Embed Size (px)
Citation preview
HEPATOPATHY IN CANINES: PROTOCOLS
FOR INVESTIGATION & MANAGEMENT
Pardeep SharmaAssistant Professor (Veterinary Medicine)
Department of Teaching Veterinary Clinical Complex
DGCN - College of Veterinary & Animal Sciences
CSK HPKV Palampur-176062
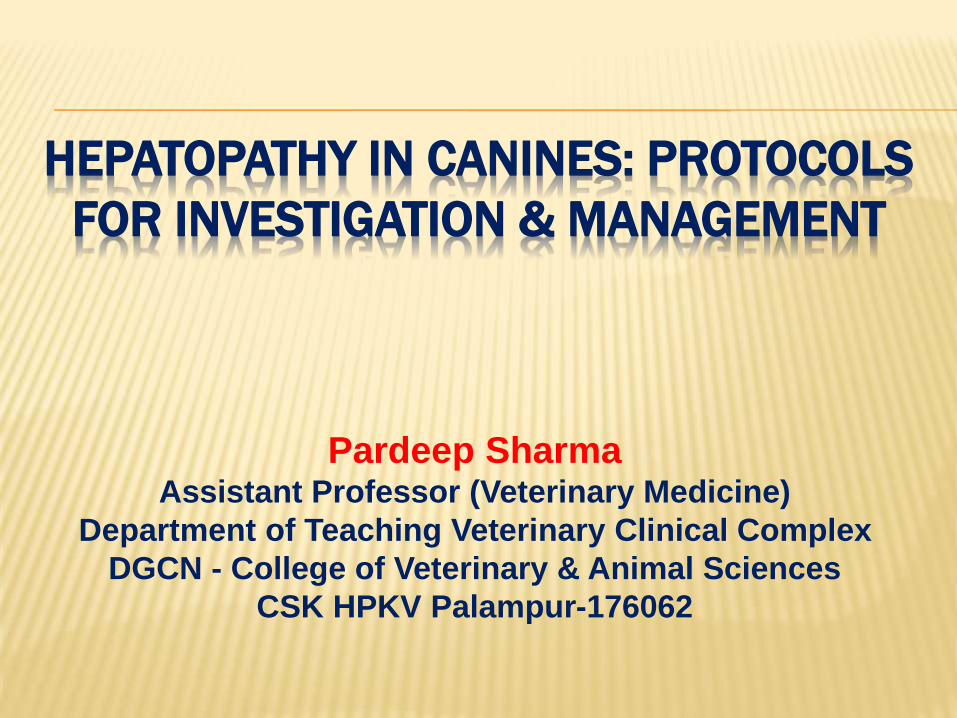
EXAMINATION OF LIVER
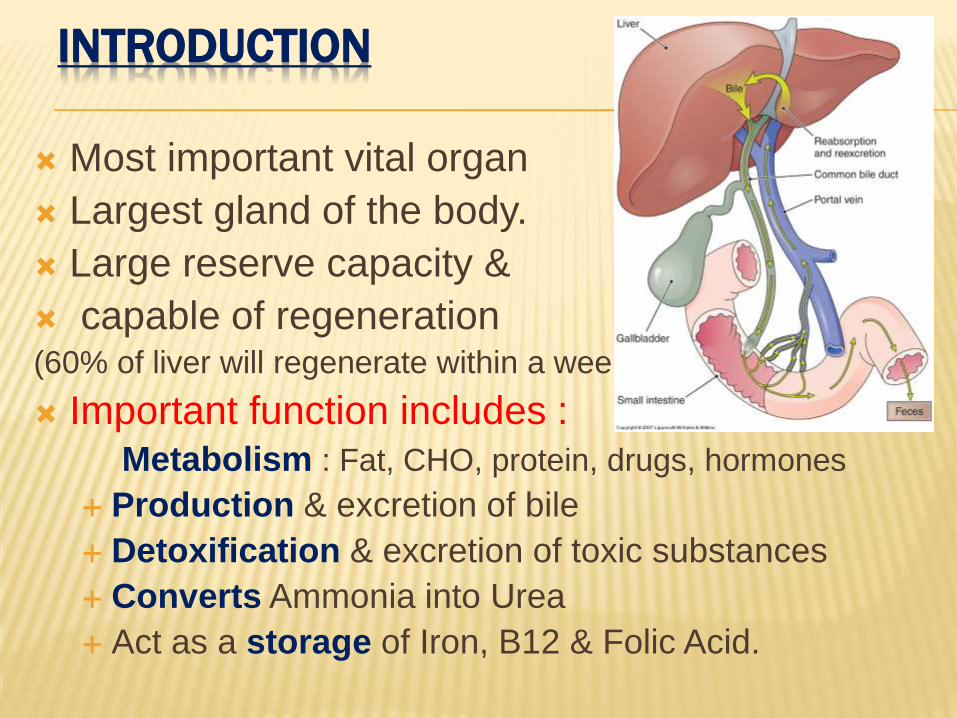
INTRODUCTION
Most important vital organ
Largest gland of the body.
Large reserve capacity &
capable of regeneration(60% of liver will regenerate within a week)
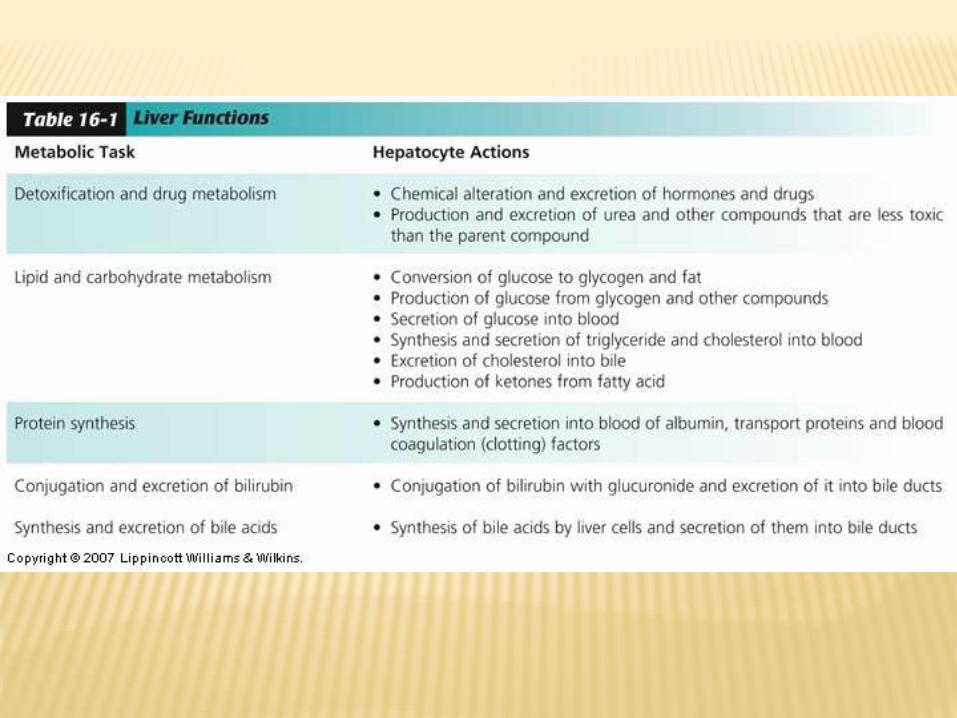
Important function includes :
Metabolism : Fat, CHO, protein, drugs, hormones
Production & excretion of bile
Detoxification & excretion of toxic substances
Converts Ammonia into Urea
Act as a storage of Iron, B12 & Folic Acid.
