexpensive
Examine multiple effects of a single exposure.
Well-suited to the evaluation of diseases with long latency Period.
Minimizes bias in theexposure determination.
Rare diseases.
Direct measurements of incidence of the disease.
Examine multiple etiologic factors for a single disease.

Limitations in Cohort vs. Case-control?
Cohort study Case-control study
Not rare diseases Not rare exposure
Prospective: Expensive and time consuming
• Incidence rates cannot be estimated unless the study is population based
Retrospective: inadequate records
Selection Bias and recall bias
Validity can be affected by losses to follow-up

EPIDEMIOLOGICAL TRIAD
HOST
AGENTENVIRONMENT

WHAT IS A PERIODONTAL DISEASE ?G
ingivitis
Periodontitis
PERIODONTAL
DISEASES
Gingivitis & Periodontitis :
GINGIVITIS :“Inflammation Of Gingiva”
It is the inflammation of the Gingiva in which the junctional epithelium remains attached to the tooth at its original level.
PERIODONTITIS :
It is the inflammatory process which involves the Gingiva and the periodontium & loss of periodontal attachment has occurred.
(Jan Lindhe 5th Edition)
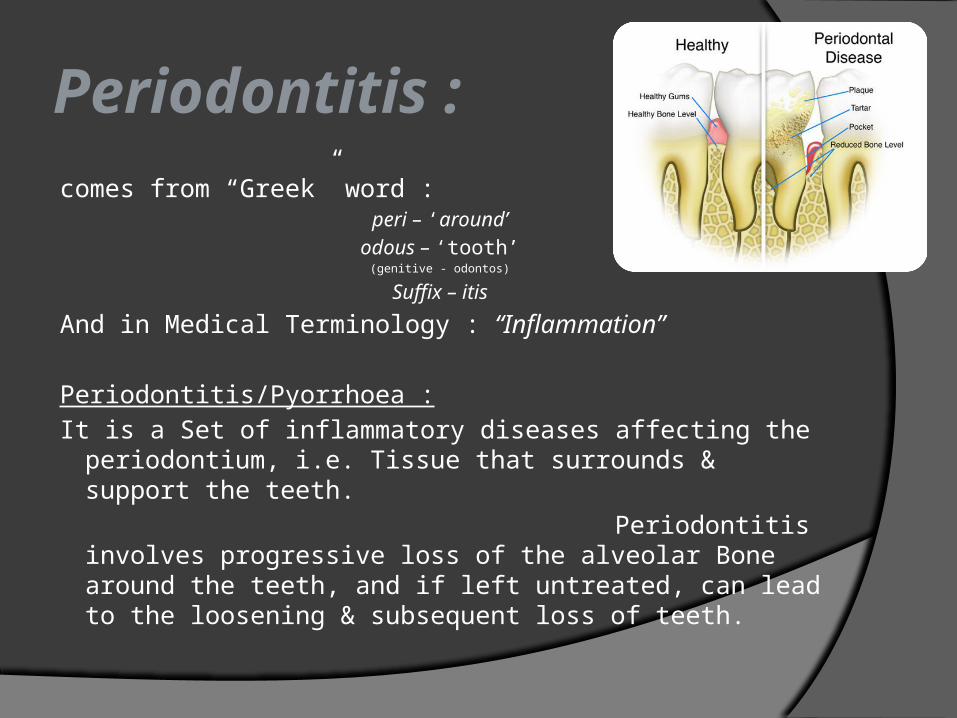
Periodontitis :
comes from “Greek” word :peri – ‘around’
odous – ‘tooth’(genitive - odontos)
Suffix – itis
And in Medical Terminology : “Inflammation”
Periodontitis/Pyorrhoea :
It is a Set of inflammatory diseases affecting the periodontium, i.e. Tissue that surrounds & support the teeth.
Periodontitis involves progressive loss of the alveolar Bone around the teeth, and if left untreated, can lead to the loosening & subsequent loss of teeth.

ETIOLOGY OF PERIODONTAL DISEASE
ETIOLOG
Y
LOCAL
FACTORS
SYSTE
MIC FACTORS

LOCAL & SYSTEMIC FACTORS
A) LOCAL FACTORS :
1) Plaque
2) Calculus –
a) Supra-Gingival Calculus
b) Sub-Gingival Calculus
3) Materia Alba.
4) Faulty Dentistry.
5) Abnormal Habits.
6) Food Impactions.
7) Diet.
8) Improper Tooth Brushing.
9) Abnormal Anatomy.
10) Erupting teeth.
11) Factors of Occlusal Functions.

B) SYSTEMIC FACTORS :
1) Nutrition.
2) Vitamins.
3) Protein Deficiency.
4) Blood Dyscrasias.
5) Endocraniological Disorders.
6) Pituitary Disorders.
7) Allergies
8) Drug Idiosyncrasies.
9) Radiations.
10) Psychogenic Factors.

