Embed Size (px)
Citation preview

Natural plant-based product outperforms nicotine replacement therapy in NZ trialBy Suzy Botica
A New Zealand study recently published in the New England Medical Journal has shown that a low-cost product found in plants such as Golden Rain is more effective at helping people quit smoking than the more expensive and widely used nicotine replacement therapy.
Dr Natalie Walker from the University of Auckland led the HRC-funded study into cytisine, a naturally occurring plant alkaloid sourced from Bulgaria that has been sold in Eastern Europe as an inexpensive smoking-cessation aid since the 1960s, but is unavailable – and relatively unknown – elsewhere. This is the first trial in the world to have compared the effectiveness of cytisine with nicotine replacement therapy (NRT).
The study team recruited 1310 adult daily smokers from New Zealand who were motivated to quit and had called the national Quitline. The participants were randomly assigned to either receive cytisine for 25 days or NRT (in the form of patches and/or gum or lozenges) for eight weeks.
Participants in both groups also received telephone-based Quitline behavioural support.
The proportion of study participants who managed to continuously abstain from smoking over a one-month period was higher for those in the cytisine group (40 per cent) than for those in the NRT group (31 per cent). Cytisine also remained more effective than NRT at keeping participants smoke-free at the two-month and six-month follow ups.
The effects of cytisine appear to be longer-lasting than NRT as well. Participants in the cytisine group who didn’t succeed in quitting smoking, took much longer to resume smoking again after the trial’s designated ‘quit day’ than those in the NRT group: 53 days for the cytisine group compared to just 11 days for the NRT group.
Dr Walker says that cytisine looks a bit like nicotine to the brain, which is how it works to reduce the severity of smokers’ nicotine cravings.
“During treatment we found that participants in the cytisine group reported fewer symptoms of tobacco withdrawal, found smoking less rewarding, and reduced the number of cigarettes they smoked each day,” says Dr Walker.
Cytisine wasn’t without its drawbacks. Participants taking cytisine reported more side effects than those in the NRT group, most commonly nausea, vomiting, and sleep disorders. However, the side effects were similar to those observed in patients taking varenicline – the most effective smoking cessation treatment available on the market.
HRC news
Issue No. 83 March 2015
INSIDE
Potential vaccines for cancer and asthma
Dr Natalie Walker
(Continued on page 7)
In the HRC 2010 annual funding round, Dr Natalie Walker was awarded over $1 million for her project to investigate a new low-cost intervention for smoking cessation.
Expressions of Interest for Projects for the HRC’s 2016 funding round open on 15 June 2015. For more information go to www.hrc.govt.nz/funding-opportunities/researcher-initiated-proposals.
Find out what these vaccines have in common on pages 18 and 19.
2
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Chief Executive’s message2014 was a big year of change for the Health Research Council of New Zealand. As the new Chief Executive (in post for about three weeks as I write this) I will sorely miss the input of Lex Davidson. I am one of many researchers who has benefited from his flexibility and understanding of the need for the ‘occasional’ no-cost extension and related contract amendment. I had imagined that I would be able to seek his wise counsel during my first year in post, but sadly that was not to be. You can tell from this issue that he is greatly missed here – and I have heard from many research offices and researchers around the country that they too will miss him enormously. Our thoughts are with his family at this time.
I have spent my first few weeks getting to know staff, and kick-starting the process of meeting with/talking to key stakeholders around New Zealand. Gaining an understanding of the ‘whole of HRC’ business, and its place in the ‘whole of health research’ context is something I am really enjoying. Part of this process is being augmented by projects we have underway exploring better ways to evaluate the impact of the research that we support. I look forward to sharing some of the information we are collating and synthesising as and when it is available.
How best to evaluate the impact of health research is inherently complex and problematic, but demonstrating ‘value add’ is crucial and something we are committed to doing. Knowledge about impact is much aided by the information you provide in annual and final reports about publications, spin-off projects that build on the HRC-funded work, and of course the changes your work brings about in practice, policy and education. Our intention is that it will become far simpler for researchers to do that with revisions to HEARD (the HRC’s online reporting system), and its integration into HRC Gateway. But, if you have stories about the impact of your work, don’t wait for your report - talk to us! The stories in this issue are just some of the examples that exist – we would welcome you letting us know more.
At the end of January 2015, I had the opportunity to meet with officials from the Ministry for Business, Innovation and Employment and European funders about the Joint Programming Initiative on Healthy Diet, Health Living (JPI- HDHL) and the Global Alliances for Chronic Diseases (GACD) and Infectious Disease Preparedness (GLOPID). One of the things that really came across in all of these meetings is the
IN THIS ISSUE
A tribute to Lex Davidson (1947–2014) 3
Reflection of Lex 5
Tribute message from Sir Robert Stewart, KNZM
6
Strategic refresh of the HRC announced 7
Study identifies ways to make cycling safer on NZ roads
8
PubMed Commons: A forum for scientific discourse
9
Harnessing wireless power for artificial heart pumps
10
E-therapy for youth depression in primary care
11
Unique study to explore NZ’s ‘puzzling’ testicular cancer rates
12
Virus hunters’ make new discovery while studying unsolved gastro outbreaks
14
Rotavirus vaccine trial a success 15
Shaping palliative care for Māori 17
Asthma and cancer vaccine research crossover
18
Right dose – right result 20
HRC Chief Executive, Dr Kathryn McPherson
Follow the HRC on Twitter
If you’d like an easy way to keep up with the latest HRC news, you can follow us on Twitter: @HRCNewZealand.