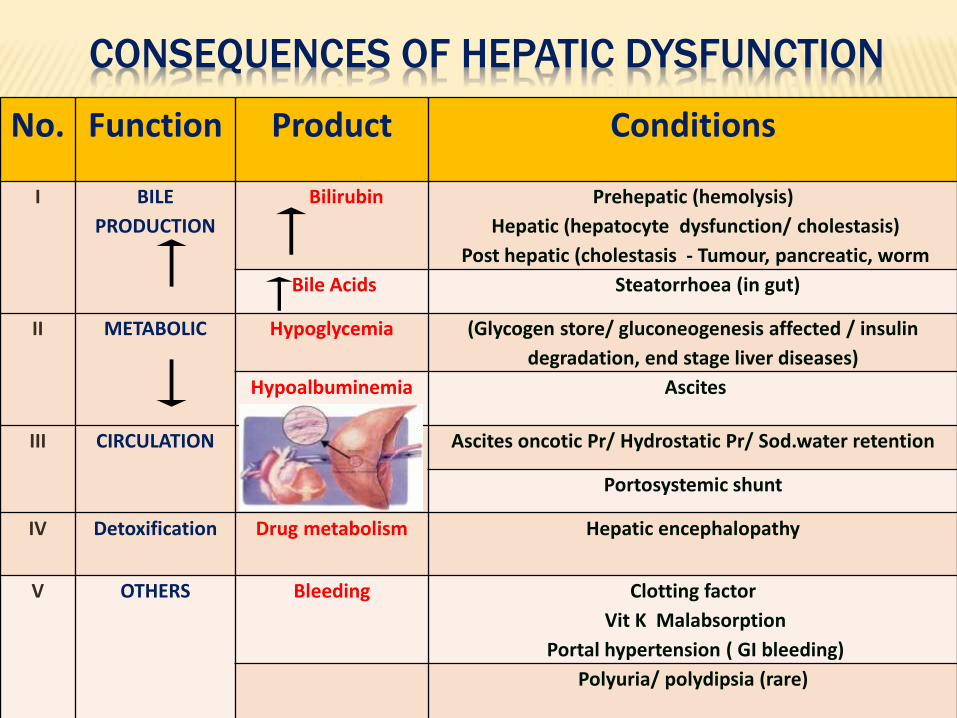
CONSEQUENCES OF HEPATIC DYSFUNCTION
No. Function Product Conditions
I BILE
PRODUCTION
Bilirubin Prehepatic (hemolysis)
Hepatic (hepatocyte dysfunction/ cholestasis)
Post hepatic (cholestasis - Tumour, pancreatic, worm
Bile Acids Steatorrhoea (in gut)
II METABOLIC Hypoglycemia (Glycogen store/ gluconeogenesis affected / insulin
degradation, end stage liver diseases)
Hypoalbuminemia Ascites
III CIRCULATION Ascites oncotic Pr/ Hydrostatic Pr/ Sod.water retention
Portosystemic shunt
IV Detoxification Drug metabolism Hepatic encephalopathy
V OTHERS Bleeding Clotting factor
Vit K Malabsorption
Portal hypertension ( GI bleeding)
Polyuria/ polydipsia (rare)
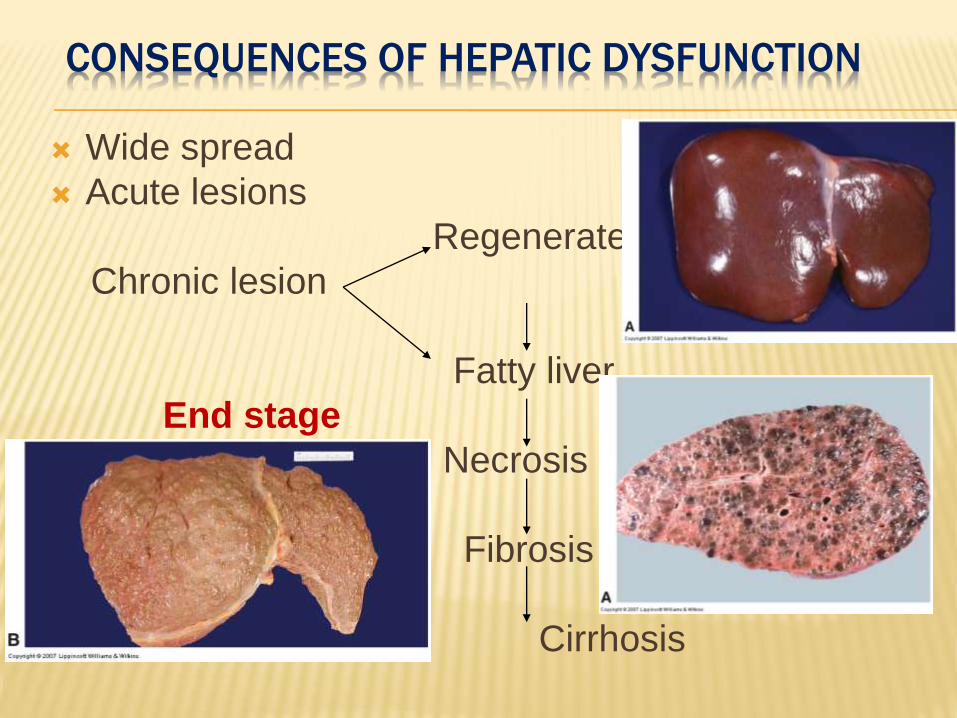
CONSEQUENCES OF HEPATIC DYSFUNCTION
Wide spread
Acute lesions
Regenerate
Chronic lesion
Fatty liver
End stage
Necrosis
Fibrosis
Cirrhosis
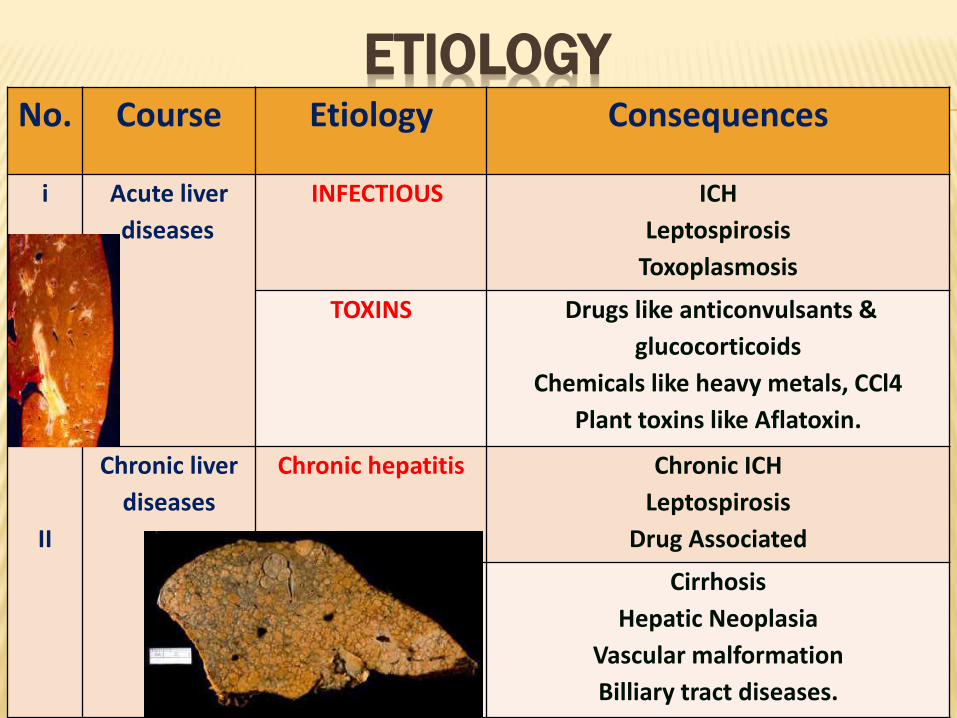
ETIOLOGYNo. Course Etiology Consequences
i Acute liver
diseases
INFECTIOUS ICH
Leptospirosis
Toxoplasmosis
TOXINS Drugs like anticonvulsants &
glucocorticoids
Chemicals like heavy metals, CCl4
Plant toxins like Aflatoxin.
II
Chronic liver
diseases
Chronic hepatitis Chronic ICH
Leptospirosis
Drug Associated
Cirrhosis
Hepatic Neoplasia
Vascular malformation
Billiary tract diseases.
BREED PREDISPOSITION
High incidences of inherited copper storage hepatopathy in the Belington terrier.