RATE OF BONE LOSS
Loe and associates in 1986 did a study on Sri Lankan tea labourers with no oral hygiene and no dental care and found that the rates of bone loss on an average to be about 0.2 mm a year for facial surfaces and about 0.3 mm a year for proximal surfaces, when periodontal disease is allowed to progress untreated.

However, the rate of bone loss may vary, depending on the type of disease present.
Löe et al identified the following three subgroups of patients with periodontal disease based on interproximal loss of attachment and tooth mortality:
1. Approx. 8% of persons had rapid progression of periodontal disease, characterized by a yearly loss of attachment of 0.1 to 1.0 mm.
2. Approximately 81% of individuals had moderately progressive periodontal disease, with a yearly loss of attachment of 0.05 to 0.5 mm.
3. The remaining 11% of persons had minimal or no progression of destructive disease (0.05 to 0.09 mm yearly).

An Epidemiologic Survey performed during the 1950s in India, used assessments of alveolar Bone height to distinguish between gingivitis & destructive periodontal disease, in a sample involving 1187 dentate subjects.
(Marshall Day et al 1955)
1) A 100 % occurrence of destructive periodontitis after the age of 40 yrs has been seen.
2) A decrease in the percentage of studies with “Gingival disease without any Bone involvement” with increasing age concomitant with an increase in percentage of subjects with “Chronic destructive periodontal disease”
(Jan Lindhe 4th & 5th Edition)
In a study of un-referred patients to ‘Glasgow Dental Hospital, United Kingdom’, which included :
1. Number Of Subjects : 74
2. Age : 50 yrs (30) to 73 yrs (44)
3. 54 % subjects : optimum Bone Height
4. 5 % Subjects : Generalized advanced Bone Loss (defined as bone loss in 50 % or more remaining teeth)
5. 20 % subjects : Three Quarters of the teeth with advanced Bone loss.
Also, Findings from other epidemiologic studies from the same period, verified a high prevalence of destructive periodontal disease in the adult population in general, and a clear Increase in disease prevalence with ‘Age’
(Jan Lindhe 5th Edition)

The model of the pathogenesis of the periodontitis in the 1950s to 1970s was predicated on the following beliefs:
1. All individuals were equally susceptible to periodontitis.
2. Long standing gingivitis invariably progresses to periodontitis with subsequent tooth loss.
3. Susceptibility to periodontal disease increases with increasing age.
4. Risk for periodontal disease was determined by environmental factors alone.

HOW IS PERIODONTITIS MEASURED ?
Periodontal Index :
1) Periodontal Index (by Russell A.L. in 1970)
2) Periodontal Disease Index (by Sigurd P. RamfJord in 1959)
3) Gingival Periodontal Index (O. Leary T.J., Gibson W.A., Shannon I.L., Schuessler
C.F. & Nabers C.L. In 1963)
4) Extent & Severity Index (J.P. Carlos, M.D. Wolfe & A. Kingman in 1986)
5) Community Periodontal Index (CPI)
6) Community Periodontal Index Of Treatment Needs (CPITN) (“Joint working committee” of the ‘World Health Organization’ & ‘Federation Dentaire’)
By Jukka Ainamo, David Barmes, George Beagrie, Terry Cutress, Jean Martin & Jennifer Sardo-Infirri in 1982

For the Assessment of Plaque :
1) Oral Hygiene Index (By Vermillion & Greene in 1960)
2) Oral Hygiene Index – Simplified (Vermillion & Greene in 1964)
3) Turesky – Gilmore – Glickman Modification Of the Quigley Hein Plaque Index (Turesky & colleagues in 1970)
For the Assessment of Calculus :
1. Calculus Surface Index (By Ennever Sturzenberger C.P. & Radike A.W. in 1961)
2. Calculus Surface Severity Index (CSSI)(By Enneverj et al 1961)

EPIDEMIOLOGICAL STUDIES IN INDIA
National Oral Health Survey And Fluoride Mapping (2002-2003)
First ever National level Epidemiological Survey done in India. Was Conducted by : “Dental Council of India” Subjects taken were : 210 (rural) & 110 (urban) Age Groups were : 12, 15, 35-44 , 65-74 years. Highest Prevalence of Periodontal Disease was in 35-44 yrs ( 89.6%)
and Lowest in of 12 yrs ( 57%) subjects. Calculus was more than bleeding in subjects aged 15yrs and above Prevalence was more in males. Comparatively, Higher prevalence was in rural subjects.