3
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
positive regard with which New Zealand health research and researchers are held. Part of our mandate is to contribute to ensuring that regard is maintained and indeed grows. This is no mean feat and yet it is what attracted me to this position.
We are now well and truly into the assessment process for the annual contestable funding round (see www.hrc.govt.nz/news-and-publications for rebuttal submission dates). This will be the first year I will not be dealing with reviews of my own grants (always a mixed blessing I find with around 160 of you having a similar sense I suspect in the weeks to come). However, those reviews, and the associated rebuttals, contribute to thoughtful discussion and informed decisions in our assessing committees. What I am seeing first-hand is just how many reviewers the HRC engages with to meet our objective of three to four independent reviews for each grant. A rough estimate is that we are in contact with about 1600 academics nationally and internationally during this time frame. It’s a mammoth
undertaking as you can imagine so – next time you are asked to review – if it’s within your area of expertise, please consider saying yes!
Finally – congratulations to Professor Anne Kelso who takes over from Professor Warwick Anderson as the new Chief Executive of the National Health and Medical Research Council in Australia in April, and enormous thanks to the staff and board of the HRC for making me welcome and for teaching me so much. Here’s to 2015 being a really good year for the contribution that the HRC, and health research, makes for New Zealanders.
Dr Kathryn McPherson, Chief Executive, Health Research Council of New Zealand
A tribute to Lex Davidson(1947–2014)By Dr Bruce A Scoggins, PhD(HRC Chief Executive from 1991 to 2006)
Lex was appointed Manager Finance and Corporate Services at the HRC in January 1991 immediately following the transition of the Medical Research Council to the Health Research Council of New Zealand. I joined the staff in October 1991 and Lex and I worked closely together for the next 15 years to ensure that the council’s financial accounts, accountability statement and performance measures met the requirements of the Government, the HRC Board, and Audit New Zealand.
Balancing income from the Government with a range of research funding initiatives of different duration required Lex to
develop an approach which ensured funds were being used effectively – not sitting unused in either in the HRC’s or a host institution’s bank account. Development of an appropriate strategy was skillfully managed by Lex through engagement
with the HRC’s Board and the staff administering research funds at the various host institutions.
It was never easy matching the research community’s and the HRC’s Research Committees’ desire for increased funding to support more research with the Government’s budget allocation.
Together with the Board, Lex often had the dual challenges of tempering expectations for increased health research funding from the
HRC’s Research Committees and stakeholders, and dealing with the fiscal realities of the Government’s budget allocation, which was often not negotiated on the three-yearly cycle required by the HRC Act.
The transition, over four years, to full cost funding of research conducted at the same time (1997/98) as the transfer of the HRC’s funding from Vote Health to Vote Research, Science
Lex Davidson
Dr Bruce Scoggins
(Continued on page 4)
4
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Upcoming closing datesFor an up-to-date list of all application registration, opening and closing dates please go to the HRC website: www.hrc.govt.nz.
Ngā Kanohi Kitea Full Project Grant Full applications close 8 April 2015 (1pm)Hard copies of full applications due at the HRC by 10 April 2015 (5pm)
Full applications:Clinical Practitioner Research Fellowship The Sir Charles Hercus Health Research Fellowship Clinical Research Training Fellowship Foxley Fellowship Online submissions open 4 June 2015 (8am) Online submissions close 1 July 2015 (12pm, noon) Hard copies due at the HRC by 3 July 2015 (5pm)
Projects – Expression of Interest Online submissions open 15 June 2015 (8am)Online submissions close 15 July 2015 (12pm, noon)Hard copies due at the HRC by 17 July 2015 (5pm)
Projects – Full application (Invitation only) Online submissions open 6 October 2015 (8am)Online submissions close 18 November 2015 (12pm, noon)
Hard copies due at the HRC by 20 November 2015 (5pm)
Programmes – Full application Online submissions open 10 August 2015 (8am)Online submissions close 14 October 2015 (12pm, noon)Hard copies due at the HRC by 16 October 2015 (5pm)
Full applications:Emerging Researcher First Grant Feasibility Studies Online submissions open 10 August 2015 (8am)Online submissions close 4 September 2015 (12pm, noon)Hard copies due at the HRC by 8 September 2015 (5pm)
Explorer Grants – Full application Online submissions open 1 October 2015 (8am)Online submissions close 4 November 2015 (12pm, noon)Hard copies due at the HRC by 6 November 2015 (5pm)
and Technology was well managed by Lex and the Secretariat Executive Management team. Since the transition of its funding the HRC has been accountable to two ministries1, which is uncommon for a Crown entity.
Both the transition of the HRC’s funding and the move to full-cost funding fully utilised Lex’s skills. Of particular importance was his validation of the overhead rates to be used by host institutions on fully costed contracts.
Lex also played a significant role in the financial planning of the HRC’s joint funding initiatives with other agencies and the HRC’s Partnership Programme. The latter was developed
by Drs Patricia Anderson and Michelle Sullivan, with my assistance.
As the manager of Corporate Services, Lex, together with the administration managers ensured that the Secretariat staff had a great working environment, originally in Symonds Street, but since 2002, in Stanley Street in Auckland.
In his 24 years at the HRC, Lex worked with seven HRC Board Chairs and two Chief Executives. He was also Acting Chief Executive on a number of occasions, including before and after Dr Robin Olds’ tenure.