Middle aged dogs of a number of breeds are over represented including American and English Cocker spaniels.
West Highland White terriers,
Dobermans (strong female predisposition),
Dalmatians and Labrador retrievers

DIAGNOSIS OF LIVER DISEASE
History
Signalment
Clinical signs
Physical examination
Radiological examination
Ultrasonography
Haematological examination
Biopsy
Liver function tests
DIAGNOSIS
Challenge for clinician as :
Clinical signs are vague & non-
specific.
Even jaundice/ascites if present
requires differentiation from causes
other than liver diseases.
Lack of clinical signs are partly due to
large functional reserve of liver &
Remarkable power of regeneration.
About 80 % of liver’s functional
mass may be lost before clinical
signs develop.

Icteric Conjuctival
Mucosa
Ascites in Pomeranian
Physical
Examination
CLINICAL SIGNS :
Clinical signs suggestive of hepatopathy are : Lethargy, anorexia & selective feeding
Weight loss,
Polydypsia & polyuria
Vomition, diarrhoea, constipation
Jaundice & Ascites.
Certain clinical signs are more
related with liver diseases like:
Alteration in liver size : Enlargement / reduction.
Jaundice : Prehepatic / hepatocellular / obstructive.
Ascites.
Hepatic encephalopathy.
Faecal changes & coagulation defects.
Melaena
HEPATIC ENCEPHALOPATHY
Signs vary
• Depression,
• Behavioral
changes
•Mania
• Convulsions
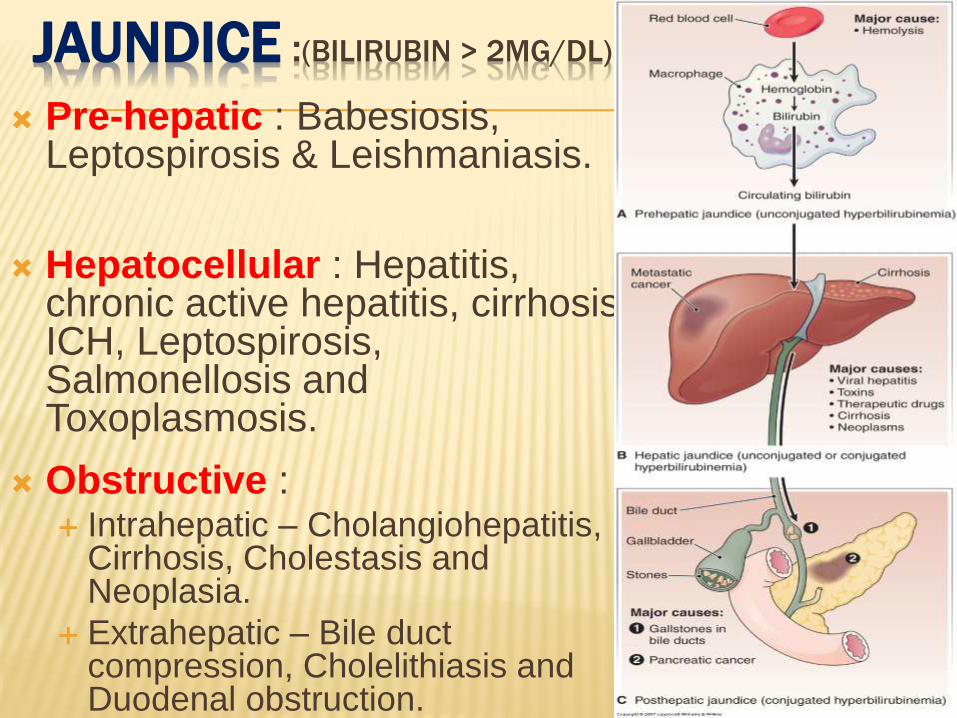
JAUNDICE :(BILIRUBIN > 2MG/DL)
Pre-hepatic : Babesiosis, Leptospirosis & Leishmaniasis.
