Embed Size (px)
DESCRIPTION
A brief presentation of CMV in Kidney Transplantation
Citation preview
CMV in Kidney TransplantArun Chawla, MD
Hofstra North Shore –LIJ School of Medicine
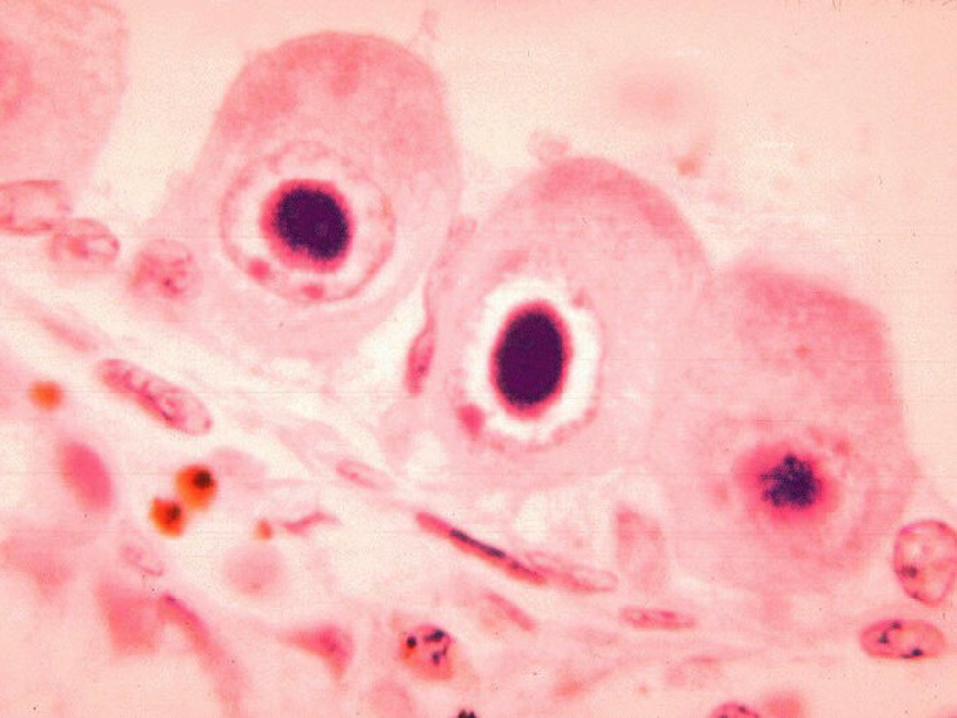
What is CMV??What is CMV?? Double-stranded, DNA herpesvirus that infects man and
other species, producing unique large cells with inclusion bodies.
Also known as human herpesvirus # 5 or HHV-5
In immunocompentent individuals, most CMV infections are mild and may produce a viral syndrome resembling infectious mononucleosis.
Approximately 50 - 90% of immunocompetent adults >40 years old have antibodies (IgG) to CMV. In otherwise healthy adults, CMV remains inactive or latent, but ready to be become active under “favorable conditions”.
Why should we know Why should we know CMV??CMV??
CMV is the most common and single most important viral infection in solid organ transplant recipients.
CMV-positive patients had significantly higher incidence of CMV disease, allograft loss, and overall costs compared with CMV-negative recipients.
Even asymptomatic CMV infection was associated with a relative risk of overall mortality of 2.9
CMV is found in oropharyngeal secretions, urine, cervical and vaginal secretions, semen, breast milk, tissues and blood.
It can be transmitted via transplanted tissue, blood transfusion, perinatally, and through sexual contact
CMV infectionCMV infection seroconversion with the appearance of anti-CMV IgM
antibodies;
a fourfold increase in preexisting anti-CMV IgG titers;
detection of CMV antigens in infected cells;
detection of CMV-DNAemia by molecular techniques;
and/or isolation of the virus by culture of the throat, buffy coat, or urine.
