Embed Size (px)
DESCRIPTION
Citation preview

Diagnosis and Diagnosis and Management of Management of
Thombocytopenic Thombocytopenic DisordersDisorders
Dr Hamid HassanDr Hamid HassanRegistrarRegistrar
Dept. of GastroenterologyDept. of GastroenterologyCMCHCMCH

OverviewOverview
• Normal PhysiologyNormal Physiology• Categories of Categories of
ThrombocytopeniasThrombocytopenias• ITPITP• TTPTTP• HITHIT• DICDIC• HUSHUS

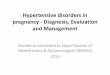
Early Haemostatic response & coagulation
Role of platelet

Pre-injury conditions encourage flow. The vascular endothelium produces
substances (including nitric oxide, prostacyclin and heparans) to prevent adhesion of platelets and white cells to the vessel wall. Platelets and coagulation factors circulate in a non-activated
state

• At the site of injury the endothelium is breached, exposing subendothelial collagen. Small amounts of tissue factor (TF) are released. Platelets bind to collagen via a specific receptor, glycoprotein Ia (GPIa), causing a change in platelet shape and its adhesion to the area of damage by the binding of other receptors (GPIb and GPIIb/IIIa) to von Willebrand factor and fibrinogen respectively. Coagulation is activated by the tissue factor (extrinsic) pathway, generating small amounts of thrombin

Normal Physiology-Normal Physiology-Production and NumberProduction and Number
• Platelets are normally made in the Platelets are normally made in the bone marrow from progenitor cells bone marrow from progenitor cells known as known as megakaryocytesmegakaryocytes..
• Normal platelet lifespan is 10d. Normal platelet lifespan is 10d. Every day, 1/10 of platelet pool is Every day, 1/10 of platelet pool is replenished.replenished.
• Normal platelet count is between Normal platelet count is between 150,000 and 450,000/mm150,000 and 450,000/mm33

Thrombocytopenia-Thrombocytopenia-How low is too low?How low is too low?
• 150,000 - 50,000: no symptoms150,000 - 50,000: no symptoms– No treatment generally required.No treatment generally required.
• 50,000 - 20,000: first symptoms50,000 - 20,000: first symptoms– Generally need to begin therapyGenerally need to begin therapy
• 20,000-10,000: life-threatening20,000-10,000: life-threatening
- spontaneous bleeding- spontaneous bleeding– Generally requires hospitalizationGenerally requires hospitalization
• <<10,00010,000: risk for spontaneous intracranial : risk for spontaneous intracranial hemorrhagehemorrhage

Causes of
THROMBOCYTOPENIA

Decreased productionMarrow hypoplasia• Childhood bone marrow failure syndromes, e.g.
Fanconi's anaemia, • Idiopathic aplastic anaemia • Drug-induced: cytotoxics, antimetabolites • Transfusion-associated graft-versus-host disease Marrow infiltration• Leukaemia ,Myeloma ,Carcinoma (rare) ,Myelofibrosis • Osteopetrosis • Lysosomal storage disorders, e.g. Gaucher's disease Haematinic deficiency • Vitamin B12 and/or folate deficiency Familial (macro-)thrombocytopathies• Myosin heavy chain abnormalities, e.g. Alport's
syndrome, Fechner's syndrome

Increased consumption of plateletsImmune mechanisms• Idiopathic thrombocytopenic purpura (ITP)* • Post-transfusion purpura • Neonatal alloimmune thrombocytopenia • Drug-associated, especially quinine Coagulation activation• Disseminated intravascular coagulation (DIC) Mechanical pooling• Hypersplenism Thrombotic microangiopathies• Haemolytic uraemic syndrome (HUS) • Liver disease • Thrombotic thrombocytopenic purpura (TTP) Others• Gestational thrombocytopenia • Type 2B von Willebrand disease

