Embed Size (px)
Citation preview

ELECTRIC STIMULATION
Dr. V. Giridhar Boyapati
USES
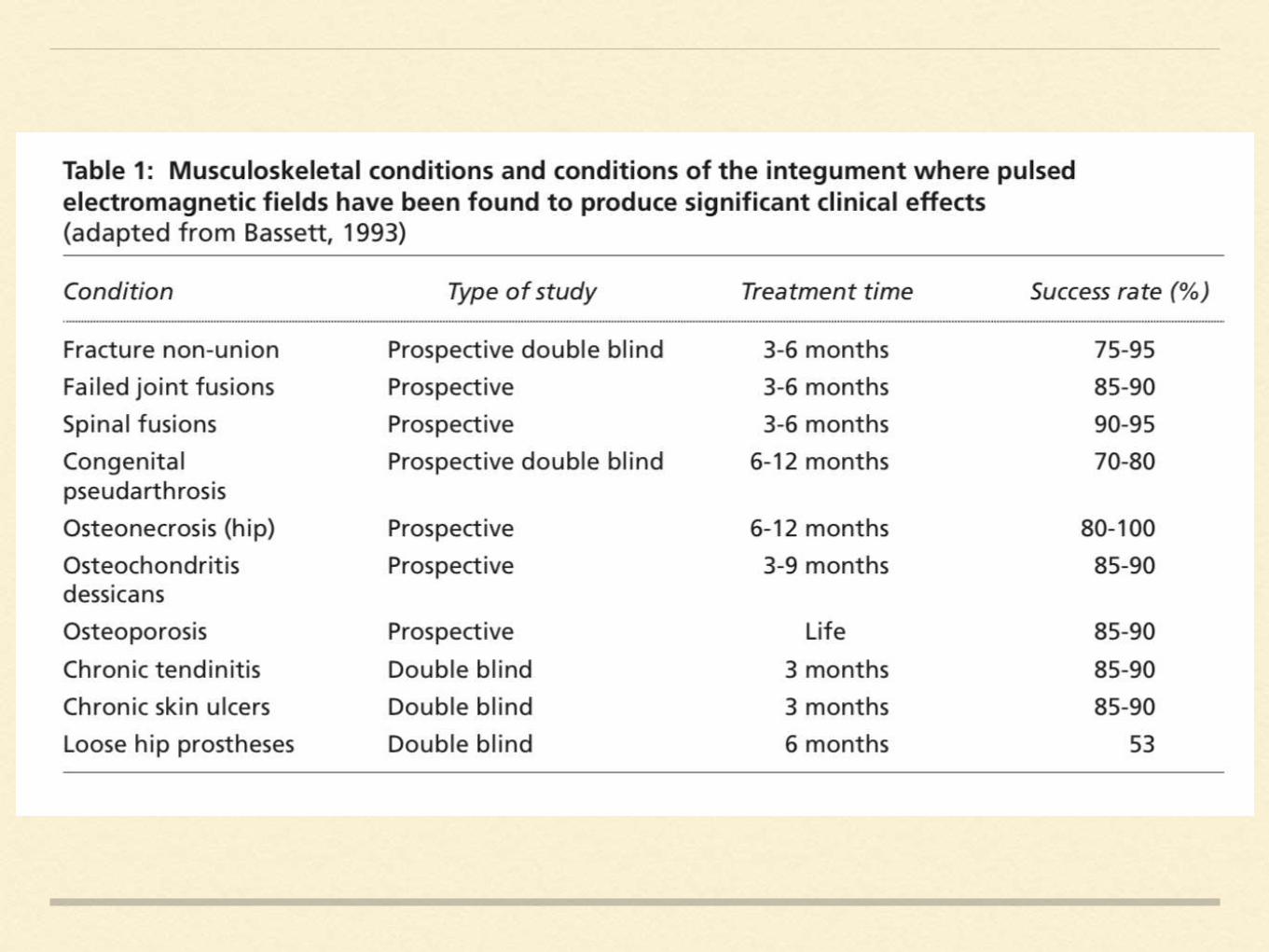
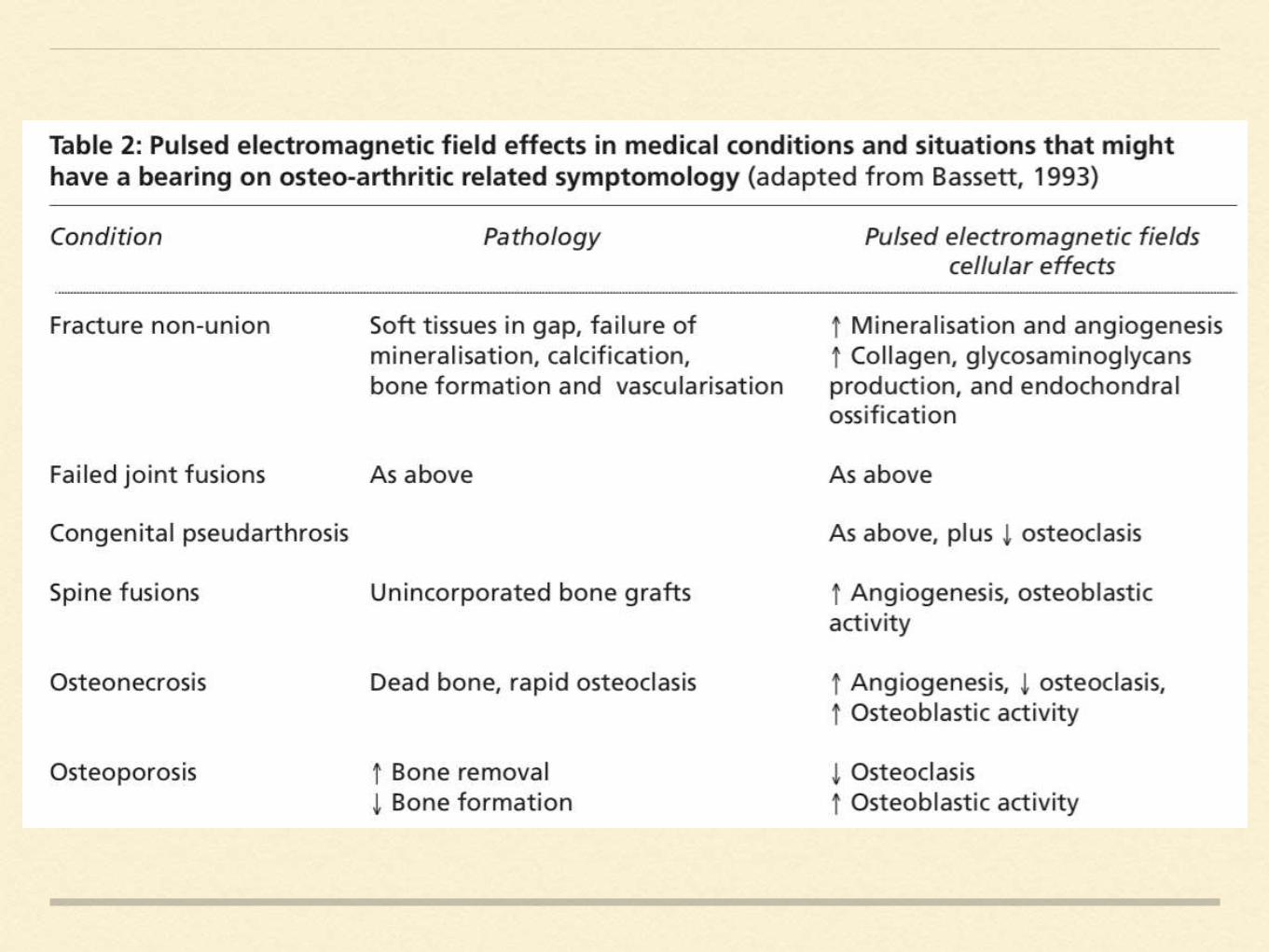
Treatment of Non union
Pseudoarthrosis
Failed fusion
Enhancement of fresh fracture healing
Treatment of AVN
Loosened prosthesis
ELECTRIC STIMULATION
Results in a series of biochemical events:
changes in the ion binding at membranes
changes in enzymatic activity ( c AMP)
Modification in mitochondrial activity
Alteration in macromolecular synthesis like collagen,RNA,
proteoglycans
Mechanical stressed bone generates an electric potential.
Areas of compression > Electronegative
Areas of tension > Electropositive
These stress generated potentials are due to :
1. Piezoelectric property
2. streaming potentials

CHEMICAL
MECHANICAL
THERMAL STIMULUS > Electric stimulus
> change in the cellular micro environmental
conditions
> callus formation
ELECTRIC STIMULATION
cathode
Ideal current 0.001-1 micro A / mm2
Ideal voltage 0.1- 10 mV / Cm
Amperage of more than 30 micro amp causes
osteonecrosis
Anode causes local tissue necrosis
ELECTRICALLY INDUCED OSTEOGENESIS
Around the cathode : pO2 is decreased
pH is increased
Produce hydrogen peroxide
• Bone grows best at hypoxic environment
• Active areas of bone growth and repair are electronegative
• Electric stimulation > stimulate Adenyl cyclase a hormone
receptor with in the membrane > cyclic AMP levels raise >
• stimulate DNA synthesis and cell division,
• tissue and cell proliferation,
• increased collagen synthesis,
• increase mineralisation,
• interfere with PTH activation,
• altered prostaglandin synthesis.