Hepatocellular : Hepatitis, chronic active hepatitis, cirrhosis, ICH, Leptospirosis, Salmonellosis and Toxoplasmosis.
Obstructive : Intrahepatic – Cholangiohepatitis,
Cirrhosis, Cholestasis and Neoplasia.
Extrahepatic – Bile duct compression, Cholelithiasis and Duodenal obstruction.
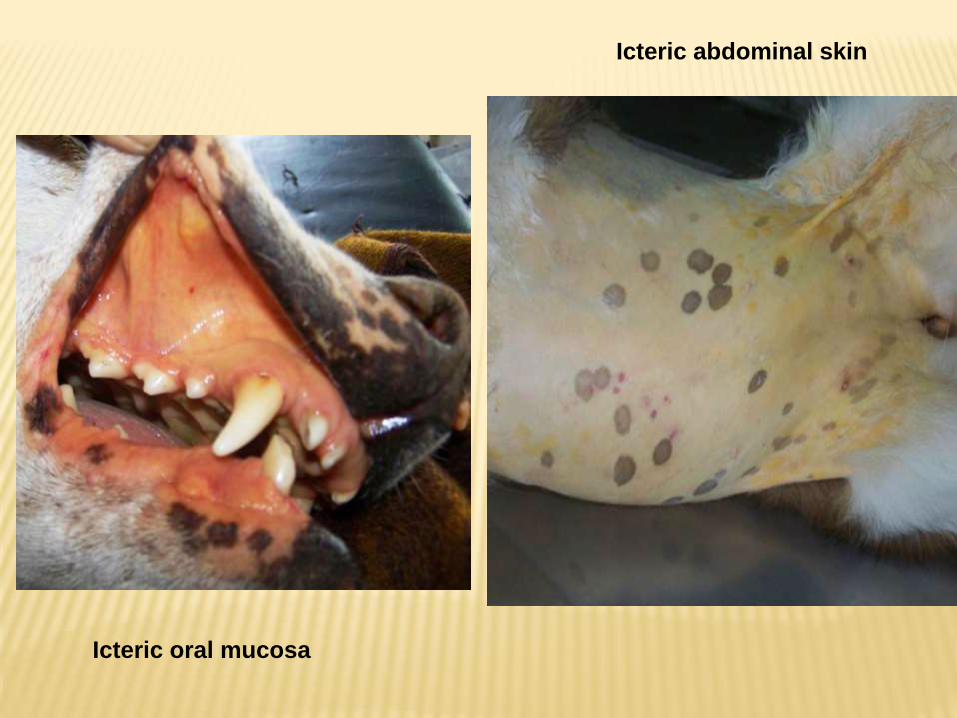
Icteric oral mucosa
Icteric abdominal skin
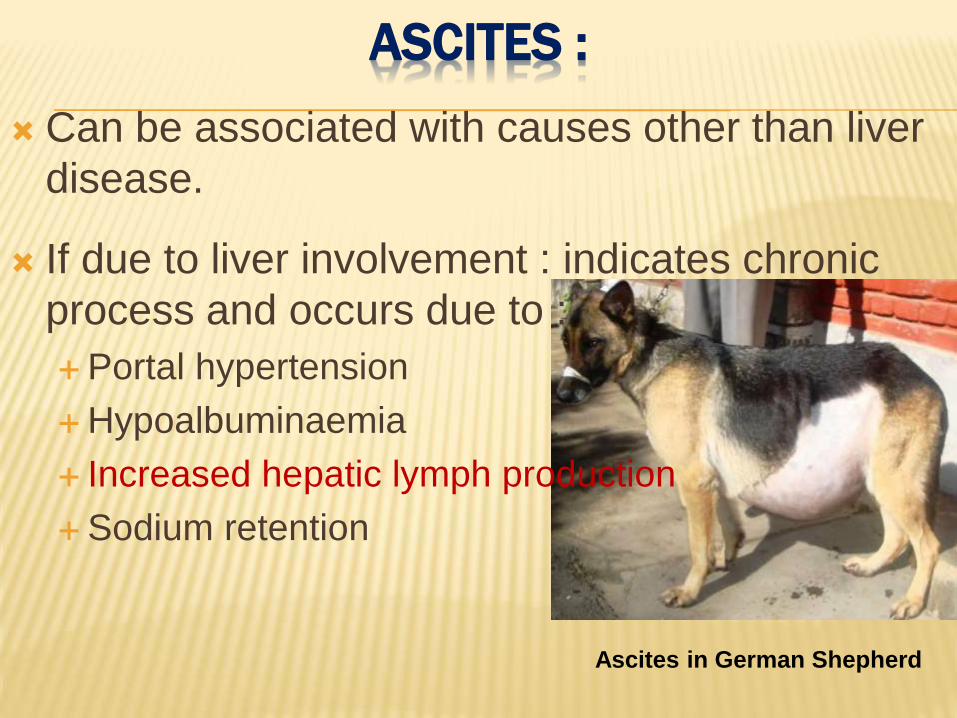
ASCITES :
Can be associated with causes other than liver
disease.