The HRC’s annual report to Parliament was prepared to a significant extent by Lex and his team. Over the years this has become a significant task with the
inclusion of a substantive number of performance measures.
Lex was ably supported in the accounts office by a hardworking and loyal finance team, led by Sandra Burge. He was also a great support to me in my 15 years as Chief Executive of the HRC.
This year is the 25th anniversary of the establishment of the HRC, and although Lex will not be with us, we will all be thinking of him as we celebrate the achievements of the organisation.
His enthusiasm, commitment and loyalty will be greatly missed!
1 Health and Research, Science and Technology
(Continued from page 3)
5
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Reflection of LexWhen I asked my colleagues at work about Lex
Can you give me one word that first comes to your head? I got naughty and cheeky, a jokester, a clown
Humorous, generous, mischievous man-about town Yes there’s no denying, it must be said
He’s a comic, a prankster, he’d mess with your head!
One day he said “Burgie I’ll help you to your car” How nice I thought, geez Lex you’re a star
But I did not know, he’d been up to his tricks He’d been down to my car and something he’d fixed
To my door handle, I let out a scream A weta just sat there, as if in a dream.
I remember one morning I sat down at my desk I reached for my mouse, what was there was grotesque!
Yes Lex he had been up to his tricks – oh once more The sod – and this time I let out a roar
Instead of my small metal handheld device Lay a mouse, it really was not very nice.
Now there’s one more word that I got – it stood out “Foodie” he’s that, oh yes – there’s no doubt
Yes we all know that our Lex – he liked to cook He even wrote his own “Good Gobbles” cook book
And when someone was sick, you could always rely On Lex, to bake something to help you get by.
Some days he’d come into the office with food And he’d jiggle and dance about, sometimes quite rude
“What is it? he’d say “go on and guess” And the side of his mouth would slide up in jest
He’d swear it was possum or rabbit or eel He could make anything into a meal!
We’d look at it, sniff at it, poke it and think Is this food something we really can eat?
It was often weird stuff he’d bought back from his travels We wondered if eating would make us unravel
And Lex, he would hover, and watch us with glee As we ate some strange critter from trips overseas.
I remember one day we both heard a loud bang And to his window we quickly both ran Down on the ground a wood pigeon lay
That poor bird, could not fly up and away I swear I could see a glint in Lex’s eye
He was thinking of making a yummy bird pie!
At work we often have team building days Dress up for the occasion our invite would say
When he was put in a team called “Colour Blue” He quickly made all of their food, turn this hue
And I think that he had a fetish for tights The costumes he came in were such a delight!
Lex was Robin Hood, Blackbeard and Santa Claus too There was simply nothing this man would not do
One year we had a Mexican theme And that year I have to say – Lex was supreme
He came in his hat and white mafia suit He did sneaky dealings, made funds to boot!
I’ve worked a few places around town in my time And had a few bosses, who’ve kept me in line
But there’s one who stands out, atop of the rest There’s no doubt about it, Lex is the “Best of the Best!”
By Sandra “Burgie” BurgeHRC Finance Administrator,
and colleague of Lex Davidson for 24 years
Lex Davidson at the 2009 New Zealand Science Honours Dinner (Photo courtesy of the Royal Society of New Zealand)

6
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Secretariat staff newsThe HRC Board Chair, Board members and Secretariat were delighted to welcome Dr Kathryn McPherson to the HRC in January as the HRC’s new Chief Executive.
Dr McPherson is an experienced public health researcher and has worked in the research field for over 16 years to improve the health of people with disabling conditions. Dr McPherson is author or co-author of more than 150 peer-reviewed journal articles. She has already had some experience working with the HRC, having served two terms on the HRC’s Public Health Research Committee.
Dr McPherson holds a PhD from the University of Edinburgh. She has clinical experience in nursing midwifery and community health, and an academic background in psychology and rehabilitation. In addition to having held appointments at AUT University, University of Otago, the University of Auckland, and Victoria University, Dr McPherson is Visiting Professor at a number of international universities.
HRC Board Chair Sir Robert Stewart, KNZM, says the board is thrilled to have someone of Dr McPherson’s standing in the research community lead the HRC into the future, and the HRC Board and Secretariat look forward to working with her.
Dr McPherson is looking forward to working with the sector to achieve HRC’s mission, and to that end will meet with a range of stakeholders and researchers from around New Zealand over the coming months, including those from universities, government departments, district health boards, and non-governmental organisations. Details about Dr McPherson’s plans to meet with HRC stakeholders will be publicised in future
issues of HRC News and HRC Update.
Welcome back to Rebecca Luther who has returned to the Research Policy, Strategy and Evaluation team from parental leave. Rebecca has resumed her role as Senior Policy Analyst working three days a week (Wednesday, Thursday and Friday). Many thanks to Pauline Curtis who filled in during Rebecca’s parental leave and who has since moved on to a new role at AUT University. We wish Pauline all the very best.
It’s also welcome back to Senior Evaluations Analyst Megan Biles, who is working three days a week (Monday, Wednesday and Friday) as part of the Research Policy, Strategy and Evaluation team.
We’re pleased to announce that Grant Barnett has been appointed as the HRC’s new Finance Manager. Grant comes to the HRC from the Auckland District Health Board and he will take on many of the responsibilities previously held by the HRC’s Chief Financial Officer, Lex Davidson, who sadly passed away in December 2014. Grant joins the HRC this month and we look forward to working with him.