• specific changes in genetic transcription
BIOLOGICAL RESPONSE
Augmentation of normal reparative process in bone.
Endochondral or / and Inramembranous bone is formed.
Electrically stimulated bone is indistinguishable from that formed
by trauma and mechanical stimulation.
Fresh fractures, ostetomies or cortical defects show early
enhancement of bone, osteoid, and mechanical strength.
Most successful osteogenic model is with Intramedullary implant
model with proximate electrodes.
MODE OF ACTION
DIRECT INTERACTION OF ELECTRIC CURRENT WITH
CELLS
Electric field may displace membrane bound ions and
influence ionic fluxes with in the cell
calcium ion influx changes
calcium release from intracellular stores
Electrochemical relaxation of cell membrane
INDIRECT INTERACTION MECHANISM
Faradic electrochemical reaction near the electrode
Decrease local oxygen concentration
change in pH

CELLULAR RESPONSE MECHANISM
Mechanical interaction with peptide hormones like PTH;
it changes calcium fluxes, release adenyl cyclase and
phosphodiesterase > cyclic AMP > DNA and protein
synthesis.
Mechanical forces alter PGE2 > cyclic AMP
Electric fields effect adenyl cyclase and PGE2 > cyclic
AMP
Alter response of bone cells to PTH

NON ELECTROMAGNETIC RESPONSE
Electrode can provide a mechanical stimulus arising
from muscle activity and locomotion, producing a
osteogenic response.
Reactivity to implant material produce hypertrophic
osteogenic response.
BIOLOGY OF ELECTRICAL STIMULATION
• Musculoskeletal tissues respond to biophysical stimuli, including
weight-bearing, pulsed ultrasound, and electrical and electromagnetic
fields.
• Physiologically, endogenous electrical potentials and currents are
generated in these tissues when damaged and terminate when healed
• It is thought that these are part of a complex signaling network maintaining
normal bone remodeling and fracture healing.
• This current may provide a biophysical input to connective tissue cells
regarding the mechanical adequacy and needs of the extracellular matrix
(ECM)
• Nonunions,is a continuous lag phase.
• In these cases, devices that produce electric or electromagnetic field
tend to improve and amplify the physiological healing response by
driving electric or electromagnetic currents through damaged tissues.
DEVICES
Several electric stimulatory devices are employed , varying in the number
of coils, the electromagnetic intensity, the pulse frequency, the duration of
electric current administration,and the location of the coils. A device
employing a :
Direct electric current (DC),
Capacitive coupling (CC),
Inductive coupling (IC)
• Irrespective of the stimulant device used, a final common pathway exists
in the molecular cascade of healing stimulation by ES, that is,
1. Increase in the intracellular calcium,
2. Resulting in increased intracellular calmodulin
3. cell proliferation
• Local growth factors like Transforming growth factor (TGF) β1,
causes proliferation and differentiation of osteochondral cells and in the
stimulation of extracellular matrix (ECM) deposition
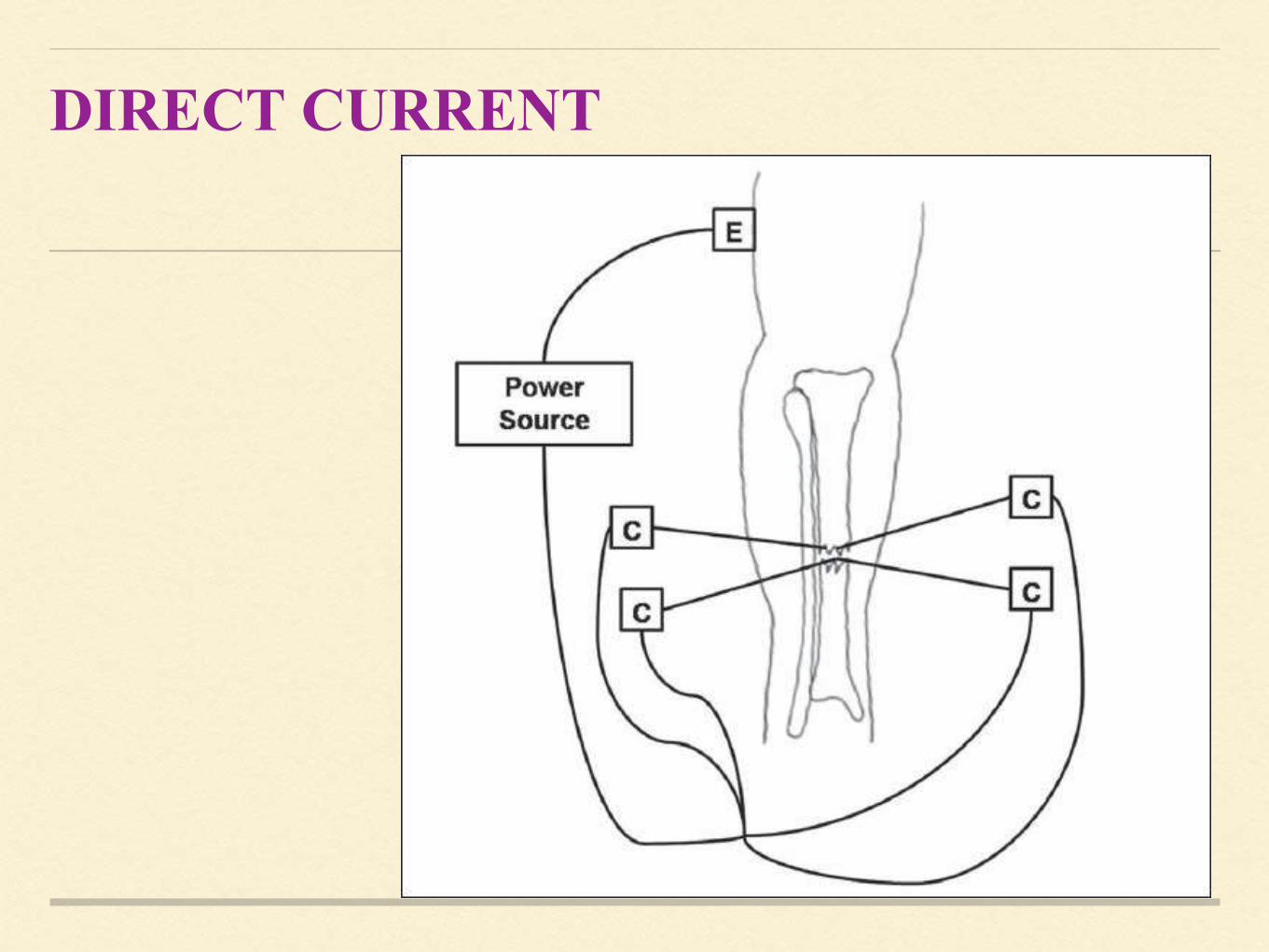
DIRECT CURRENT
Implantation of one or multiple cathodes into the bone
An anode is typically placed on the skin over the fracture site and a 5 to
100μA current is delivered.
In 1981, Brighton et al. published a case series using direct electrical
stimulation via four cathodes surgically implanted into a fracture
nonunion site for 12 weeks They found that four 20-μA cathodes applied
for 12 weeks produced solid bony union in 76.8% union.
Direct electrical current has also been used to promote healing of
Spinal fusion,
Ankle fusions and
Charcot foot reconstructions.
An electrochemical reaction occurring at the cathode is thought to
result in the osteogenic effects of direct electrical stimulation.
A Faradic reaction at the cathode has been shown to lower oxygen
concentration, increase pH, and produce hydrogen peroxide.
Decrease in oxygen concentration has been found to enhance osteoblastic
activity and decrease osteoclastic activity.
The direct electrical current also results in increased proteoglycan and
collagen synthesis.
Hydrogen peroxide may stimulate macrophages to release vascular
endothelial growth factor (VEGF), an angiogenic factor that is critical
for osteogenesis.