If due to liver involvement : indicates chronic
process and occurs due to :
Portal hypertension
Hypoalbuminaemia
Increased hepatic lymph production
Sodium retention
Ascites in German Shepherd
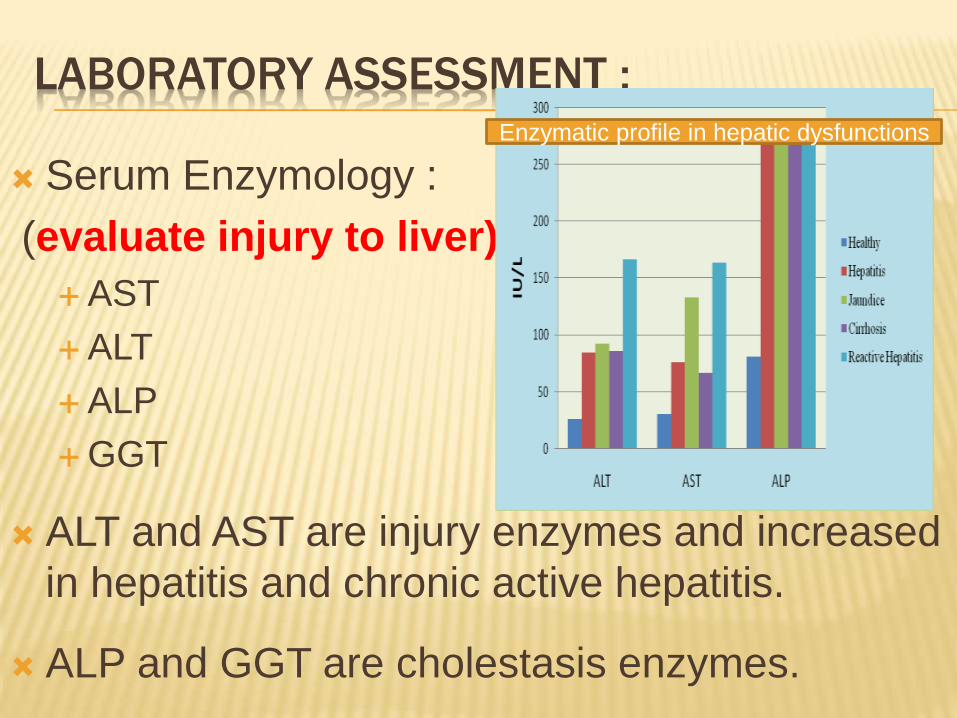
LABORATORY ASSESSMENT :
Serum Enzymology :
(evaluate injury to liver)
AST
ALT
ALP
GGT
ALT and AST are injury enzymes and increased
in hepatitis and chronic active hepatitis.
ALP and GGT are cholestasis enzymes.
Enzymatic profile in hepatic dysfunctions
TEST BASED UPON HEPATIC SECRETION /
EXCRETION: EVALUATE FUNCTION
Bile pigments
Bile salts (concentration is increased)
Clearance of foreign dyes (BSP: t ½ is increased in hepatopathy.)
TEST BASED UPON Specific biochemical function:
Plasma Albumin : Hypoalbuminaemia occuring in chronic liver diseases.
Globulin may increase or decrease depending upon chronicity.
Ammonia metabolism : Increased ammonia level lead to hepatic
encephalopathy.
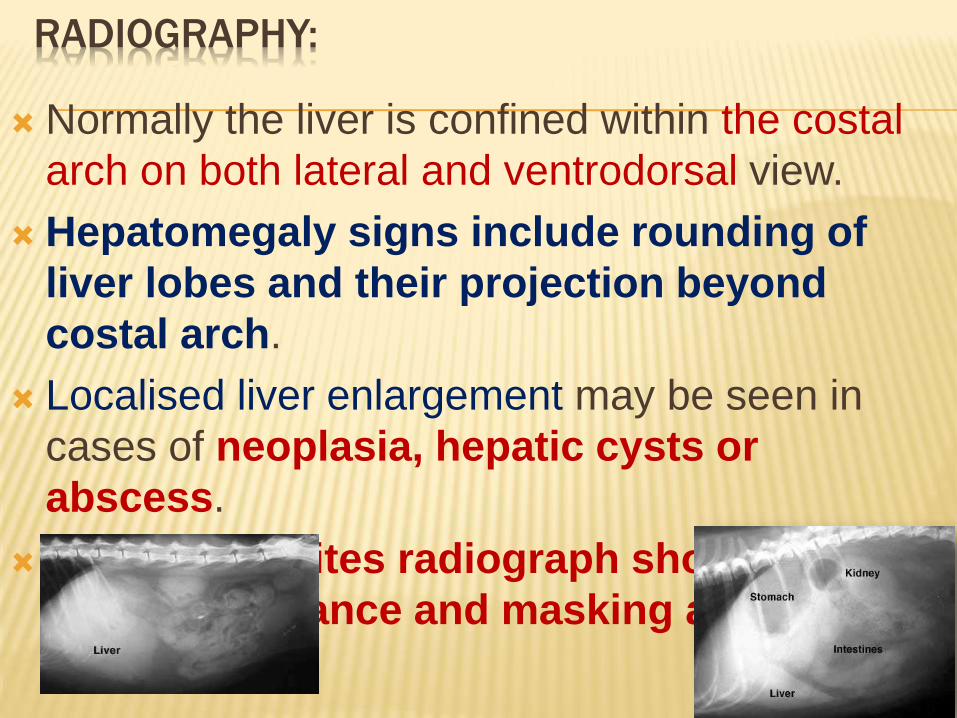
RADIOGRAPHY:
Normally the liver is confined within the costal
arch on both lateral and ventrodorsal view.
Hepatomegaly signs include rounding of
liver lobes and their projection beyond
costal arch.
Localised liver enlargement may be seen in
cases of neoplasia, hepatic cysts or
abscess.
In case of ascites radiograph shows ground
glass appearance and masking abdominal
details.