The HRC’s former Chief Executive, Dr Bruce Scoggins, has written a special tribute to Lex Davidson, which can be found on page 3 of this issue of HRC News.
In November 2014 Stacey Pene’s fixed-term contract role with the HRC’s Maori Health Research team ended. The HRC would like to thank Stacey for the contribution he has made to the HRC during his time here, and wish him all the best for his future career.
Tribute message from Sir Robert Stewart, KNZMLex Davidson, the HRC’s Chief Financial Officer was a man I really admired. He had many great qualities, but one feature that was outstanding, in my opinion, was that he was scrupulously honest.
Lex had worked for the HRC for over 24 years, and he will be greatly missed by the HRC Board and staff of the Secretariat, and many others who had had the pleasure to work with him. Sir Robert Stewart,
KNZM, HRC Board Chair
7
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Dr Walker says one of the most compelling reasons to make cytisine more widely available is the cost. Cytisine is commercially produced in Bulgaria and Poland, and doesn’t have a patent attached to it. As a result, it is significantly cheaper than NRT and varenicline (cytisine: US$20 to $30 for 25 days; NRT: US$112 to $685 for 8 to 10 weeks; varenicline: US$474 to $501 for 12 weeks).
“More affordable smoking cessation treatments are urgently needed,” says Dr Walker. “In New Zealand both NRT and varenicline are heavily subsidised by the government. This trial has shown that cytisine is more effective than NRT and considerably cheaper than both NRT and varenicline,
so big cost savings are possible if cytisine was licensed and marketed outside of Eastern Europe.”
Following on from this study, Dr Walker hopes to secure funding to carry out a head-to-head trial to see if cytisine is as good as varenicline for helping people quit smoking.
Information: Dr Natalie Walker National Institute for Health Innovation, the University of Auckland✆ +64 9 923 [email protected]
(Continued from page 1)
Strategic refresh of the HRC announcedThe HRC Board Chair, Sir Robert Stewart, KNZM, recently received a letter from the Science and Innovation Minister, Hon Steve Joyce and Health Minister, Hon Jonathan Coleman outlining their intent to undertake a strategic refresh of the Health Research Council of New Zealand (HRC). The ministerial press release about the nature and purpose of the refresh can be found at www.beehive.govt.nz/release/health-research-council-review-underway. The HRC is pleased to be involved in disseminating information about the refresh to key stakeholders.
Why undertake a refresh? The Government has called for the refresh to examine how HRC’s contribution fits with the Government’s broad health and economic goals. Ministers have expressed support for our role in supporting what is recognised internationally as New Zealand’s high performing health research sector. They see the refresh as an opportunity to facilitate HRC’s role and contribution, and to capture our relevance, efficiency, effectiveness and impact within New Zealand’s Science and Innovation System.
What will be involved? The process will involve officials from the Ministry of Business, Innovation and Employment and Ministry of Health jointly conducting the refresh exercise. They will work closely with the HRC to collect information, and consult with the health research sector and end-users to develop their advice. Feedback will be sought from a range of stakeholders such as researchers and universities, district health boards, clinicians, medical
technology firms, Māori and Pacific stakeholders and other funding agencies. The timeframe for the refresh is over the next few months with ministers expecting to receive the findings in June.
Our expectations? We have been advised that the word ‘refresh’ has intentionally been chosen rather than ‘review’ or ‘restructure’. The process is aimed at enhancing our contribution, and the intent is that it will be an open and engaged process. We will be providing input into, and commenting on, the advice that will go forward and officials from the ministries will be keeping the HRC fully informed as the refresh progresses.
As the new Chief Executive of the HRC, I welcome the strategic refresh as a real opportunity to identify what the HRC does well, and be responsive to areas where we could do better. I look forward to hearing your views and feedback and receiving the synthesised findings of the review in due course. I am keen, as those of you
who have already met me know, to engage with you and the ministries on the best way for us to achieve our mission and our goals.
The HRC takes very seriously the need to demonstrate our ‘value add’ to New Zealand. To that end we have initiated a number of activities in the last year or so that will assist in producing data to meet the refresh objectives. For example, interim findings from our bibliometric survey provide evidence that HRC-funded research is more highly cited than other New Zealand health research. This is of course just one measure, but it does indicate the work produced is of the highest quality and utility to other researchers. There are many ways that New Zealand in 2015 is different because of the work the HRC has supported over the past 25 years. The refresh will inform how we do this as we move ahead to the next 25.
Dr Kathryn McPherson HRC Chief Executive

8
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Study identifies ways to make cycling safer on NZ roadsBy Suzy Botica
Cyclists in Auckland have a higher risk of being involved in a crash with a motor vehicle than cyclists from other parts of the country. This is despite – and possibly because of – the region having the lowest level of bicycle use relative to car use. Identifying factors that can help improve the conditions cyclists’ face and overcome barriers to active travel nationally was a key focus of the recently completed Taupo Bicycle Study.
In 2009, University of Auckland researcher Dr Sandar Tin Tin began a HRC-funded project to investigate the injury risks and cycling behaviour of a large group of cyclists recruited from the Taupo Cycle Challenge, New Zealand’s largest mass cycling event, in 2006. The 2590 cyclists who participated in this baseline Taupo Bicycle Study came from throughout New Zealand, although most were from the North Island.