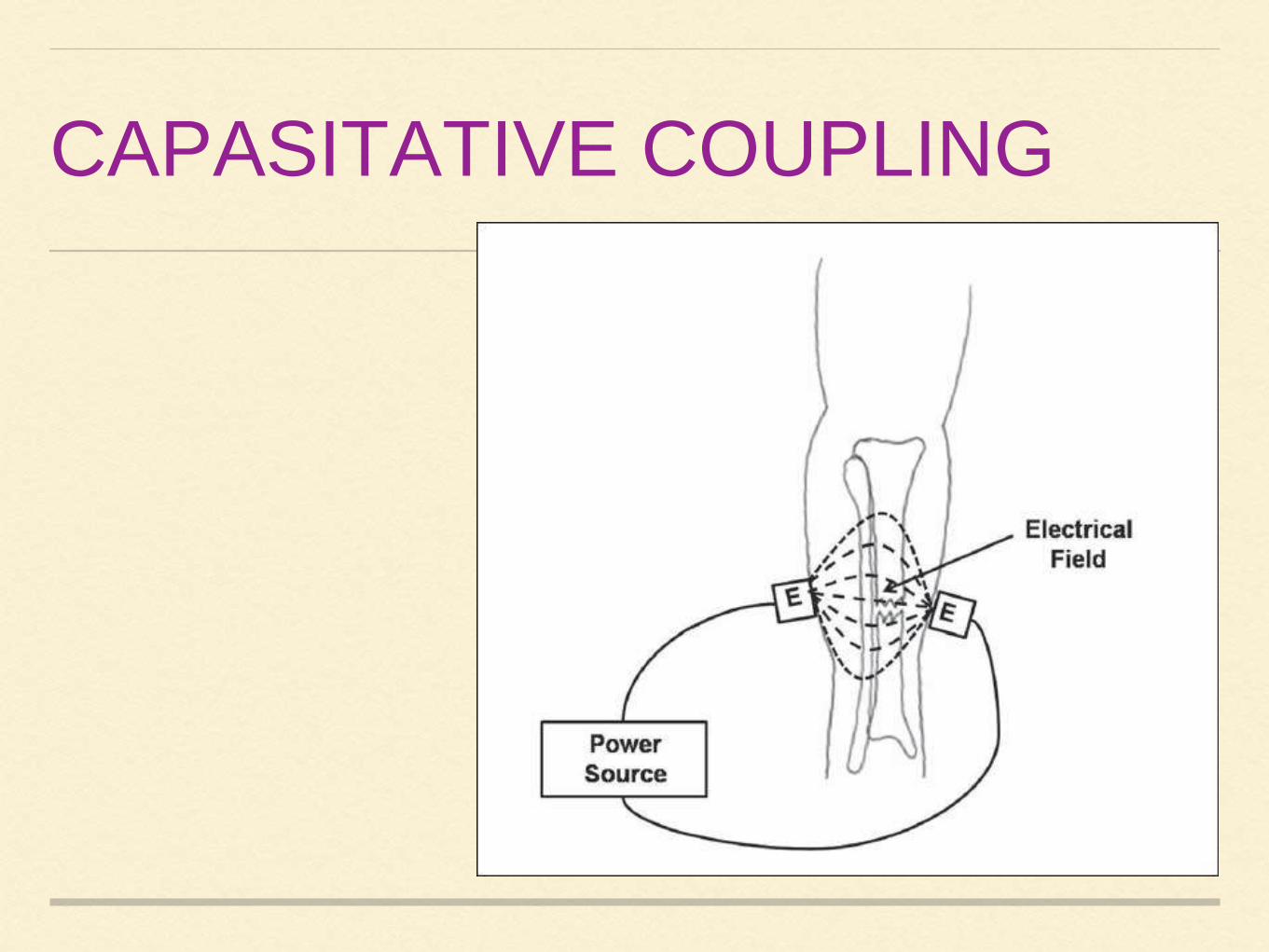
CAPASITATIVE COUPLING
Capacitive coupling is a noninvasive technique that involves placing
two electrodes on the skin overlying the fracture such that the
fracture site lies between the electrodes.
An alternating current is then used to create an electrical field within
the fracture site.
Potentials of 1-10 V at frequencies of 20-200 kHz are applied to the
electrodes, which result in the development of electric fields of 1-
100 mV/cm at the fracture site.
Brighton et al. found that the electrical field strength played a major role in
determining the proliferation of bone cells when exposed to a capacitive
coupling electric field.
Korenstein et al. found that there was a dose-dependent response to
capacitive coupled fields whereby Bone cell proliferation depend on :
1. Electrical field strength
2. Time the bone cells are exposed to the electrical field
Wang et al. found that capacitive coupling up-regulates the mRNA
expression for bone morphogenic proteins (BMPs)2, 3, 4, 5, 6, 7, and 8, as
well as gremlin and noggin.This increase in the production of growth
factors that are important for the proliferation and differentiation of
osteoblastic cells and influences osteogenesis.
Chemical pathway by which capacitive coupling acts on the bone cell to cause
proliferation and osteogenesis is signal transduction results from calcium ion
translocation through voltage-gated calcium channels that leads to
increases in prostaglandin
cytosolic calcium, and
activated calmodulin
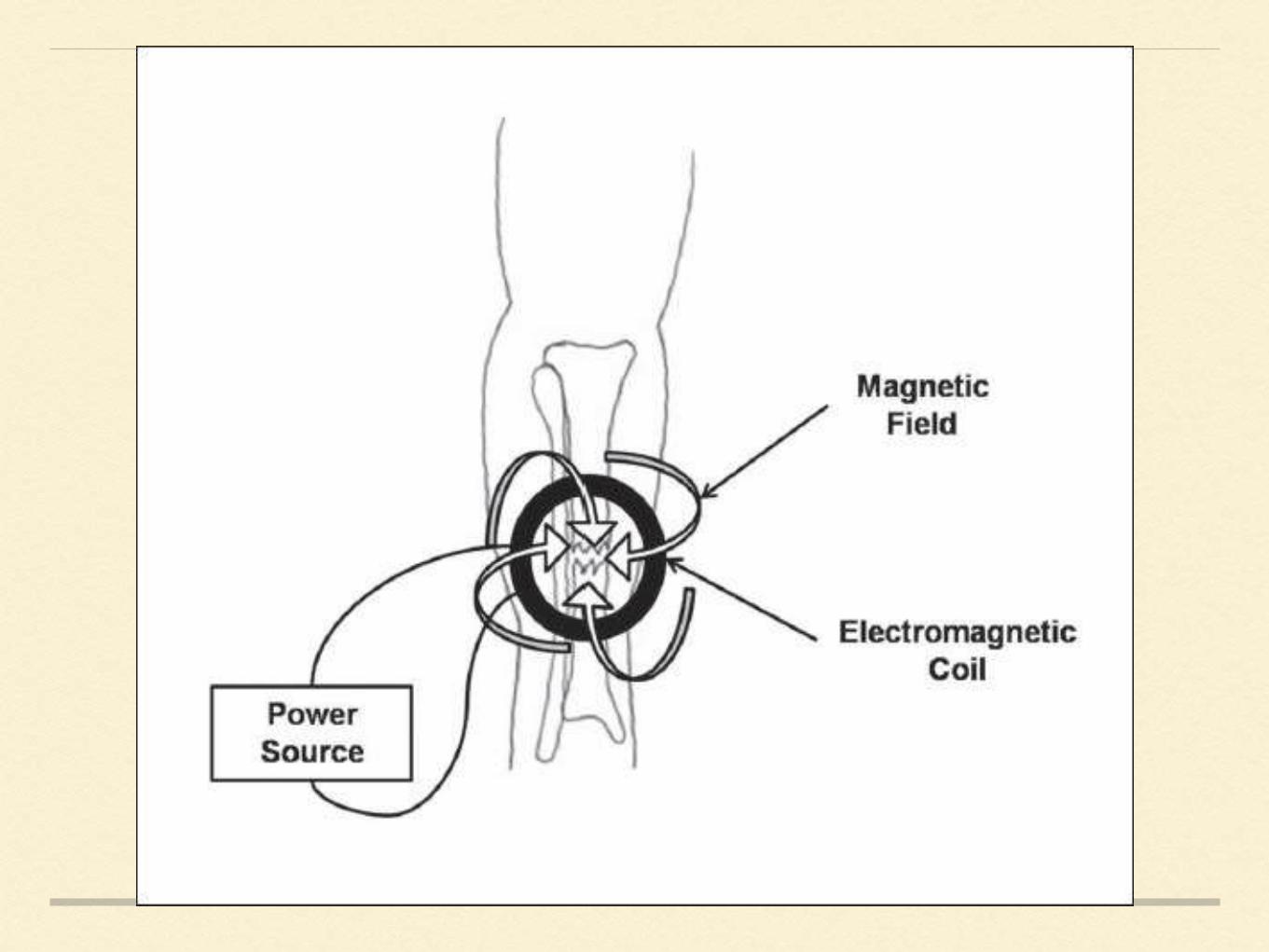
INDUCTIVE COUPLING
Inductive coupling relies on the use of a pulsed electromagnetic field
(PEMF) device that is placed on the skin over the fracture site .
The PEMF consists of a wire coil through which a current is passed and a
magnetic field is generated. The magnetic field, in turn, induces an electrical
field within the fracture site.
The size of the electrical field that is induced within the fracture site is
dependent on the magnitude of the magnetic field and the physical
characteristics of the tissues surrounding and within the fracture site.