CMV DiseaseCMV Disease CMV Infection + clinical signs and
symptoms, such as fever, leukopenia, or organ involvement
pneumonitis,
esophagitis,
encephalitis,
hepatitis,
pancreatitis,
adrenalitis,
esophagitis,
.gastritis
enteritis & colitis
rarely myocarditis
Retinitis
Also…Also… Alters host response and depresses immunity
Presdisposes to bacterial and fungal infections
CMV-induced transplant glomerulopathy
independent risk factor for the development of rejection
development of coronary artery narrowing
significantly associated with renal artery stenosis
associated with thrombotic microangiopathy (HUS/TTP)
Types of CMV InfectionTypes of CMV Infection Primary infection - (asymptomatic to mononucleosis like
syndrome in immune competent individuals)
Latent infection - (presence of viral genome in mononuclear leukocytes, endothelial cells, and organs in the absence of active replication of infectious virus)
Reactivation
Reinfection (new strain of CMV)
Risk FactorsRisk Factors CMV status of donor and recipient
The number of CMV particles
Rate of increase of virus in the blood correlated with the risk of developing CMV disease
Correlation of CMV DNA levels with response to antiviral therapy in cardiac and renal allograft recipients.Toyoda M et al Transplantation 1997 Apr 15;63(7):957-63.
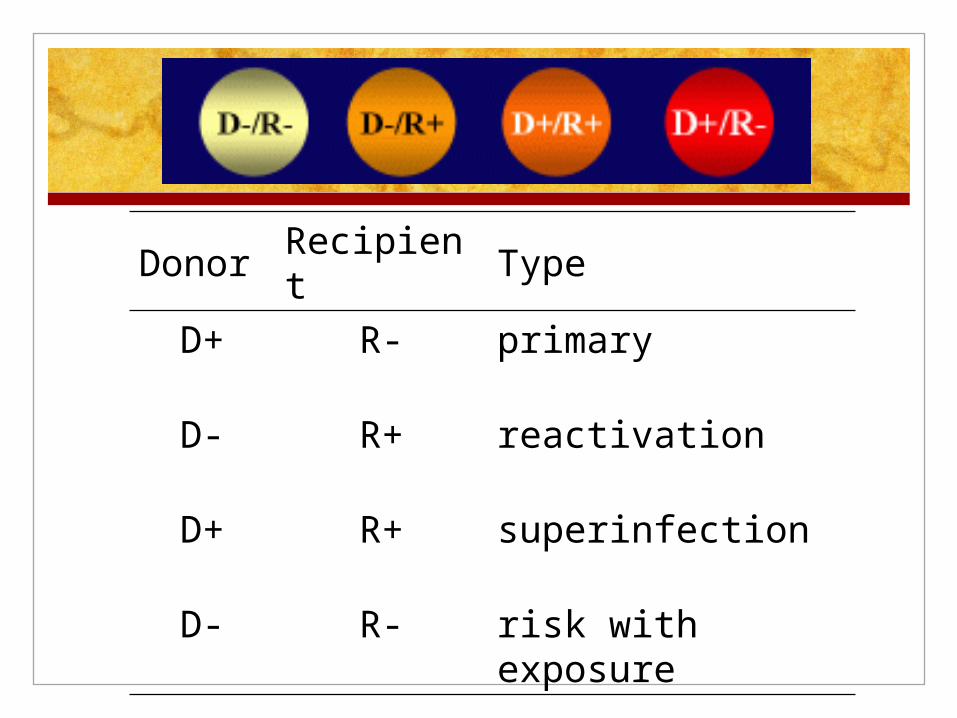
Donor Recipient Type
D+ R- primary
D- R+ reactivation
D+ R+ superinfection
D- R- risk with exposure
PreventionPrevention Infection rates of upto 60% without prophylaxis have come
down to as low as 5 % with prophylaxis.
A prophylactic strategy - antiviral agents to patients at increased risk of developing CMV infection.
A preemptive strategy - periodic monitoring for viremia, principally using PCR to permit prompt treatment after the detection of very early systemic infection.