Evaluation of Patient with Low Evaluation of Patient with Low PlateletsPlatelets
• History History – Has the patient ever had a normal platelet count?Has the patient ever had a normal platelet count?– Carefully review Carefully review medicationsmedications, including OTC meds., including OTC meds.
• Antibiotics, quinine, anti-seizure medicationsAntibiotics, quinine, anti-seizure medications– Ask about Ask about other conditionsother conditions which may be which may be
associated with low plateletsassociated with low platelets• Liver Disease/hepatitisLiver Disease/hepatitis• Thyroid Disease - both hypo- and hyper-Thyroid Disease - both hypo- and hyper-• Infections: viral, rickettsialInfections: viral, rickettsial• PregnancyPregnancy
– Ask about Ask about other conditionsother conditions which may be associated which may be associated with ITPwith ITP
• Lupus, CLL, lymphomaLupus, CLL, lymphoma

Evaluation of Patient with Low Evaluation of Patient with Low PlateletsPlatelets
• PhysicalPhysical– Evaluate for lymphadenopathy and splenomegalyEvaluate for lymphadenopathy and splenomegaly– Look for stigmata of bleedingLook for stigmata of bleeding– Blood blisters and oral petechiae, ie “Wet Purpura” Blood blisters and oral petechiae, ie “Wet Purpura”
• best harbinger of intracranial hemorrhagebest harbinger of intracranial hemorrhage• Laboratory DataLaboratory Data
– Other blood counts should be normal.Other blood counts should be normal.– Check Check B12 and folateB12 and folate levels. levels. – Look at Look at peripheral smearperipheral smear to exclude to exclude
pseudothrombocytopenia, also exclude TTP (especially pseudothrombocytopenia, also exclude TTP (especially if anemia also present.)if anemia also present.)
– Send coagulation screens (PT/PTT) to exclude DICSend coagulation screens (PT/PTT) to exclude DIC– Send HIV, hepatitis serologies and TSHSend HIV, hepatitis serologies and TSH
• Consider doing a bone marrow biopsyConsider doing a bone marrow biopsy– Megakaryocytes should be presentMegakaryocytes should be present..


Immune/Idiopathic Immune/Idiopathic Thrombocytopenic PurpuraThrombocytopenic Purpura
ITP

ITPITP
• DefinitionDefinition: isolated thrombocytopenia with no : isolated thrombocytopenia with no clinically apparent associated conditions or other clinically apparent associated conditions or other causes of thrombocytopenia.causes of thrombocytopenia.
• EtiologyEtiology: autoantibodies directed against : autoantibodies directed against
glycoprotein IIb/IIIaglycoprotein IIb/IIIa on platelet surface. IgG- on platelet surface. IgG-coated platelets are taken up by RE system.coated platelets are taken up by RE system.
• IncidenceIncidence: approximately 100 per million; half of : approximately 100 per million; half of these are children. In adults, two peaks:these are children. In adults, two peaks:
– one are young (<40) with female predominance, one are young (<40) with female predominance,
– one are older (>60), no gender predominance.one are older (>60), no gender predominance.
Association Association ; connective tissue disease , HIV ; connective tissue disease , HIV infection ,B cell malignency ,drugsinfection ,B cell malignency ,drugs

Clinical presentation
-Abrupt onset (childhood ITP)– Gradual onset (adult ITP)– Purpura– Menorrhagia– Epistaxis– Gingival bleedingPredisposing condition– Recent live virus immunization
(childhood ITP)– Recent viral illness (childhood
ITP)– Bruising tendency


Workup
• CBC – Isolated thrombocytopenia.– Truly giant platelets on peripheral
smear suggest congenital thrombocytopenia.
– The WBC count and hemoglobin typically are normal, unless severe hemorrhage has occurred.
bone Marrow : increase megakaryocyte
• Coagulation studies are normal, and a bleeding time is not useful.

Management ITP
• Asymptomatic pt• Symptomatic pt - initial management -subsequent
management. Relapsed ITP by steroid, splenectomy, anti D immune globulin. Refractory ITP

Management of ITPManagement of ITPAsymptomatic AdultAsymptomatic Adult
• If platelet count is >30 K, If platelet count is >30 K,
no therapy is required. no therapy is required. Check platelet counts at intervals.Check platelet counts at intervals.
• If platelet count is < 30 K, begin If platelet count is < 30 K, begin therapy with therapy with corticosteroidscorticosteroids. .
• Stop all NSAIDS and ASA to improve Stop all NSAIDS and ASA to improve platelet function.platelet function.