Induced magnetic fields varying from 0.1 to 20G have been used to produce
electrical fields varying from 1 to 100 mV/cm within bone
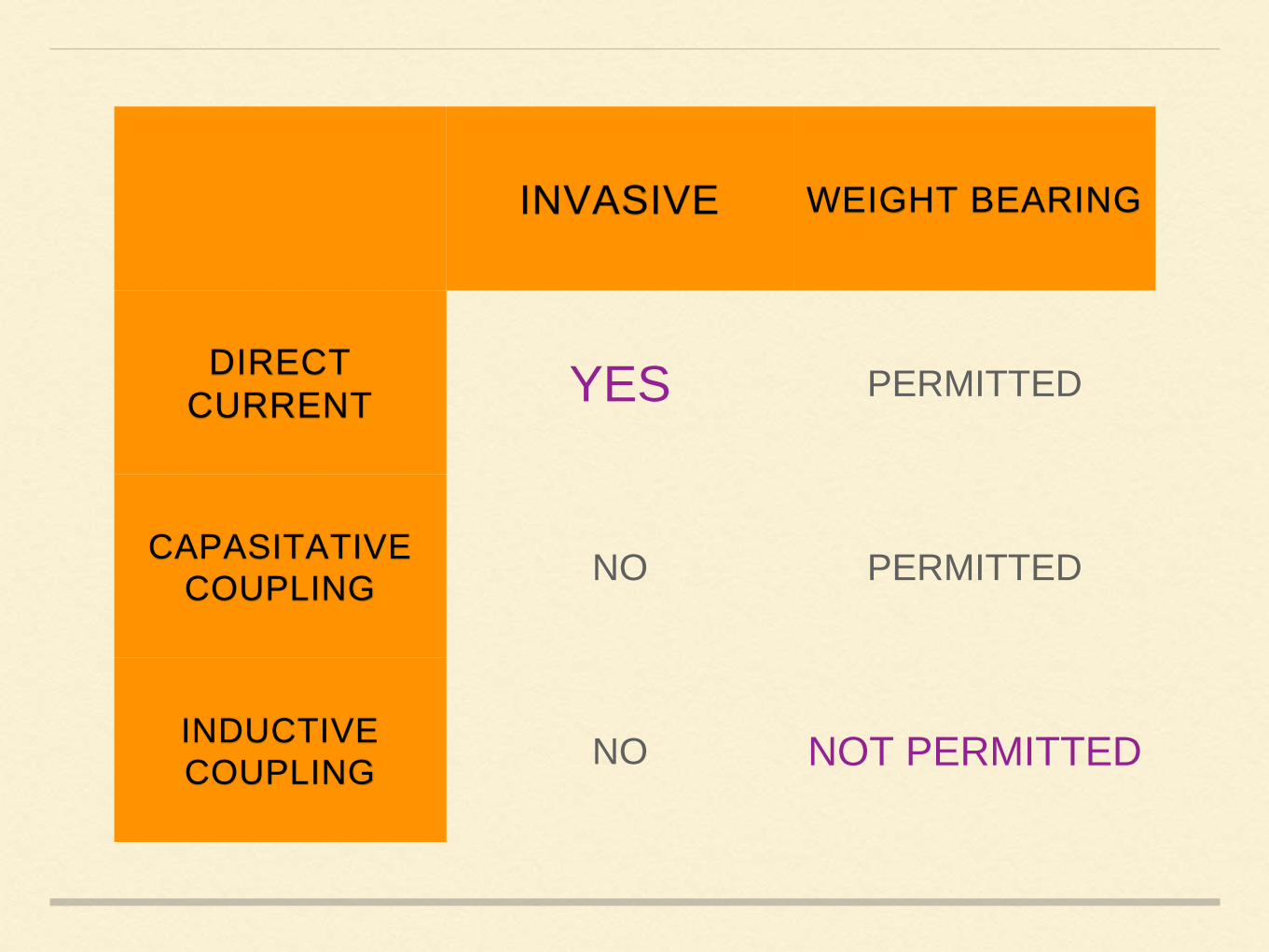
INVASIVE WEIGHT BEARING
DIRECT
CURRENT YES PERMITTED
CAPASITATIVE
COUPLINGNO PERMITTED
INDUCTIVE
COUPLINGNO NOT PERMITTED
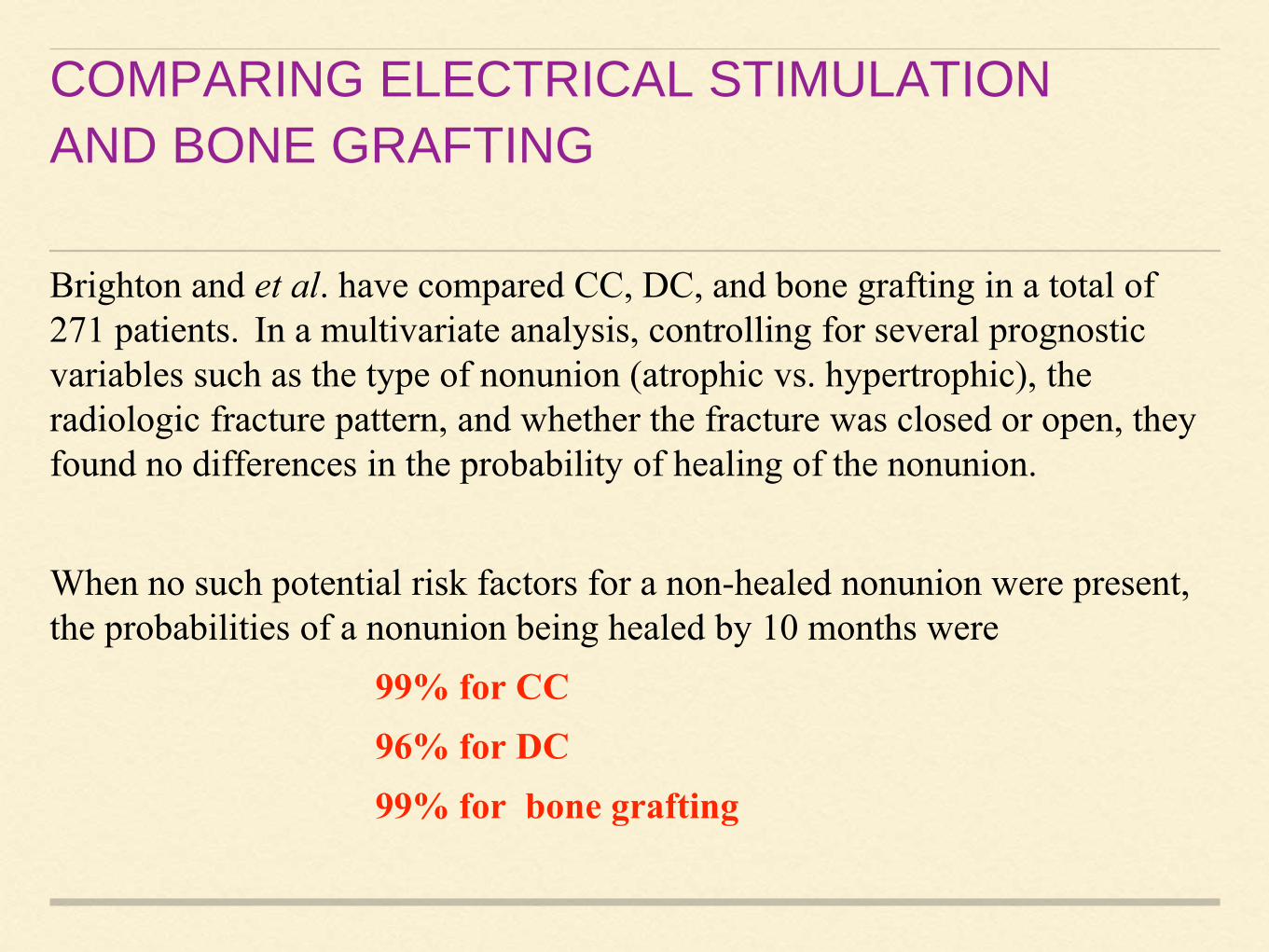
COMPARING ELECTRICAL STIMULATION
AND BONE GRAFTING
Brighton and et al. have compared CC, DC, and bone grafting in a total of
271 patients. In a multivariate analysis, controlling for several prognostic
variables such as the type of nonunion (atrophic vs. hypertrophic), the
radiologic fracture pattern, and whether the fracture was closed or open, they
found no differences in the probability of healing of the nonunion.
When no such potential risk factors for a non-healed nonunion were present,
the probabilities of a nonunion being healed by 10 months were
99% for CC
96% for DC
99% for bone grafting

PEMS promotes organization and consolidation in delayed union.
PEMF treatment of osteoblasts in the active proliferation stage accelerates
cellular proliferation, enhanced cellular differentiation, and increased bone
tissue-like formation.