So what do we do?
Meta-analysis: the efficacy of strategies to prevent organ disease by CMV in solid organ transplant recipients. Kalil AC et al Ann Intern Med. 2005 Dec 20;143(12):870-80.
Agents for ProphylaxisAgents for Prophylaxis Ganciclovir was superior to acyclovir or CMV Ig
Gancilcovir (i.v. vs. po)
Valganciclovir vs. ganciclovir – PV 16000 - 1 percent of patients developing CMV disease while receiving therapy. Time-to-onset of CMV disease and to viremia were delayed with valganciclovir; rates of acute allograft rejection were generally lower with valganciclovir.Also, lower resistance (2% vs. none). Caution with neutropenia.
Investigative phase – leflunamide, valacyclovir.
Efficacy and safety of valganciclovir vs. oral ganciclovir for prevention of CMV disease in solid organ transplant recipients. Paya C et al. J Transplant 2004 Apr;4(4):611-20.
Choice and durationChoice and duration D-/R- with acyclovir for 3 months
D-/R+ - with valganciclovir for 3 - 6 months
D+/R+ and D+/R- with valganciclovir for 6 - 9 months.
The worst graft and patient survival at three years post-transplantation is observed among the group in which the donor and recipient are both positive.
CMV status & HLA-DR CMV status & HLA-DR matchingmatching
CMV disease occurred most frequently in D+/R- recipients with zero HLA-DR matches.
In addition, allograft survival at five years was significantly decreased among those with CMV disease and zero matches compared to patients with CMV disease and one or two HLA-DR matches (16 versus 76 percent, respectively).
These results suggest that, to enhance allograft survival, consideration should be given to HLA-DR matching plus CMV status in the allocation of kidneys.
Preemptive strategyPreemptive strategy blood quantitative CMV-PCR weekly for 12 to 16 weeks post-
surgery.
CMV-PCR becomes positive, > 2000 copies/mL, approach varies in part upon the severity of the infection:
a) Stop azt or MMF
b) Asymptomatic/Mild disease – valganciclovir for 21 days or longer if necessary to clear viremia.
c) Weekly quantitative PCRs should be obtained during treatment to determine response. If levels no less by 50% in two weeks, viral resistance should be suspected. Consider i.v. then.
Diagnosis of CMVDDiagnosis of CMVD Symptoms and signs consistent with CMV disease together with detection of
CMV by an appropriate method applied to a specimen from the involved tissue (AII).
Symptoms of organ involvement together with CMV detection in blood are not
enough for diagnosis of CMV disease. Detection of CMV in tissue specimens is important (AII).
Symptomatic CMV infections typically occur 1-4 months after transplantation if prophylaxis is not used or one to four months after discontinuation of prophylaxis
TreatmentTreatment The mononucleosis-like syndrome may resolve without the administration of
antiviral drugs.
Discontinue azt/MMF
Usually do not discontinue cyclosporine or tacrolimus unless there is evidence of life-threatening infection
i.v. ganciclovir (life threatening infections or npo)
Oral?? VICTOR study
Oral ganciclovir, acyclovir, or valacyclovir should not be used for treatment of CMV disease
The role of CMV immunoglobulin in the treatment of CMV disease is unclear. It may be considered as adjunc- tive therapy for severe forms of CMV disease such as pneumonitis
Oral valganciclovir is noninferior to intravenous ganciclovir for the treatment of cytomegalovirus disease in solid organ transplant recipients. Asberg A et al. J Transplant. 2007 Sep;7(9):2106-13
Duration of t/tDuration of t/t monitoring weekly viral loads & continued until viral
eradication is achieved, but not shorter than 2 weeks
Follow renal function and adjust dose
Secondary prophylaxis – 1-3 months
Longer if - primary CMV infection, DDT, high baseline viral load, persistent viremia when transferred to secondary prophylaxis, multiorgan disease, and treatment of rejection.
Several CMV vaccines are under development; none are currently available for routine clinical use.
Thank You Thank You …………….…………….