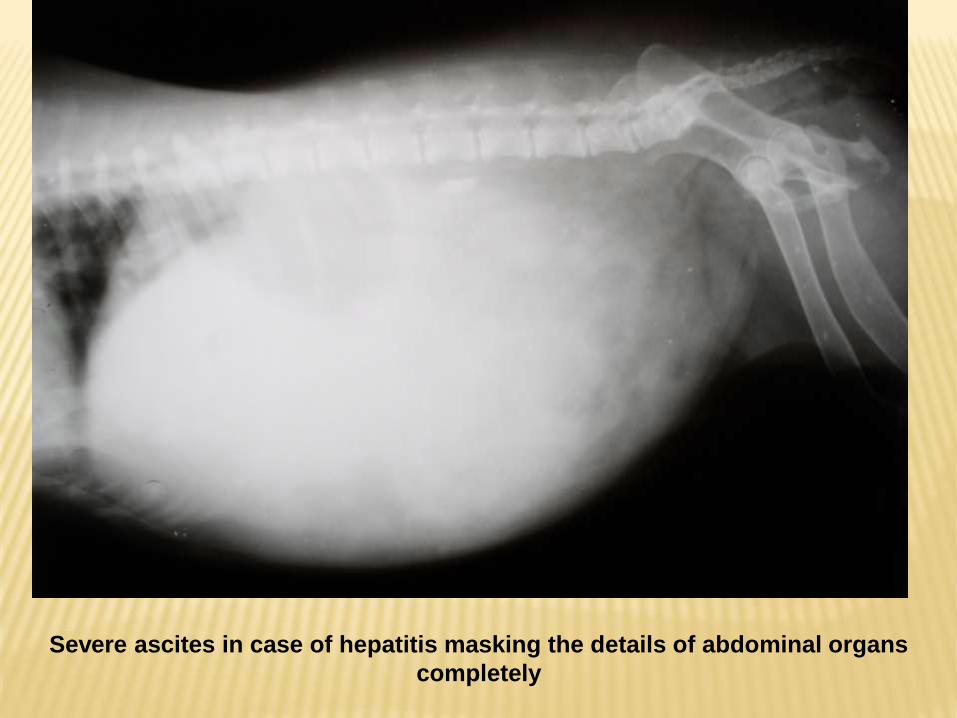
Severe ascites in case of hepatitis masking the details of abdominal organs
completely
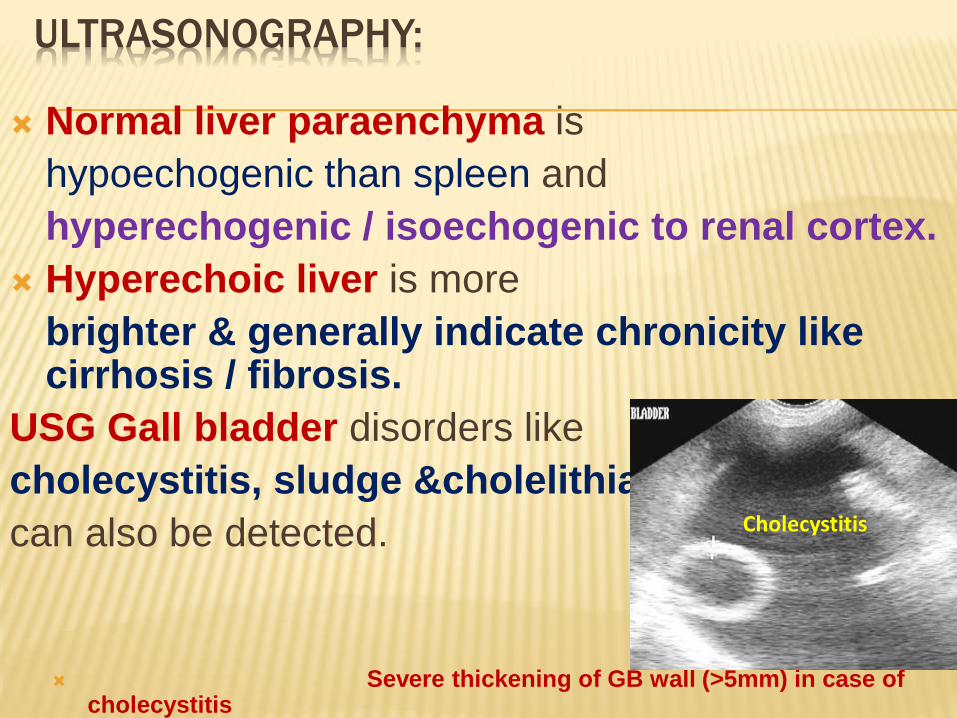
ULTRASONOGRAPHY:
Normal liver paraenchyma is
hypoechogenic than spleen and
hyperechogenic / isoechogenic to renal cortex.
Hyperechoic liver is more
brighter & generally indicate chronicity like cirrhosis / fibrosis.
USG Gall bladder disorders like
cholecystitis, sludge &cholelithiasis
can also be detected.
Severe thickening of GB wall (>5mm) in case of cholecystitis
Cholecystitis
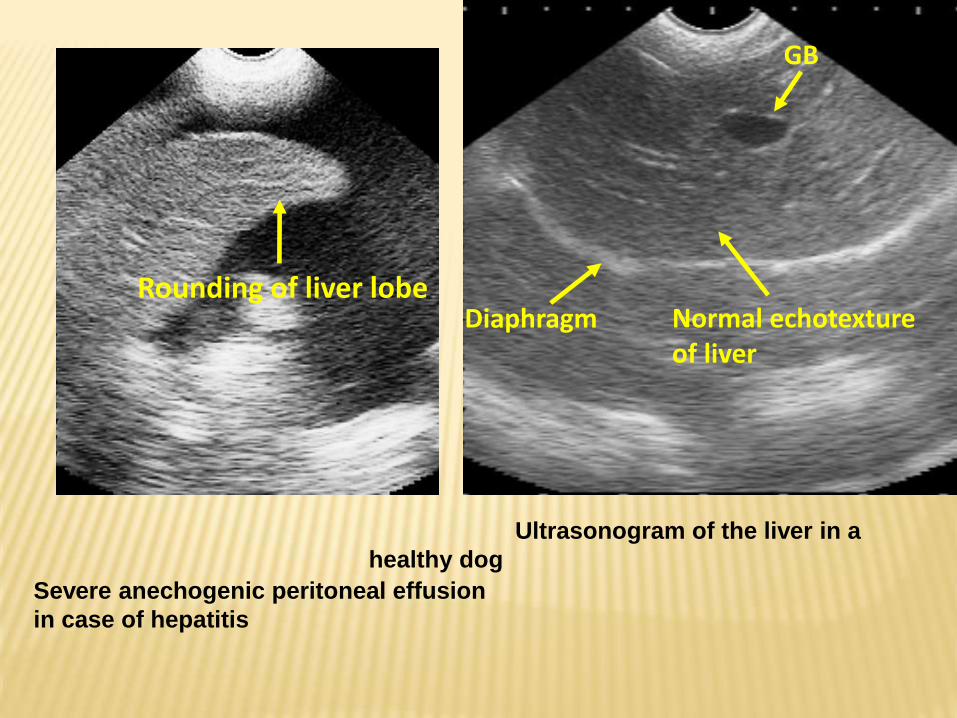
Diaphragm
GB
Normal echotexture of liver
Ultrasonogram of the liver in a
healthy dog
Rounding of liver lobe
Severe anechogenic peritoneal effusion
in case of hepatitis
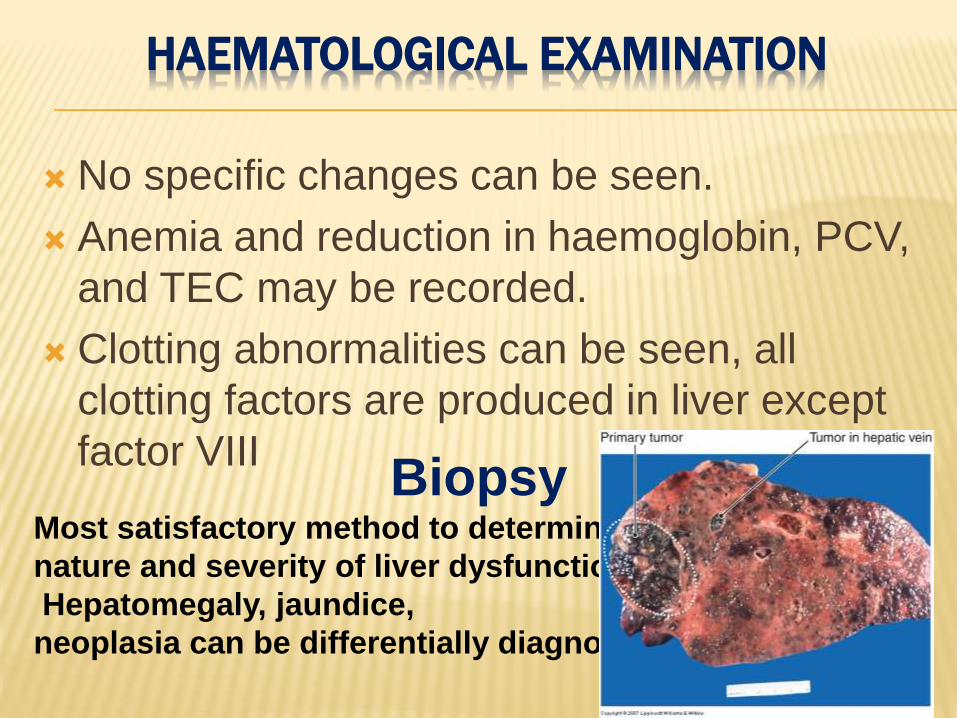
HAEMATOLOGICAL EXAMINATION
No specific changes can be seen.
Anemia and reduction in haemoglobin, PCV,
and TEC may be recorded.
Clotting abnormalities can be seen, all
clotting factors are produced in liver except
factor VIIIBiopsy
Most satisfactory method to determine
nature and severity of liver dysfunction.
Hepatomegaly, jaundice,
neoplasia can be differentially diagnosed.
DIETARY MANAGEMENT OF LIVER DISEASE
Rest to the animal.
Correct malnutrition by fulfilling the basic
energy.