PEMF has role in stimulating protein synthesis, which have effect in gene
regulation.Up-regulation of mRNA levels and protein synthesis for growth
factors has also been observed with the application of PEMS. This
enhances cellular repair and synthesis of extracellular proteins, which have
role in differentiation and growth.
Recent series of Simons et al.(2003) and Punt et al.(2008)
Daily duration of therapy 12 hrs / day schedule to be effective and compliant for
patients as well.
In their series, >90% success was achieved.
Infection has no detrimental effect on fracture healing but gap between fracture
ends and distance between coils are important factors.
Distance between coils has worked by producing coil effects across fracture
ends. They work by generation of electromagnetic field leading to stimulation of
osteosynthesis.
Best nonunion to be treated by this method is one without any other complication
such as infection.
Compound fractures in need of dressing with gap or loss of bony fragment will
be difficult to be managed by this modality.
CONTRAINDICATIONS
Segmental bone loss at the fracture site
Synovial pseudoarthrosis
Infected nonunions
Poor mechanical stability of the fracture site.
In these clinical scenarios, surgical management to bone graft defects,
eradicate infection, or stabilize the fracture with internal fixation is
required before electrical stimulation can be considered.
Electrical stimulation should be thought of as an adjunct to, not a
replacement for, standard fracture care.
Current evidence from randomized trials is insufficient to conclude a benefit
of electromagnetic stimulation in improving the rate of union in patients with a
fresh fracture, osteotomy, delayed union, or nonunion.
Current evidence is insufficient to conclude a benefit of electromagnetic
stimulation on time to healing in tibial stress fractures.
Current evidence is insufficient to attribute a reduction in pain to
electromagnetic stimulation in patients with a fracture or osteotomy;
Electromagnetic stimulation results in short but not long-term (i.e., four
weeks or more) increases in scintimetric healing activity with no impact on
fracture redisplacement rates in non operatively treated
Bone density is improved in patients undergoing femoral intertrochanteric
osteotomy
Monitoring Electric property of bone is useful for diagnosing
delayed and early non-union of bones and may enable the clinician
to change the line of treatment.
Electric properties like :
Impedence
Mutual Inductance
Resonant frequency
Conductance
• Patients with abnormal healing due to various complications impedance
at the time of fracture union was lower than that at the first week.
• The impedance showed significant difference at week 1, 4 and 6.
• Conductance can be a marker of fracture healing at week 8. There is no
significant difference between the values of conductance at week 4 and 6
• This suggests that inductance and conductance can be used for the early
diagnosis of delayed unions.
SCAPHOID FRACTUREAND
NONUNION
Treatment of scaphoid non-union presently includes ongoing
immobilization, bone grafting, various internal fixators, and combinations of
these. Ultimately it may become necessary to insert a prosthetic scaphoid.
The use of pulsing electromagnetic fields and capacitively coupled
electric fields, both of which methods claim a high rate of success.
One Study has suggested that the combined use of a bone graft plus
electrical stimulation has a higher rate of success than either method
alone.
Osterman et al, state in their review article of scaphoid non-union that
the most appropriate indication for the use of electrical stimulation is in
those patients who have failed the previous bone grafting and in
whom the scaphoid has remained relatively aligned.
Frykman and Adams on 44 and 54 scaphoid nonunions, respectively, showed
that 69%to 80% of un-united fractures that presented more than six months
after injury, healed using PEMF stimulation and a thumb spica cast.
Patients were treated for at least three months or until the fracture had united.
Nonunions with radiological evidence of avascular necrosis 73% to 89%
Acute scaphoid fractures by up to 30%.
The healing of tibial and radial fractures was found to be significantly
accelerated in two prospective, randomised, double-blind trials as an adjunct to
conventional treatment.
IMPACTED HIP FRACTURES
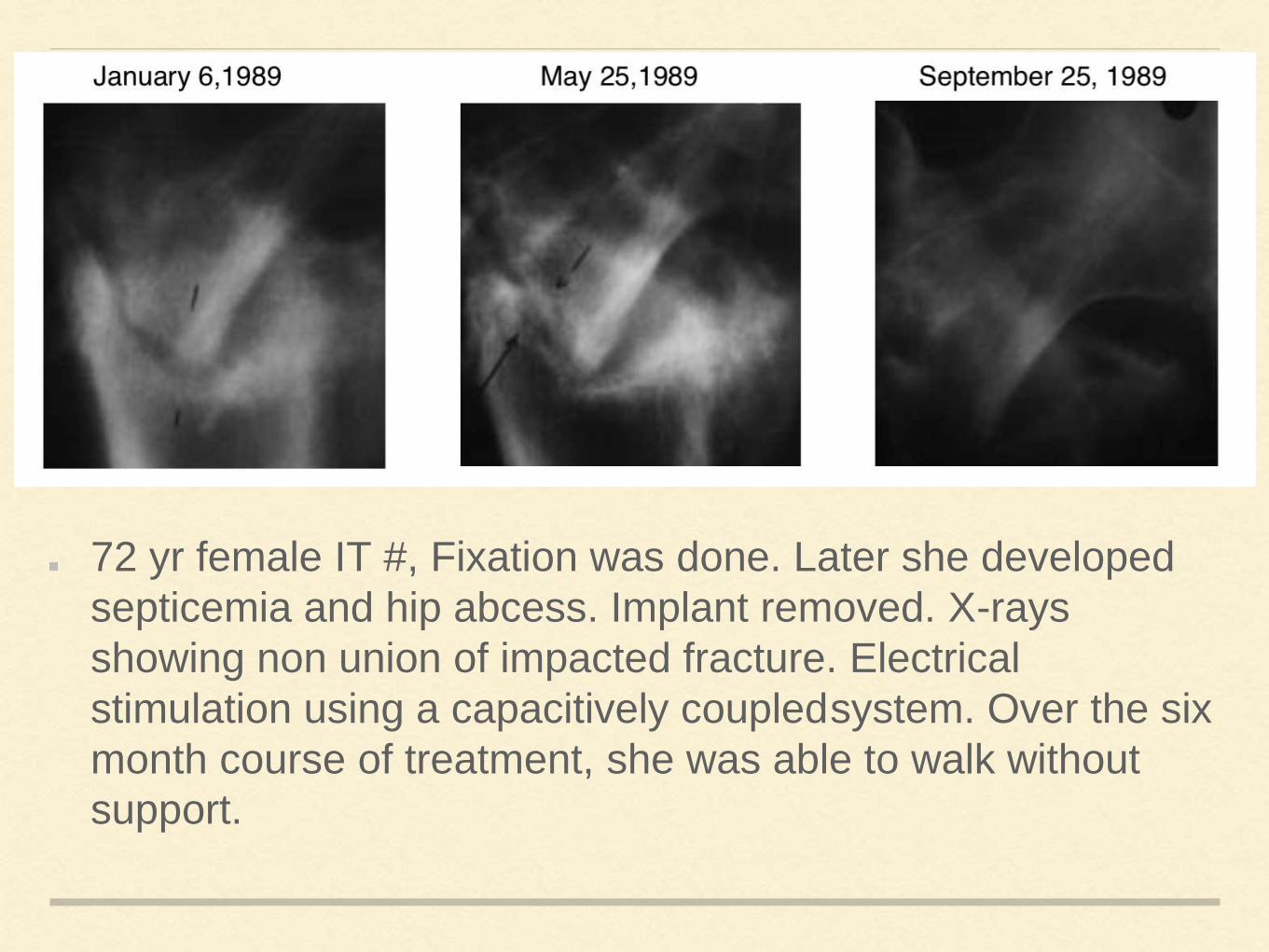
72 yr female IT #, Fixation was done. Later she developed
septicemia and hip abcess. Implant removed. X-rays
showing non union of impacted fracture. Electrical
stimulation using a capacitively coupledsystem. Over the six
month course of treatment, she was able to walk without
support.