Initial Management of ITPInitial Management of ITPAdult with Symptomatic Adult with Symptomatic
PurpuraPurpura• If platelet count is >10, If platelet count is >10,
prednisoneprednisone alone - use 1 mg/kg. alone - use 1 mg/kg.
• If platelet count <10, treat with If platelet count <10, treat with prednisone, but also add prednisone, but also add IVIgIVIg 1g/kg/d 1g/kg/d x 2d. - may require admissionx 2d. - may require admission
• Along with prednisone, add Calcium Along with prednisone, add Calcium and Vitamin D to prevent bone loss.and Vitamin D to prevent bone loss.
• If patient has severe bleeding, may If patient has severe bleeding, may need need platelet transfusionsplatelet transfusions..

Subsequent Management of Subsequent Management of ITPITP
Adult with Symptomatic Adult with Symptomatic PurpuraPurpura• Follow platelet counts daily until >20, then Follow platelet counts daily until >20, then
can d/c patient with close follow-upcan d/c patient with close follow-up• Once platelet count normalizes, commence a Once platelet count normalizes, commence a
slow steroid taperslow steroid taper over 6-8 weeks. over 6-8 weeks.• 1/3 of adults will have gone into remission.1/3 of adults will have gone into remission.• 2/3 of patients will relapse during or after 2/3 of patients will relapse during or after
steroid taper. steroid taper.

Management of Relapsed ITPManagement of Relapsed ITP
• Once the patient relapses, may need to Once the patient relapses, may need to re-introduction of steroids to increase re-introduction of steroids to increase the platelet count out of the danger the platelet count out of the danger range, but range, but THIS CANNOT THIS CANNOT SUBSTITUTE FOR DEFINITIVE SUBSTITUTE FOR DEFINITIVE THERAPYTHERAPY..
• Prednisone is now a crutch to support a Prednisone is now a crutch to support a dangerously low platelet count.dangerously low platelet count.
• Options now include Options now include splenectomysplenectomy (standard of care if 2 relapse) or (standard of care if 2 relapse) or intermittent treatment with intermittent treatment with anti-D anti-D immune globulinimmune globulin . .

Management of Relapsed ITPManagement of Relapsed ITP by Splenectomy by Splenectomy
• effective in 2/3 of patientseffective in 2/3 of patients• Complete remission 70% ,Complete remission 70% ,• improvement in 20-25%improvement in 20-25%• via open method or laparoscopically.via open method or laparoscopically.• vaccinate against encapsulated bacteria vaccinate against encapsulated bacteria
(Pneumococcal ,meningococcal, H. influenzae) (Pneumococcal ,meningococcal, H. influenzae) 2 weeks before procedure.2 weeks before procedure.
• Pen V 500mg BD life long Pen V 500mg BD life long • May need steroids and/or IVIg before May need steroids and/or IVIg before
procedure to boost platelet counts procedure to boost platelet counts preoperatively.preoperatively.

Management of Relapsed Management of Relapsed ITPITP
Anti-D Immune GlobulinAnti-D Immune Globulin• Can be used as a substitute for IVIg for Can be used as a substitute for IVIg for
maintenance therapymaintenance therapy• Especially useful in patients with Especially useful in patients with
contraindications to splenectomy.contraindications to splenectomy.• Coats red cells with IgG and allows red cells Coats red cells with IgG and allows red cells
to serve as decoy for splenic macrophages.to serve as decoy for splenic macrophages.• Patient must be Rh positive. Patient must be Rh positive. • Not effective after splenectomy.Not effective after splenectomy.• Designed to cause hemolytic anemia--Hgb Designed to cause hemolytic anemia--Hgb
may drop as much as 3g/dl.may drop as much as 3g/dl.• Intermittent dosing may allow patients to Intermittent dosing may allow patients to
avoid splenectomy.avoid splenectomy.

Case 1Case 1• A 19 y.o. female college student presents A 19 y.o. female college student presents
with a rash over her lower extremities. with a rash over her lower extremities. She had a viral illness 2 weeks ago. She She had a viral illness 2 weeks ago. She has no other medical problems, and she has no other medical problems, and she takes no medications.takes no medications.
• Physical examination reveals petechiae Physical examination reveals petechiae over the shins.over the shins.
• Platelet count is 20K.Platelet count is 20K.