With the support of her supervisors, Professors Shanthi Ameratunga and Alistair Woodward, Dr Tin Tin set about following up with participants from the baseline Taupo Bicycle Study, resurveying them through a web questionnaire. Participants’ data were then linked to data from four national databases, including police reports, the Accident Compensation Corporation (ACC) claims database, hospital discharges, and mortality records.
To date, 13 papers based on this exploratory research have been published in international peer-reviewed journals. One of the latest papers, published last year in the European Journal of Public Health1, examines the role of conspicuity (i.e. visibility) in preventing bicycle crashes involving a motor vehicle in New Zealand.
Dr Tin Tin says they found that aids designed to increase cyclists’ physical conspicuity – such as fluorescent clothing, lights, and reflective materials – were not sufficient to prevent bicycle crashes involving a motor vehicle, particularly in Auckland where bicycle use is low compared to car use. More important for cyclists’ safety on the road was the visibility of cyclists based on motor vehicle drivers’ interests and experience or ‘attention conspicuity’.
“We may be able to improve attention conspicuity by creating a more balanced transport mix,” says Dr Tin Tin. “The ‘safety in numbers’ effect suggests that if more people cycle and less drive, cyclists will be safer as drivers are more likely to pay attention to the presence of cyclists.”
Although Dr Tin Tin points out that the Auckland study participants had different cycle characteristics than those cyclists from other regions (e.g. the Auckland cyclists were less likely to cycle off-road, but more likely to cycle in the dark and in a bunch), she says these factors only explain half
of their higher crash risk. The other half is likely to be due to the car-dominated transport environment.
“Our findings suggest that New Zealand has been caught in a vicious circle in the past two decades, where a lower proportion of cyclists on the road decreases their conspicuity and poses them a higher crash risk, which in turn discourages bicycle use,” says Dr Tin Tin.
“Turning this vicious circle to a virtuous one requires cooperative and multidisciplinary efforts to promote cyclists’ safety and encourage cycling on New Zealand roads.”
Curiously, although cyclists may feel more visible, and hence safer, riding in a bunch, the study found that bunch riding may actually be associated with a higher crash risk.
“Our study couldn’t determine if the crash happened during bunch riding, just that those who engage in bunch riding are more likely to have had a crash. Perhaps this is because cyclists are more likely to take risks in a bunch and less likely to notice road hazards.”
The Taupo Bicycle Study project received funding worth over $600,000 in the HRC’s 2009 annual funding round. Dr Sandar Tin Tin has recently completed this five-year long project using participants’ data linked to four national databases.
Dr Sandar Tin Tin
9
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Other on-road injury risk factors identified included being over 35 years old, living in urban areas or in the Auckland region, using a road bike, and having had a history of a crash.
Over the study follow-up period, the Taupo Bicycle Study participants had 116 crashes that came to the attention of medical personnel or police per 1000 people per year, of which 66 occurred on the road and 10 involved a collision with a motor vehicle2. This correlates to 240 crashes and
38 collisions per million hours spent cycling on the road – similar to figures from Australia and the US, but much higher than European countries.
“Although the latest census shows that there has been a 16 per cent increase in bicycle commuting from 2006, bicycling still only makes up a small fraction of all trips in New Zealand. I hope that the outcomes from this study will help shape strategies to promote travel-related physical activity and improve road safety in
New Zealand,” says Dr Tin Tin.
Information: Dr Sandar Tin TinSchool of Population Health, the University of Auckland✆ +64 9 373 7999 ext 87034 [email protected]
Taupo Bicycle Study cyclistsOf the 2590 participants in the Taupo Bicycle Study, 35.5 per cent lived in Auckland, 20.6 per cent in Wellington, and 42.5 per cent in other regions.
On average, the participants cycled five hours a week on the road, of which 20 per cent involved riding in a bunch.
About 29.3 per cent reported always wearing fluorescent colours when cycling.
Of the 1731 participants who cycled in the dark, 83.8 per
cent always used functioning front lights, 89.9 per cent always used functioning back lights, and 49.1 per cent always used reflective materials.
The participants identified adverse weather and the danger of a car-dominated transport environment as the most important barriers to bicycle travel. More bike lanes and paths, better bicycle security in public places, and shower facilities at work would encourage them to cycle more often.
1 Tin Tin, S, Woodward, A, Ameratunga, S. (2014). The role of conspicuity in preventing bicycle crashes involving a motor vehicle. The European Journal of Public Health.
2 Tin Tin, S, Woodward, A, Ameratunga, S. (2013). Incidence, risk, and protective factors of bicycle crashes: Findings from a prospective cohort study in New Zealand. Preventive Medicine 57, 152–161.
PubMed Commons: A forum for scientific discoursePubMed Commons provides a forum for sharing information and perspectives about biomedical publications in the biomedical literature database, PubMed. This project was developed in response to interest from the scientific community and has been operating as an open pilot since December 2013.
PubMed Commons enables authors of PubMed-indexed publications to post relevant comments to any PubMed record. Anyone can view comments, which appear below abstracts. Comments are posted immediately but are regularly monitored for adherence to guidelines. They are contributed under a worldwide, royalty-free, non-exclusive, perpetual Creative Commons license that permits sharing and reuse.
The quality of the comments is high, but the use of the Commons is low. There are currently around 8,500
members, with over 2,700 comments live on publications. Moderation occurs after comments are made, and there is a computational approach to use ratings and other information to increase or decrease prominence. This infrastructure has been able to minimise the potentially harmful use of the forum to date.