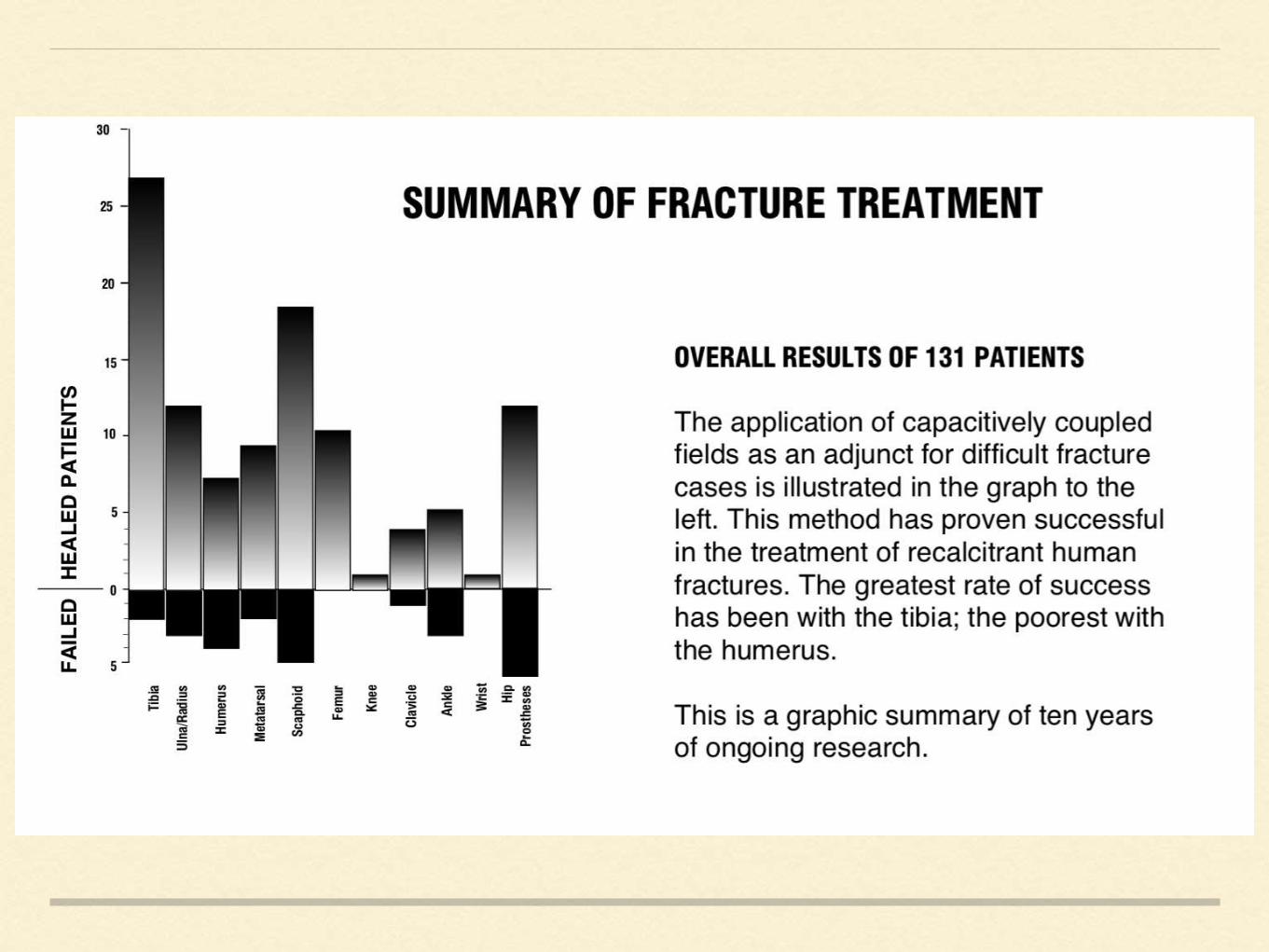
FRACTURE TREATMENT
PAINFUL HIP PROSTHESIS
In 1985 Ascherl reported clinical evidence of tightening in loosened hip
prostheses using pulsed electromagnetic fields. Using a clinical scoring
system, he reported a success rate of 69.5% in 348 loosened
arthroplasties.
In a similar study in 1988, Kennedy reported a 55% success rate
Brighton and Pollack demonstrated that capacitively coupled electrical fields
were as effective as inductively induced fields in the treatment of non-unions in
long bones in humans.
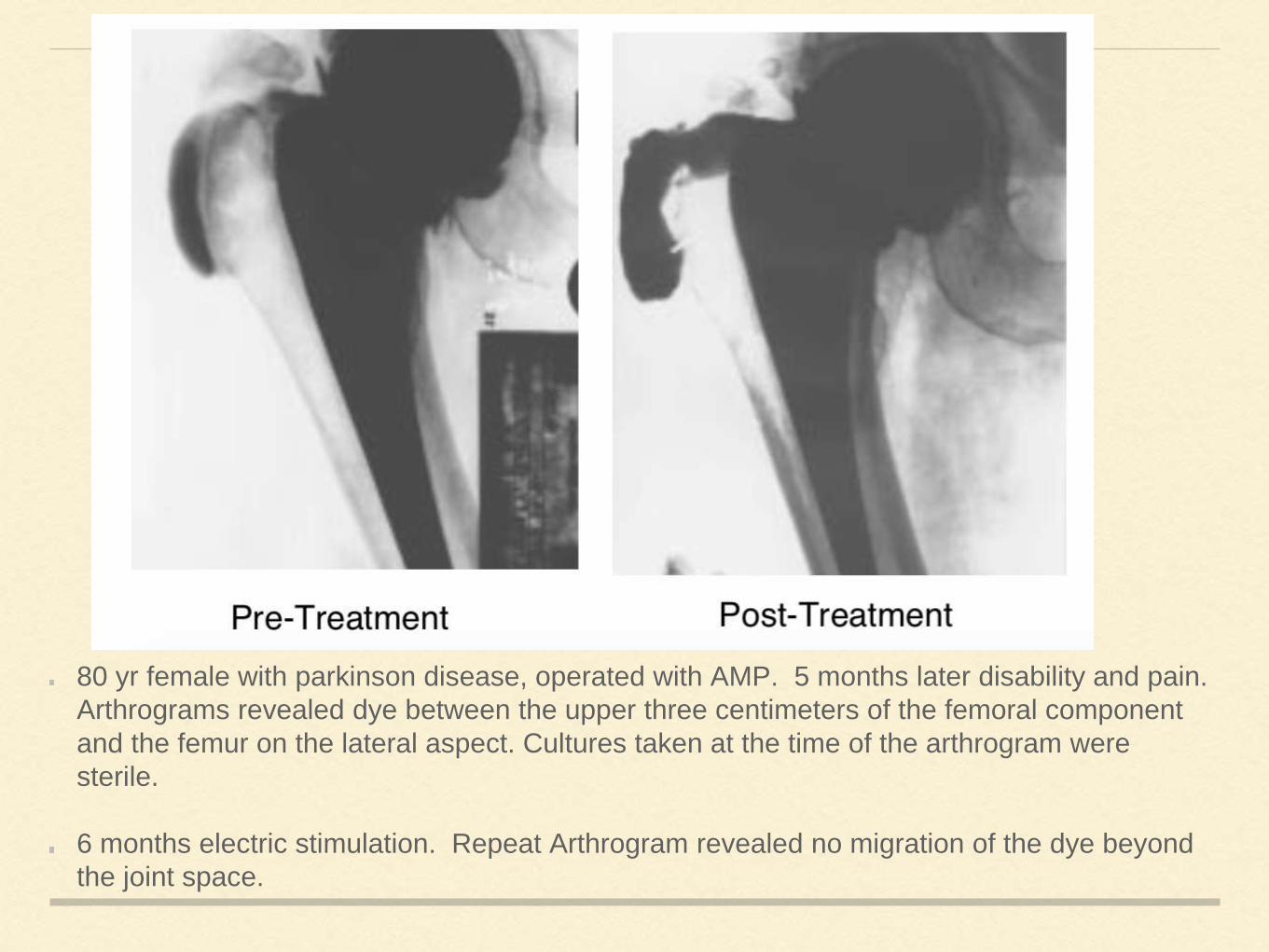
80 yr female with parkinson disease, operated with AMP. 5 months later disability and pain.
Arthrograms revealed dye between the upper three centimeters of the femoral component
and the femur on the lateral aspect. Cultures taken at the time of the arthrogram were
sterile.
6 months electric stimulation. Repeat Arthrogram revealed no migration of the dye beyond
the joint space.
Fifteen patients with painful hip prostheses were exposed to pulsed electric
fields for eight hours per day over a period of six to twelve months and
followed with a clinical scoring system for four years.
In twelve of the fifteen there was clinical improvement as measured by a
modified Harris Hip score.
Three of the twelve went on to revision surgery because of insufficient relief
of pain and the remaining nine avoided further surgery
Overall success rate of 60% at four years.
OSTEOPOROSIS
Use of pulsed electromagnetic fields, induced at a
physiological frequency and intensity, to prevent
osteoporosis.
Using treatment regimen of 1 hr per day of pulsed
electromagnetic fields, produced an osteogenic dose
response to induced electric power, with maximum
osteogenic effect between 0.01 to 0.04 tesla per sec.
Response showed decrease of intracortical remodeling,
inhibition of endosteal resorption and stimulation of both
endosteal and periosteal new bone formation.
OSTEOARTHRITIS

Positive results in terms of pain reduction and bone healing by the
application of pulsed electromagnetic fields to damaged or painful tissues
and osteoarthritic joints, regardless of method of stimulation.
Potential for favorable restorative transcriptional and biochemical effects of
applied fields on the cells of bone and cartilage and their surrounding tissue
structures.
1. In contrast to other physiotherapy modalities which may invoke
hyperthermia and proteolytic enzyme activity which increases cartilage
destruction, and potentially induces swelling, pulsed electromagnetic field
applications may be applied athermally
2. Application enhance chondrocyte activation in such a way so as to promote
proteoglycan and collagen synthesis.