Case 1…Case 1…
• The patient is begun on The patient is begun on prednisone at 1 mg/kg. prednisone at 1 mg/kg.
• Seven days later, the patient Seven days later, the patient returns, complaining of acne, returns, complaining of acne, insomnia, severe indigestion, insomnia, severe indigestion, and visual hallucinations. and visual hallucinations. The platelet count is 250K. The platelet count is 250K. Prednisone dose is tapered Prednisone dose is tapered over 8 weeks, and the patient over 8 weeks, and the patient remains asymptomatic with remains asymptomatic with normal platelet counts.normal platelet counts.

Case 3Case 3
• A 46 y.o. woman is found to have a A 46 y.o. woman is found to have a platelet count of 20 on routine platelet count of 20 on routine laboratory testing. She has some easy laboratory testing. She has some easy bruising and gum bleeding, but admits bruising and gum bleeding, but admits to not flossing. to not flossing.
• She has no PMHx, and is on no She has no PMHx, and is on no medications. She works as a school medications. She works as a school principal.principal.
• She is started on 1 mg/kg of prednisone. She is started on 1 mg/kg of prednisone.

Case 3..Case 3..• After 1 week, the platelet count is 180, and After 1 week, the platelet count is 180, and
the prednisone dose is tapered by 10 mg the prednisone dose is tapered by 10 mg per week. When she reaches a dose of 10 per week. When she reaches a dose of 10 mg qd, the patient develops severe mg qd, the patient develops severe menstrual bleeding and is noted to have a menstrual bleeding and is noted to have a platelet count of 8k.platelet count of 8k.
• She is admitted to the hospital, and is She is admitted to the hospital, and is begun on IVIg at 1g/kg IV qd x 2d. The begun on IVIg at 1g/kg IV qd x 2d. The prednisone dose is increased to 60 mg prednisone dose is increased to 60 mg daily. By the third day, the platelet count daily. By the third day, the platelet count is 60K.is 60K.

Case 3..Case 3..
• The patient is vaccinated against The patient is vaccinated against pneumococcus, meningococccus, and pneumococcus, meningococccus, and Hemophilus influenzae. Hemophilus influenzae.
• She undergoes laparascopic She undergoes laparascopic splenectomy, which is uneventful. The splenectomy, which is uneventful. The platelet count rises to 600K. She is platelet count rises to 600K. She is successfully weaned off steroids. successfully weaned off steroids.

Management of Refractory Management of Refractory ITPITP
• One third of patients will have an One third of patients will have an inadequate response to inadequate response to splenectomy.splenectomy.
• Management of these patients Management of these patients involves accepting that they have involves accepting that they have a chronic, incurable condition.a chronic, incurable condition.
• Target platelet counts should be Target platelet counts should be lower--aim for about 30K or lower--aim for about 30K or absence of bleeding.absence of bleeding.

Treatment of Refractory ITPTreatment of Refractory ITP• Immunosuppressive agentsImmunosuppressive agents
– Rituximab (anti-CD20)Rituximab (anti-CD20)• 40% effective40% effective• May be used before splenectomy May be used before splenectomy
– Mycophenolate mofetilMycophenolate mofetil– CyclophosphamideCyclophosphamide
• Adjunct agentsAdjunct agents– Thrombopoietin Receptor AgonistsThrombopoietin Receptor Agonists
• RomiplostimRomiplostim• EltrombopagEltrombopag

Drug induced
Thrombocytopenia

Drugs Commonly Drugs Commonly Implicated in Implicated in
ThrombocytopeniaThrombocytopenia• Beta-lactam antibiotics.Beta-lactam antibiotics.• Trimethoprim-sulfamethoxazole Trimethoprim-sulfamethoxazole
and other sulfa drugs.and other sulfa drugs.• Vancomycin.Vancomycin.• Quinine/quinidine.Quinine/quinidine.• Heparin.Heparin.• Abciximab .Abciximab .• HH22 blockers blockers• If a patient’s platelets fall, ALL If a patient’s platelets fall, ALL
unnecessary drugs need to be unnecessary drugs need to be stoppedstopped..
• give platelet transfusions , IVIg is give platelet transfusions , IVIg is particularly helpful in quinine-particularly helpful in quinine-induced ITP. ,induced ITP. ,