PREVALENCE OF PERIODONTAL DISEASES IN INDIA
YEAR REFERENCE AREA AGE (in Years) SAMPLE SIZE CLINICAL PARAMETERS
RESULTS/FINDINGS
2009 Kumar TS, Dagli RJ et al (7)
Bhill Adults in Southern Rajasthan
15-54 years 1590 (male) subjects
OHI-S & CPITN Debris, calculus & OHI-S increased with ageShallow pockets were prevalent (40%) in35-44 years age·Deep pockets were common (11%) in olderIndividuals.
2009 Parmar G, Sangwan P et al. (8) - Mean age 32
YEARS365 subjects :Areca nut & Tobacco Chewers – 168 &Non-chewers – 197
OHI-S & Clinical examination for ulcers and Burns etc.
Periodontal pocket are higher in Areca nut & TobaccoChewers
2008 S Nagarajan, Puspanjali K.
Bangalore 20-44 years 216 patients •Self administered questionnaire•Periodontal examination•Loe & Silness CPITN• Mobility
•Perceived periodontal health status was low.•The awareness increased with increasing severity of the disease
2008 Kumar S,Dagli RJ et al (15)
Rajasthan 18-25 years26-34 years35-44 years45 year and above
513 (male) subjects
•WHO oral health assessment form.•Clinical examination by method by WHO oral health survey
•Prevalence was 98.2%•Prevalence increased with increasing age.•Maximum disease was present in35-44 -45 years of age.•On an average 0.4% sextant having deep probing depth.

YEAR REFERENCE AREA AGE (in Years) SAMPLE SIZE CLINICAL PARAMETERS
RESULTS/FINDINGS
2007 Vandana KL, Sesha Reddy M (17)
Davanagere distt.
15-74 years 1029 subjects •CPITN•OHI-S•Jackson’s Fluorosisindex
1)With increasing age gingivitis reduce from85% to 42.9% and periodontitis increased18% to 57%.2) With increased severity of Fluorosis.3) Severityof gingivitis reduced 89.4% to 64% andperiodontitis increased from 8.5% to 35.8%.
2007 Dhar V, Jan A et al (18)
Udaipur distt. - 1587Government school children
- Gingivitis was found in 84.37% of children,Malocclusion in 36.42% and Fluorosis in36.36%

YEAR REFERENCE AREA AGE (in years) SAMPLE SIZE CLINICALPARAMETERS
RESULTS/FINDINGS
2005 Kumar M,Chandu GN et al (22)
- -220 Psychiatric Patients
CPITNOHI-SDMFT
Lower prevalence of caries with poor oral hygiene & extensive Needs for dental Treatment
2005 GPI Singh,J Bindra et al.(23)
Ludhiana - 1000 subjects•500 : Rural•500 : Urban
Assessment according to WHO
2005 Sood .M. (24) Ludhiana - 1000 subjects•500 : Rural•500 : Urban
•Assessment according to WHO•Oral Health assessment Form
Periodontal disease prevalence as well as severity was more in Smokers & Coronary artery Disease Patients.
RESULT URBAN RURAL
Bleeding 68.8% 69.2%
Calculus 96.8% 97.2%
Shallow Pockets
42.3% 31.7%
Deep Pockets
22.9% 11.0%

YEAR REFERENCES AREA AGE (in Years) SAMPLE SIZE CLINICAL PARAMETERS
RESULTS/FINDINGS
1997 Alexandra S. et al (33)
Mysore 7-17 years 817 (Tibetan School Children)
•Bleeding•Calculus•Malocclusion
•Malocclusion & Calculus were more in Girls.•Significantly, Increase in Bleeding among 8-13 yrs & 17 yrs old Girls than Boys
1993 Rao .S., Homagain .S. (44)
Adult rural Community
20-64 years 575 Subjects CPITN High Prevalence of periodontal diseases – 99.6%Greater Treatment Needs in Males than in Females.
1990 Anil S., Hari S et al (49)
Trivandrum distt., Kerala
•15-19 years•25-29 years•35-44 years
2756 (subjects)
Male : 1354Female : 1402
CPITN •15-19 yrs age group :Calculus & Bleeding was common (86%)•25-29 yrs age group : Calculus & shallow pockets (80%)•35-44 yrs :Calculus & Deep Pockets (33%)

CONCLUSION
• Periodontal diseases are one of the more prevalent oral diseases affecting more than 50% of Indian community.
• Untreated chronic periodontitis is responsible for tooth loss in majority of the cases.
• Constant presence of chronic inflammation and inflammatory mediators has also been proved to be a significant risk factor of several systemic diseases e.g. preterm low birth weight babies, coronary artery diseases, diabetes mellitus etc.
• Foreseeing the bad effects of periodontal diseases on oral as well as general health, the prevention of these diseases should be included in national health programme and national oral health survey should be conducted to get meaningful data for different oral diseases and plan around preventive/curative measures.

References :• Fermin A. Carranza (10th Edition)• Journals Of Periodontology, 1999• Jan Lindhe (4th & 5th Edition)• Journals Of Periodontology, 1998; Volume 16; Epidemiology of periodontal
disease among older adults• Journals Of Periodontology; 2001, June 2001; Vol. 26 Issue 1.• Soben - peter• JOHCD Prevalence of Periodontal Diseases in India• Journal of Indian Society Of Periodontology• JOP (Journals Of Periodontology) 2005• J Int. Acad Periodontol; PMC 2006 January 25• Indian Journal of Community Medicine 2005-10-2005-12;30(4)• Indian Journal of Community Medicine 2005-04-2005-06;30:2• Indian J Dent Res 2003;14(4):289-297• J Indian Soc Pedod. Prev. Dent 1997;15(4):114-117