3. Application could help with repair of bone damage, which may be causing or
perpetuating the disease to some extent.
4. Unlike drugs, pulsed electro-magnetic field effects may be prolonged, as well
as efficacious. Konrad et al (1996) , reported that the benefits of applying pulsed
electromagnetic field therapy for aseptic loosening of total hip prostheses were
still noticeable one year after completion of treatment
5. Unlike drugs, no side-effects of pulsed electromagnetic fields have been
reported in the literature.
6. Anti-inflammatory and pain reducing properties might prove equally valuable
in preserving joint integrity.
ARTHRODESIS
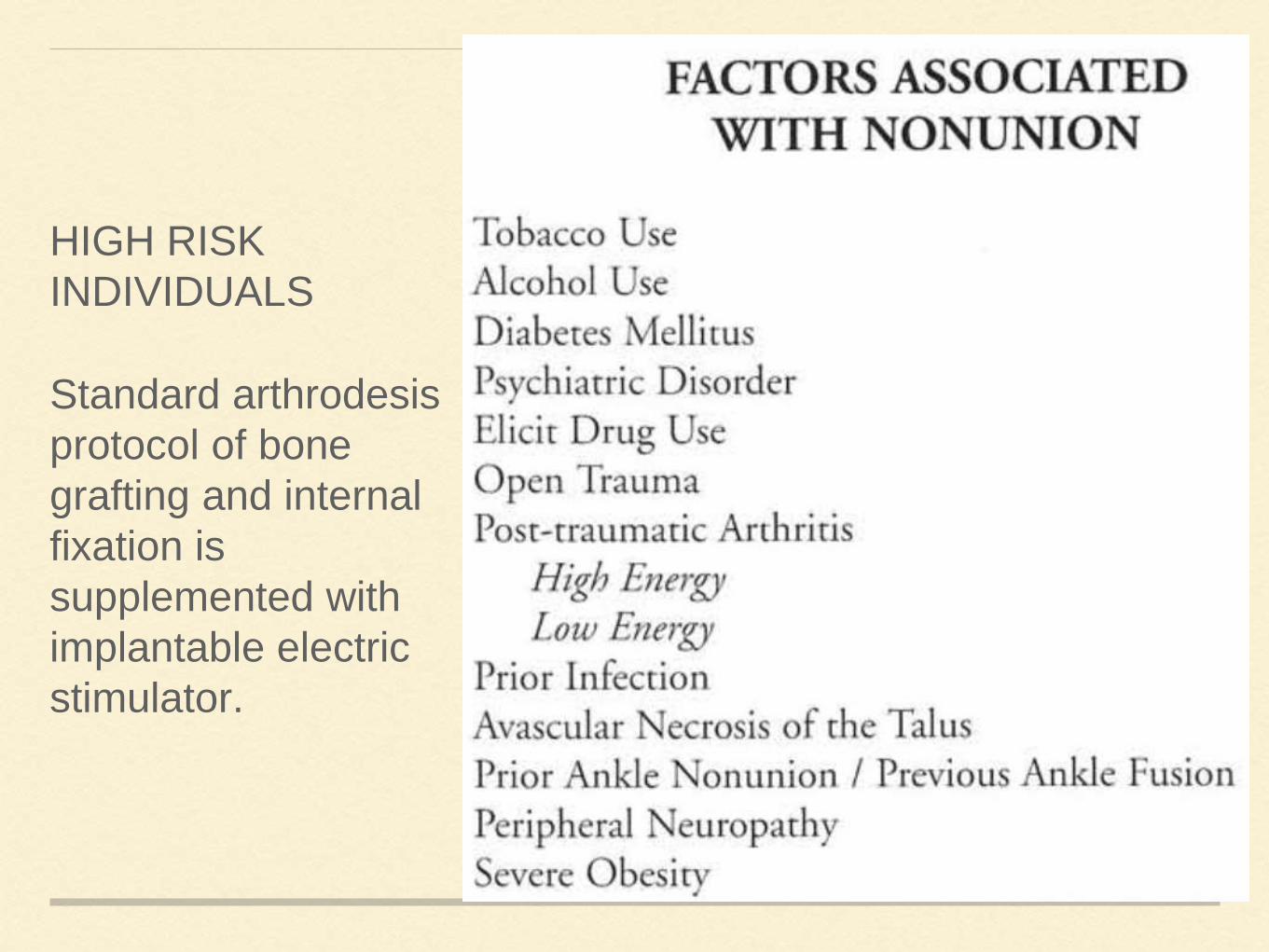
HIGH RISK
INDIVIDUALS
Standard arthrodesis
protocol of bone
grafting and internal
fixation is
supplemented with
implantable electric
stimulator.
SPINAL FUSION
Dwyer et al. were the first to show that adjunctive electrical stimulation
improved the fusion rate of a diagnostically varied group of patients
undergoing both anterior and posterior spinal fusion.
DEVISES :
Direct current
Capacitive coupling
Inductive coupling
Indicated in ‘Difficult to Fuse’ spine fusion population consisting of:
• One or more previous fusion attempts;
• Multi level procedures;
• Grade II or worse spondylolisthesis
• Risk factors, consisting of obese patients, smokers, diabetics
Randomized study compared 28 patients undergoing posterior spinal fusion
without stimulation and 31 patients with DCES. The stimulated group was
found to have a successful fusion rate of 81% compared with 54% in the
non-stimulated group.
Failure rates of lumbar fusion is about 20-40%.
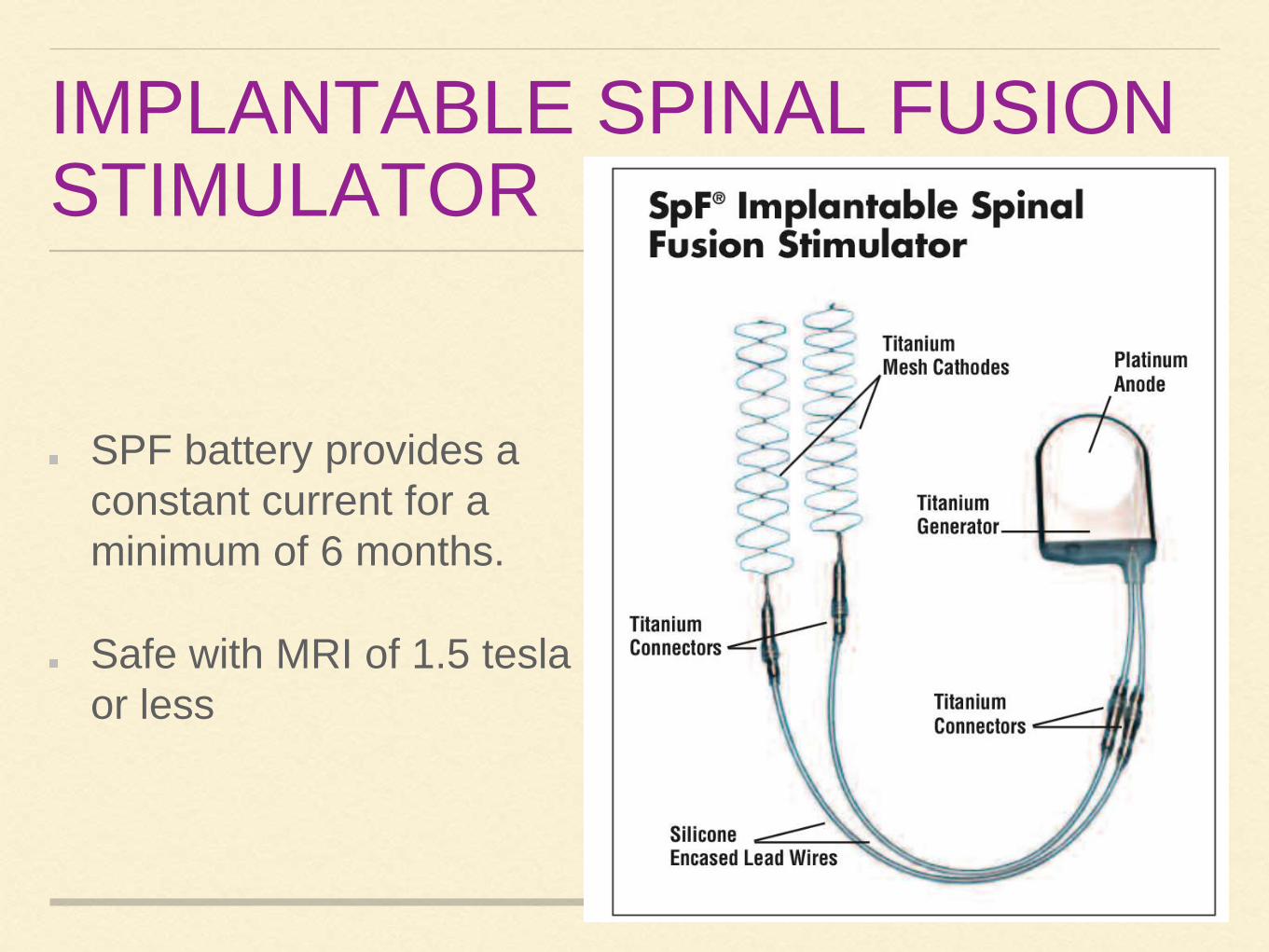
IMPLANTABLE SPINAL FUSION STIMULATOR
SPF battery provides a
constant current for a
minimum of 6 months.