Case 4Case 4• A 55 y.o. woman presented with A 55 y.o. woman presented with
bleeding from her nose and mouth bleeding from her nose and mouth and gums. and gums.
• PMHx - HTN, DM, DJDPMHx - HTN, DM, DJD• Medications - glucotrol, Medications - glucotrol,
glucophage, HCTZ, quinine for leg glucophage, HCTZ, quinine for leg crampscramps
• PEx - petechiae over limbs and PEx - petechiae over limbs and torso, blood blisters in mouth, torso, blood blisters in mouth, epistaxis.epistaxis.
• Platelet count 2KPlatelet count 2K

Case 4Case 4
• Pt admitted to hospital, Pt admitted to hospital, quinine stopped, patient quinine stopped, patient treated with platelet treated with platelet transfusions and IVIg.transfusions and IVIg.
• Platelet count rose to normal Platelet count rose to normal over the next 5-6 days.over the next 5-6 days.
• Eight months later, Eight months later, thrombocytopenia recurred, thrombocytopenia recurred, and patient admitted to and patient admitted to taking quinine again for taking quinine again for recurrent leg cramps.recurrent leg cramps.

Heparin induced
Thrombocytopenia

Heparin-Induced Heparin-Induced ThrombocytopeniaThrombocytopenia• Seen in 1-3% of patients treated Seen in 1-3% of patients treated
with heparinwith heparin
• Usually, 7-10 d after heparin Usually, 7-10 d after heparin started, platelets fall by at least 1/3 started, platelets fall by at least 1/3 to 1/2. to 1/2. – Patients Patients do not have to be do not have to be
thrombocytopenicthrombocytopenic. . – Can occur earlier in patients who Can occur earlier in patients who
have been previously exposed to have been previously exposed to heparin, even as SQ injections.heparin, even as SQ injections.
• Caused by antibodies against the Caused by antibodies against the complex of heparin and PF4. These complex of heparin and PF4. These antibodies activate platelets.antibodies activate platelets.
• Can lead, paradoxically, to Can lead, paradoxically, to THROMBOSISTHROMBOSIS, in up to half of , in up to half of patients.patients.
• More common in patients with More common in patients with vascular diseasevascular disease

HIT/T treatmentHIT/T treatment
1.1. IF PLATELETS FALL ON IF PLATELETS FALL ON HEPARIN, STOP HEPARIN HEPARIN, STOP HEPARIN IMMEDIATELY.IMMEDIATELY.
2.2. Stop heparinStop heparin3.3. Stop heparinStop heparin4.4. Use a different Use a different
anticoagulantanticoagulant1.1. Lepirudin Lepirudin 2.2. ArgatrobanArgatroban

Thrombotic Thrombocytopenic
Purpura
( TTP )

TTP - Diagnostic Features TTP - Diagnostic Features • Microangiopathic Hemolytic Anemia Microangiopathic Hemolytic Anemia
(MAHA)(MAHA)– Elevated LDH, elevated bilirubinElevated LDH, elevated bilirubin– SchistocytesSchistocytes on the peripheral smear on the peripheral smear– MUST BE PRESENTMUST BE PRESENT
• Low platelets - MUST BE PRESENTLow platelets - MUST BE PRESENT• FeverFever• Neurologic ManifestationsNeurologic Manifestations - headache, - headache,
sleepiness, confusion, stupor, stroke, coma, sleepiness, confusion, stupor, stroke, coma, seizuresseizures
• Renal ManifestationsRenal Manifestations - hematuria, - hematuria, proteinuria, elevated BUN/Creatinineproteinuria, elevated BUN/Creatinine
• Abdominal PainAbdominal Pain - can see elevated - can see elevated lipase/amylaselipase/amylase