Provide carbohydrate rich diet & nutrient
requirements (amino acids, K & Zn, especially
vitamins B, C & K).
Administration of 5-10 % glucose I/V.
Support hepatocellular regeneration by
providing the limiting nutrients i.e. diet must be
low in protein.
High biological value protein like Proteinex
should be given.
To limit liver damage by preventing copper
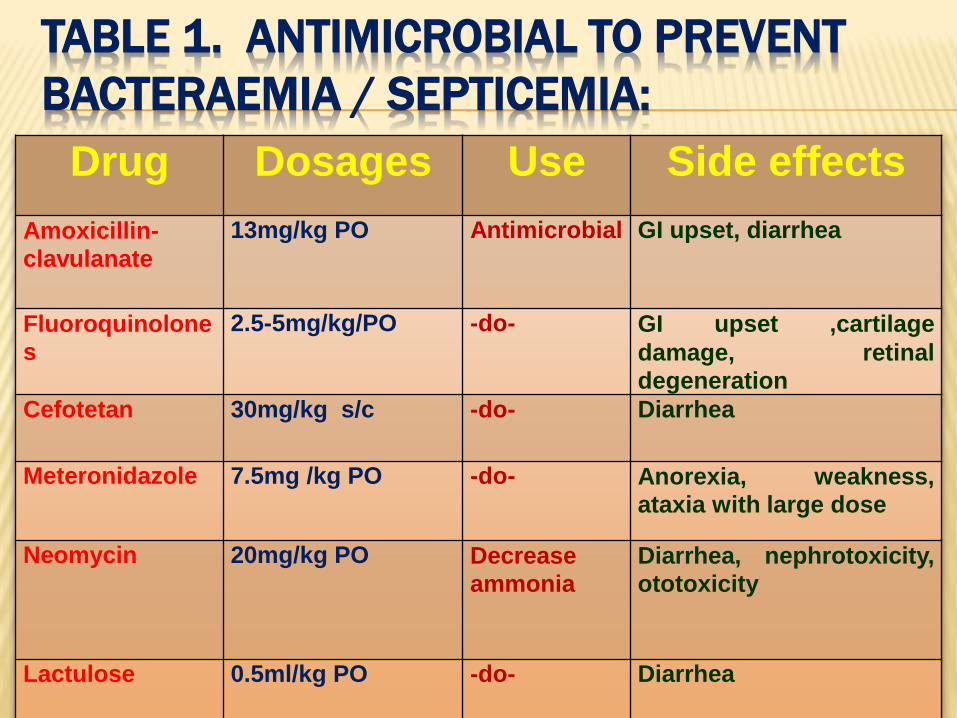
TABLE 1. ANTIMICROBIAL TO PREVENT
BACTERAEMIA / SEPTICEMIA:
Drug Dosages Use Side effects
Amoxicillin-
clavulanate
13mg/kg PO Antimicrobial GI upset, diarrhea
Fluoroquinolone
s
2.5-5mg/kg/PO -do- GI upset ,cartilage
damage, retinal
degeneration
Cefotetan 30mg/kg s/c -do- Diarrhea
Meteronidazole 7.5mg /kg PO -do- Anorexia, weakness,
ataxia with large dose
Neomycin 20mg/kg PO Decrease
ammonia
Diarrhea, nephrotoxicity,
ototoxicity
Lactulose 0.5ml/kg PO -do- Diarrhea
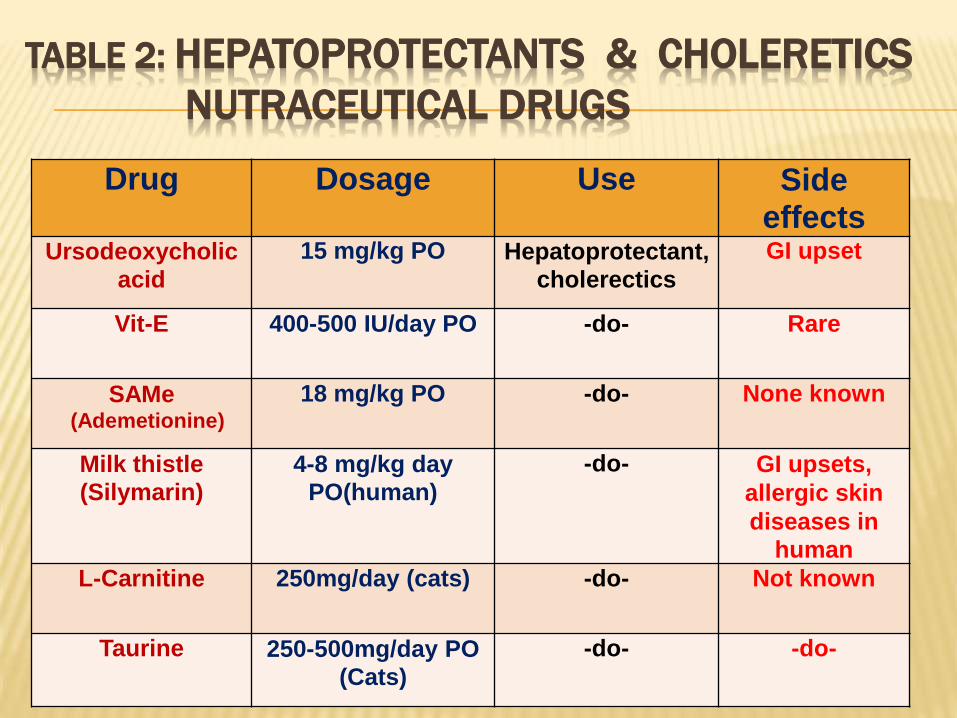
TABLE 2: HEPATOPROTECTANTS & CHOLERETICS
NUTRACEUTICAL DRUGS
Drug Dosage Use Side effects
Ursodeoxycholic
acid
15 mg/kg PO Hepatoprotectant,
cholerectics
GI upset
Vit-E 400-500 IU/day PO -do- Rare
SAMe(Ademetionine)
18 mg/kg PO -do- None known
Milk thistle
(Silymarin)
4-8 mg/kg day
PO(human)
-do- GI upsets,
allergic skin
diseases in
human
L-Carnitine 250mg/day (cats) -do- Not known
Taurine 250-500mg/day PO