Safe with MRI of 1.5 tesla
or less
AVASCULAR NECROSIS
Electrical stimulation has been shown experimentally to
enhance osteogenesis and neovascularization as well as to
alter osseus turnover.
Three different methods can be described:
1. Non-invasive pulsed electromagnetic-field stimulation
2. Direct-current stimulation of the necrotic area through
insertion of an electrode at the time of a core decompression
3. Non-invasive direct-current stimulation by capacitive
coupling after a core decompression

Stimulation with pulsed electromagnetic fields (PEMFs) has
been shown to be useful for enhancing bone repair and for
exerting a chondro protective effect on articular cartilage.
Electric stimulation was performed in combination with core
decompression (CD); although the results obtained were good, it
was not possible to demonstrate any statistically significant
advantage of the combined treatment as against treatment with
CD alone.
Results of the studies suggest that an early instrumental
diagnosis at the onset of the disorder and the immediate use of
PEMFs enables better clinical results.
Lesions in early stage respond well to treatment with PEMFs
and, in the majority of cases, as far as Ficat II, are capable of
preventing the progression of the disease.
Ficat stage -III does not constitute a real indication for this treatment.
Idiopathic lesions seem more sensitive to PEMF therapy as compared
with secondary forms, because the therapies responsible of the disease
cannot be interrupted.
Initial stages of the AVN are dominated by the ischemic and
inflammatory component; which is responsible for the joint pain, edema,
and degradation of the cartilage.
PMEF produces pain relief mediated by the anti inflammatory action of
the PEMFs that enables resolution of the joint edema.
Strong anti inflammatory effects of PEMFs causes an increase of adenylyl
cyclase activity and a reduction of superoxide anion production, as a result
of receptors located on the neutrophil surface.
This anti inflammatory action has been demonstrated on the sinoviocytes
and chondrocytes.The binding plays a fundamental role on the
inflammatory response and promotes new vessel formation and limits the
extension of the necrotic area, resulting from ischemia.
PEMFs exert a chondroprotective effect in vivo on osteoarthritis,which may
play a fundamental role in the treatment of early stages of osteonecrosis of
the femoral head by limiting the damage induced by inflammation and
preserving cartilage and subchondral bone exerting a short term effects.
PEMF has effects firstly on angiogenesis and then on osteogenesis.
In association with core decompression, biophysical stimulation enhances the osteo-
integration of autologous bone grafts, stimulates the local production of growth
factors, and favors the osteogenic activity of osteoblasts reducing the bone
reabsorption by interfering with the activation of the parathyroid hormone receptor,
thus decreasing the recruitment and differentiation of osteoclasts.
Stimulation with PEMFs may be a good opportunity to resolve the disease or at
least to delay the time until joint replacement becomes necessary.
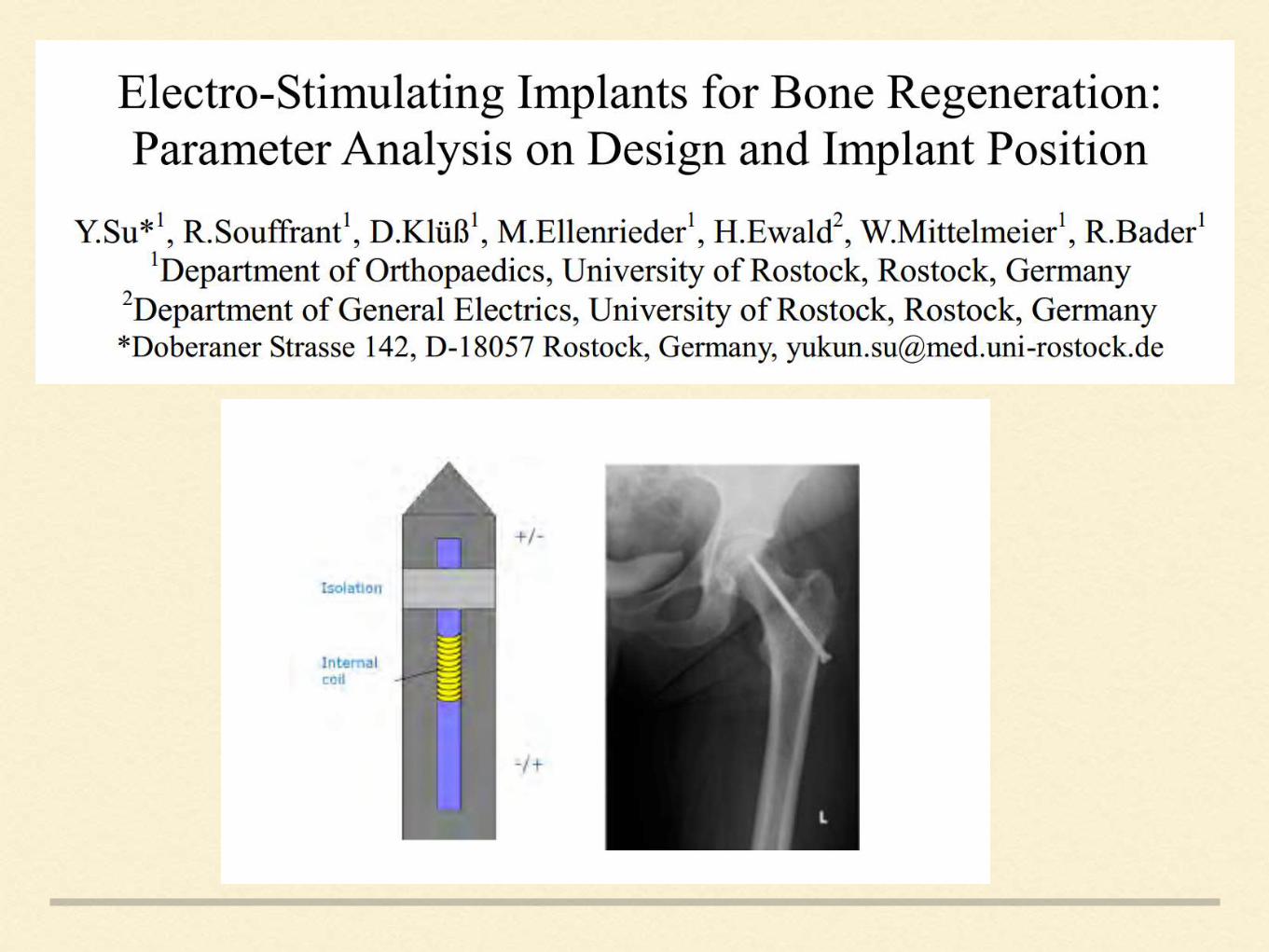
Alternating electromagnetic field using a screw implant to the
weak bone in the femoral head is to speed up bone regeneration
in case of avascular necrosis of the femoral head.
A BISS (bipolar induction screw system), as the depicted ASNIS
screw with integrated coil and electrodes is used.
ASNIS screw is only suitable for the case where the femoral
head show sclerosis and no collapse on cancellous bone . This
means, as long as the cartilage of the femoral head is not
damaged, the electro-stimulation therapy with the ASNIS-s
screw can be applied.
When the cartilage is ruptured and the femoral head shows
flattening, other therapies such as a total hip replacement have
to be considered.
GALVANIC CORROSION OR
BATTERY EFFECT
Some implant systems use several metals for different components. For example, Co-Cr rods may attach to titanium alloy screw heads, or Co-Cr rods and screw heads may attach to titanium alloy screw shanks.
This matching of dissimilar metals raises the concern of galvanic (bimetal) corrosion, also known as the battery effect.
An electrochemical effect occurs when two dissimilar metals, also known as a “couple,” are placed in an ionic bath.
An electric potential is created and ions flow from the anode metal, which is more resistant to corrosion and oxidation to the cathode metal.
Less resistant metal will undergo greater corrosion.
The strength of the effect is proportional to the difference in the electrochemical properties of the metals, called the “anodic index,” and can be measured by the electromotive force.
Galvanic corrosion can lead to
pain,
inflammatory responses,
metallosis, and
device failure.
For this reason, bimetallic systems designed to be used in corrosive environments should have an anodic index of 0.15 or less.
For galvanic corrosion to occur, the following three conditions must be met:
dissimilar metals,
electrical contact, and
a path for ion exchange.
All three conditions are present when medical devices are placed in the body.
Galvanic corrosion may be minimized by lessening the impact of
environmental factors through a process called Passivation. During this process, the surface of the implant is coated with a shielding layer, usually by formation of oxides, which will resist ion exchange.