There is a joining wizard with email addresses from PubMed authors to enable self-joining. The PubMed Commons team provides a personal alerting service to authors of articles receiving comments (about 10 per
cent respond to comments).
National Center for Biotechnology Information
U.S. National Library of Medicine, National Institutes of Health
Go to PubMed Commons at www.ncbi.nlm.nih.gov/pubmedcommons for more information.

10
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Harnessing wireless power for artificial heart pumpsBy Suzy Botica
Although artificial heart pumps have revolutionised the treatment of patients with heart failure, they do have one significant limitation: all of them currently have a bulky cable passing through the skin to power the pump, which is a major source of infection. In fact, about 60 per cent of people with heart pumps get a serious infection that requires hospitalisation.
In 2010, University of Auckland physiologist and bioengineer Professor Simon Malpas began a HRC-funded project designed to circumvent this problem by developing a way to wirelessly power artificial heart pumps. With the project now complete, we catch up with Professor Malpas to find out if he and his team at the university’s Auckland Bioengineering Institute have succeeded in their quest.
Q: What are some of the major challenges you’ve had to overcome to develop your system of wireless power for artificial heart pumps?
A: In industrial or commercial applications that use wireless power, such as your electric toothbrush, the alignment of the transmitter and receiver coils is known and fixed. However, it’s different for biological applications. We humans aren’t fixed; we have fat, muscle, and tissue, which makes us squishy – and we move.
We’ve developed a system of power transfer that allows for two things: firstly, it allows for the coil on the inside of the body and the coil on the outside of the body to move in relation to each other so that they align. Secondly, we’ve designed compact coils that can deliver up
to 10W of power without causing excessive heating. That’s really important because if you cause heating of about 40 to 43 degrees, this can result in long-term cellular damage to the patient.
Q: Does your system have a backup if something goes wrong?
A: Yes, our system includes a rechargeable backup battery that can supply 5W for about 30 minutes. This battery allows the patient to be tether free so that they can carry out activities such as showering without worrying about the power transfer system. The battery also ensures there’s constant power in case the system is accidently disengaged.
Q: How has this new technology that you’ve developed been received in the medical devices industry?
A: Our main target opportunity for this technology was artificial hearts, and there’s no doubt that remains the area with a pressing need. Everyone in the industry recognises the problem and sees that the solution is to have wireless power. The market for artificial hearts is not an area for the fainthearted though. Companies need a huge amount of capital for their development. We’re currently in discussions with two companies working in different areas about
the application of our technology, and we’re going to submit a funding application with them early this year. Any company we team up with has to be at the right phase of their development cycle – and these two are – so we’re hopeful successful partnerships will come about.
Q: Last year you were awarded a HRC grant of nearly $1.2 million to develop an implantable device to improve the management of patients with fluid on the brain (hydrocephalus). What’s the main problem you’re looking to solve here with the aid of wireless power?
A: Hydrocephalus is one of the most
Professor Simon Malpas was awarded over $1 million in the HRC 2010 annual funding round, for his project to develop wireless power for an implantable heart pump.
Expressions of Interest for Projects for the HRC’s 2016 funding round open on 15 June 2015. For more information go to www.hrc.govt.nz/funding-opportunities/researcher-initiated-proposals.
Professor Simon Malpas

11
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
common neurological disorders among children. It’s associated with increased pressure on the brain due to excess fluid and/or a failure to drain this fluid – and it’s fatal unless a shunt is inserted. While lifesaving, unfortunately 50 per cent of these shunts will fail within two years. Currently, there are no systems that enable you to monitor a shunt’s performance. If the pressure is going up in the skull and the shunt needs to be replaced or reprogrammed to allow for more or less flow out, there’s no means of assessing that.
The symptoms of early shunt failure are also often very similar to a simple headache or non-related infection, which necessitates many costly CT or MRI scans to resolve. We want to remove that stress, reduce cost and radiation exposure, and the likelihood of missing shunt malfunction by
developing a tiny implant that will allow clinicians to wirelessly monitor the intracranial pressure, brain temperature, and fluid flow of patients with water on the brain.
Q: How will this implant work?
A: We’re working on developing a very small implant that would be placed under the skull. A wand waved across the implant would then send intracranial pressure signals remotely to an external reader. One of the major parts of this grant is to develop pressure sensing capability and stability over a long period of time.
Q: What do you hope to achieve by the end of this HRC grant?
A: Our aim in this grant is to remain focused on developing and proving the technology, and then carrying out the first animal trials. If we can get through
all of those phases by the end of it then we’ll be in a good space to seek out private investment from venture capital funds or other sources for the next round of research required.
There are three classes of medical devices. Class three devices are for chronic conditions and include pacemakers and artificial hearts. Our implant would be a class 3 device, which means it will be subject to the most stringent evaluation and approval processes for safety and efficacy. I don’t know of anyone else in New Zealand who has designed and produced a class 3 medical device, so it would be unique if we can do it.
Information: Professor Simon MalpasThe University of Auckland✆ +64 9 923 6922 [email protected]
E-therapy for youth depression in primary care Depression is serious problem affecting more than 50,000 young New Zealanders each year. There are effective psychological therapies, such as cognitive behavioural therapy, but more than three-quarters of adolescents with depression never receive treatment.