(Cats)
-do- -do-
MANAGEMENT (CONTD…) :
Management of Ascites :
Include rest, dietary restriction of sodium.
Administration of diuretic.
Spironolactone @ 2 mg / kg b. wt. or combination of
spironolactone and frusemide is used.
Abdominal paracentesis in cases of respiratory
distress. (tapping the abdomen utilizing a
drainage technique)
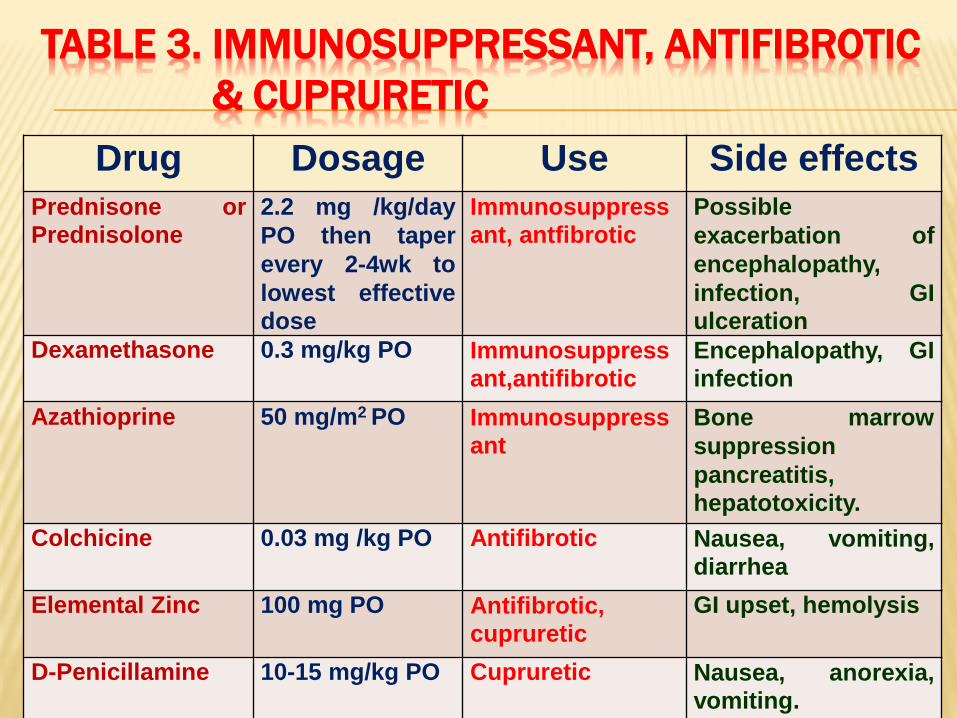
TABLE 3. IMMUNOSUPPRESSANT, ANTIFIBROTIC
& CUPRURETIC
Drug Dosage Use Side effects
Prednisone or
Prednisolone2.2 mg /kg/day
PO then taper
every 2-4wk to
lowest effective
dose
Immunosuppress
ant, antfibroticPossible
exacerbation of
encephalopathy,
infection, GI
ulceration
Dexamethasone 0.3 mg/kg PO Immunosuppress
ant,antifibroticEncephalopathy, GI
infection
Azathioprine 50 mg/m2 PO Immunosuppress
ant
Bone marrow
suppression
pancreatitis,
hepatotoxicity.
Colchicine 0.03 mg /kg PO Antifibrotic Nausea, vomiting,
diarrhea
Elemental Zinc 100 mg PO Antifibrotic,
cupruretic
GI upset, hemolysis
D-Penicillamine 10-15 mg/kg PO Cupruretic Nausea, anorexia,
vomiting.
TAKE HOME MESSAGE
Specific attention in high risk breeds
Non specific clinical signs
Increased ALT – initiate diagnostic steps
Rule out extra hepatic causes
Avoid / reduce hepato toxic drugs
THANKYOU
Don’t get angry
Smooth and easy gets
it every time