TTP - etiologyTTP - etiology• May be associated with an May be associated with an
antibody against or a antibody against or a deficiency of the protease deficiency of the protease which cleaves the ultra-high which cleaves the ultra-high molecular weight multimers molecular weight multimers of von Willebrand’s factor. of von Willebrand’s factor. These very high molecular These very high molecular weight vWF multimers cause weight vWF multimers cause abnormal platelet activation. abnormal platelet activation.
• Can be induced byCan be induced by drugsdrugs, , including ticlopidine, quinine, including ticlopidine, quinine, cyclosporine, tacrolimus, cyclosporine, tacrolimus, mitomycin C.mitomycin C.
• Increased incidence with Increased incidence with pregnancypregnancy or or HIVHIV

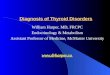
TTP -lab
CBC normal or slightly elevated WBC.
• Hemoglobin is moderately depressed at 8-9 g/dL.
• Platelet count ranges from 20,000-50,000 per microliter.
• Peripheral smear : Red blood cells are fragmented and appear as schistocytes. Certain schistocytes have the appearance of helmet cells (H). Spheroidal cells often are present (S). Occasional nucleated erythroid precursors may be present.

TTP - Course and TTP - Course and PrognosisPrognosis
• 95% fatal prior to therapy, now 5% fatal.95% fatal prior to therapy, now 5% fatal.• Treatment relies on Treatment relies on PLASMA EXCHANGE.PLASMA EXCHANGE.
– Plasma exchange is superior to plasma Plasma exchange is superior to plasma infusion, but if PLEX is delayed, give FFP.infusion, but if PLEX is delayed, give FFP.
• Remove all inciting agents.Remove all inciting agents.
• Platelet transfusions contra-Platelet transfusions contra-indicated.indicated. – Multiple case reports of stroke and/or death Multiple case reports of stroke and/or death
during or immediately after platelet during or immediately after platelet transfusion.transfusion.
– Can consider giving if life-threatening Can consider giving if life-threatening hemorrhage is present, but avoid routine hemorrhage is present, but avoid routine platelet transfusions.platelet transfusions.
• Secondary measures if no response to Secondary measures if no response to plasma exchange include plasma exchange include splenectomysplenectomy, , vincristinevincristine

DIC
• Pathophysiology 4 simultaneously occurring mechanisms:• TF-mediated thrombin generation
• Dysfunctional physiologic anticoagulant mechanisms (eg, depression of antithrombin and protein C system),
• Impaired fibrin removal due to depression of the fibrinolytic system –
caused by high circulating levels of plasminogen activator inhibitor type 1 (PAI-1);
• Inflammatory activation

Underlying conditions
• Infection/sepsis • Trauma • Obstetric, e.g. amniotic fluid embolism,
placental abruption, pre-eclampsia • Severe liver failure • Malignancy, e.g. solid tumours and
leukaemias • Tissue destruction, e.g. pancreatitis,
burns • Vascular abnormalities, e.g. vascular
aneurysms, liver haemangiomas • Toxic/immunological, e.g. ABO
incompatibility, snake bites, recreational drugs

DIC- Presentations
Bleeding 64%
Renal dysfunction 25% Hepatic dysfunction 19% Respiratory dysfunction 16% Shock 14% CNS dysfunction 2%

INV--DIC
• PT - increased• APTT - increased• Fibrinogen - decreased• FDP - increased

RX --DIC
• focus on addressing underlying disorder
• Administration of Blood Components and Coagulation Factors – platelet , FFP, cryopricipitate
• Anticoagulation – heparin,proteinC
• Patients with DIC should not in general be treated with antifibrinolytic therapy, e.g. tranexamic acid.


HUS - Hemolytic Uremic HUS - Hemolytic Uremic SyndromeSyndrome
• Usually classified along with TTP Usually classified along with TTP as “TTP/HUS”as “TTP/HUS”
• Has fewer neurologic sequelae, Has fewer neurologic sequelae, more renal manifestations.more renal manifestations.
• Usually precipitated by diarrheal Usually precipitated by diarrheal illness, especially illness, especially E. coli O157:H7E. coli O157:H7 or Shigellaor Shigella
• Seen more in pediatric patients, Seen more in pediatric patients, usually has better prognosis. May usually has better prognosis. May respond less well to plasma respond less well to plasma exchange.exchange.

THANK YOU