A research team at the University of Auckland, led by Professor Sally Merry, have developed an effective e-therapy for young people to cope with feeling down, worried or stressed, called SPARX. SPARX takes the form of an innovative fantasy game that lets young people learn skills in a virtual world and apply them in real settings.
With funding from the HRC’s Research Partnerships for New Zealand Health Delivery initiative, Professor Merry, in partnership with Kapiti Youth Support, undertook a research project that expanded SPARX to an online format and created an e-monitor to link young people electronically with primary care clinicians who ‘prescribe’ SPARX, and who in turn could monitor young people’s progress.
The research showed that an online intervention can be delivered successfully within the context of a youth health service, with high levels of satisfaction reported by the young people who used the resource and with a significant improvement in symptoms of depression. It was identified that feedback can be provided directly to young people
using SPARX and that this can be delivered via an e-monitor and web-based dashboard to clinicians.
SPARX was officially launched at the University of Auckland by the Prime Minister on 28 April, 2014.
The findings from Professor Merry’s research have been used to support
In 2012, Professor Sally Merry was awarded nearly $200,000 for her project ‘E-monitoring and e-therapy for youth depression in primary care’. Funding was awarded through the HRC Research Partnerships for New Zealand Health Delivery initiative.
Professor Sally Merry
(Continued on page 13)
12
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Unique study to explore NZ’s ‘puzzling’ testicular cancer ratesBy Suzy Botica
In 2010 a paper published in the International Journal of Cancer showed that Māori have the highest rate of testicular cancer in New Zealand1. Intrigued by the paper’s findings, Dr Jason Gurney is embarking on a programme of research to find out why Māori are the only non-white population in the world to have the highest rates of this cancer.
Dr Gurney (Ngāpuhi, Ngati Hine) was awarded a 2014 HRC Eru Pōmare Research Fellowship in Māori Health to carry out his study of testicular cancer at the University of Otago, Wellington. His supervisor and mentor for this study is Associate Professor Diana Sarfati, lead author of the 2010 paper which first sparked his interest in testicular cancer.
“It was one of the first papers I read when I started working with Diana at the University of Otago, Wellington’s Department of Public Health. The paper showed that Māori have 50 per cent higher rates of testicular cancer than European New Zealanders. This is in stark contrast to other countries where European males suffer up to
five times the rates of testicular cancer compared to other ethnic groups. That’s what makes this New Zealand finding so puzzling,” says Dr Gurney.
Perhaps even more perplexing though was the finding that Pacific men in New Zealand have very low rates of testicular cancer. Māori men are about three times more likely to have testicular cancer than Pacific New Zealanders. Dr Gurney refers to this as the ‘Polynesian paradox’, where “two Polynesian populations residing in the same country experience a vastly different burden of disease”.
“This is one of the very rare occasions where Māori and Pacific peoples don’t move in parallel with respect to the incidence of a given cancer or
One of the HRC’s major Career Development Awards – the HRC Eru Pōmare Postdoctoral Fellowship – was awarded to Dr Jason Gurney last year. Dr Gurney will use his funding to research why Māori men have significantly higher rates of testicular cancer than non-Māori men. You can read about the other Māori Health Research Postdoctoral Fellowships that the HRC offers at www.hrc.govt.nz/funding-opportunities/maori-development.
Dr Jason Gurney and Associate Professor Diana Sarfati (Photo courtesy of the University of Otago, Wellington)

13
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
disease. It may well be the lynchpin in this whole mystery, because if we can explain why Māori have such high rates of testicular cancer and Pacific peoples such low rates, then we have a good chance of explaining what’s causing testicular cancer – and that would be ground-breaking.”
Dr Gurney’s fellowship will involve piloting the first case-control study of testicular cancer to be performed in New Zealand. It will also draw on his lead-authored paper published in The Journal of Urology2 which found that ethnic patterns of undescended testes, where the testes fail to reach the normal position in the scrotum, mirrored those observed for testicular cancer.
“Undescended testes is one of the few known risk factors for testicular cancer. We found that Māori had higher rates of undescended testes than all other ethnic groups, with Pacific and Asian groups having the lowest rates. Since the main risk factors for undescended testes occur in the womb, this suggests that the ethnic patterning of testicular cancer is at least partly due to prenatal risk factors.”
Dr Gurney and his research team are currently in the process of developing the design for the case-control study, which he says will require about 1000 participants. Maternal smoking, low birth weight and short gestational duration, as well as pre- and post-natal exposure to cannabis, are just a few of the potential risk factors
his group will be exploring. Study participants will also undergo blood tests to account for any possible genetic risk factors.
“It’s a bit like looking for a needle in a haystack, as there are so many exposures that have been linked to testicular cancer,” says Dr Gurney. “As soon as we can pinpoint which risk factors are more important than others, then we can start to look at prevention. We can’t prevent a disease if we don’t know what causes it.”
Dr Gurney says his HRC-funded fellowship – which will allow their group to pilot the case-control study, before seeking additional funding to complete it – is a unique opportunity to not only explain why Māori have the highest rates of testicular cancer in New Zealand, but also to help pinpoint what causes testicular cancer in general, something which has eluded the global research community to date.
“Ultimately, this is all about preventing testicular cancer. If we can point to certain things, like cannabis use, then that’s a highly modifiable risk factor. I want to explore every avenue that we can in terms of retrospective and prospective research.”
Although advances in treatment have led to very high survivorship among testicular cancer patients, Dr Gurney says that this high survival masks the impact of other significant outcomes.
“This is a disease with a very long
shadow, as it occurs in young men with a median age of about 35. A number of survivors will be left infertile or suffer some other sexual dysfunction after treatment. It’s an enormous quality of life issue not just for the young men, but also for their whānau.”
Information: Dr Jason GurneyUniversity of Otago, Wellington,✆ +64 4 918 6182 [email protected]
1 Sarfati D, Shaw S, Blakely T, Atkinson J, Stanley J. (2010) Ethnic and socioeconomic trends in testicular cancer incidence in New Zealand. International Journal of Cancer: 128, 1683–1691.
2 Gurney J, Sarfati D, Stanley J, Studd R. (2013) Do ethnic patterns of cryptorchidism reflect those found in testicular cancer? The Journal of Urology, Vol. 190, 1852–1857.
national implementation of SPARX through the Prime Minister’s Youth Mental Health Project, in collaboration with the National Institute of Health Innovation (NIHI) at the University of Auckland and the Ministry of Health. The research team are continuing to work with NIHI and the Ministry of Health to implement and monitor SPARX online, with the Ministry funding the ongoing
implementation and maintenance of SPARX.
SPARX is actively being promoted in many settings, including functions attended by general practitioners, school nurses, school guidance counsellors, psychiatrists and others. The implementation team at NIHI, with support from the research team, have ensured active engagement in
public meetings and community events designed to reach out to members of the public (parents, whānau, community organisations tasked with youth health), and are exploring ways in which social media can be used to maximise the reach to young people.
For more information, go to www.sparx.org.nz.
(Continued from page 11)
Subscribing to HRC NewsCurrent and past issues of HRC News can be viewed on the HRC website: www.hrc.govt.nz.
If you would like to subscribe to HRC News, please email: [email protected], and put ‘Subscribe HRC News’ in the header. Please include your name and postal address details. You can also use this email address to advise us if you no longer wish to receive HRC News.
14
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
‘Virus hunters’ make new discovery while studying unsolved gastro outbreaksBy Suzy Botica
Institute of Environmental Science and Research (ESR) scientist Dr Richard Hall has confirmed what is believed to be New Zealand’s first reported case of the sometimes nasty virus known as human parechovirus 3 (HPeV3).
The ESR team, dubbed the ‘virus hunters’, made the discovery as part of an HRC-funded study delving into unsolved outbreaks of human gastroenteritis (vomiting and diarrhoea).
Each year more than 25 per cent of gastro outbreaks in New Zealand go unsolved.
HPeV3 was first discovered in Japan in 2004, but up until very recently it has only been reported once in Bolivia. Last year it caused a significant outbreak of sepsis (infection of the
blood) in babies in Australia.
Dr Hall says the virus, which mainly infects babies and young children, may often cause no symptoms, but is also known to cause more severe diseases which can be fatal, including blood infections in newborn babies, acute inflammation of the brain, and even paralysis.
The faecal sample that tested positive for HPeV3 came from a 2-year-old child who was part of a gastro outbreak that occurred in a childcare
facility over the course of 17 days in 2012. It is not clear if it was the cause of the outbreak, but the Ministry of Health and the medical officer of health from the district health board where the patient resided were notified about the finding.
“The HPeV3 virus survives in the body for only a short time, maybe a few weeks, and is thought to be spread through the faecal-oral route. It can affect different tissue types in the body, such as the membranes surrounding the brain, but there’s still a lot that we don’t know about it.”
Dr Hall says the reason why the HPeV3 virus hasn’t been found in Australasia up until now isn’t because it’s uncommon. Instead, it’s because people haven’t thought to look for it before.
“Due to the serious illnesses associated with HPeV3 infection, we’d like to make clinicians and public health authorities aware of its presence, and suggest they consider
Dr Richard Hall received an Emerging Research First Grant worth $150,000 in the HRC’s 2011 annual funding round. These grants support emerging researchers who are seeking to establish independent careers in health research. For more details go to www.hrc.govt.nz/funding-opportunities/researcher-initiated-proposals.
Dr Richard Hall
(Continued on page 16)
15
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Rotavirus vaccine trial a successBy Mark Wright
A vaccine that can be safely given to newborns to protect them from rotavirus and the severe gastroenteritis it can cause, has come a step closer following a successful HRC-funded efficacy trial in Dunedin.
Although the new vaccine has been developed by the RV3 Rotavirus Vaccine Programme at the Murdoch Children’s Research Institute in Melbourne, it has strong links to the University of Otago, through the involvement of a former paediatrics senior lecturer, Professor Graeme Barnes, who moved to Melbourne in the 1970s and played a key role in rotavirus research.
University of Otago principal investigator Dr Pam Jackson says RV3 was developed from a strain of rotavirus – identified by Professor Barnes – where newborns that had it exhibited no symptoms. Babies who had it didn’t go on to get rotavirus later, so that apparent natural protection made the strain an ideal basis for a vaccine.
“Also, this strain has come from human newborns, as opposed to the other vaccines, which have come from cow or monkey rotavirus strains.”
To put its importance in perspective, Professor Barry Taylor, co-principal investigator and Dean of the Dunedin School of Medicine and Head of
Paediatrics and Child Health, says rotavirus kills an estimated 600,000 children every year, mainly in the third world.
“In New Zealand it would probably cause one or two deaths per year, but it does result in a lot of days in hospital.
“It is most dangerous in the first month or two. The other rotavirus immunisations that have been developed by commercial companies are actually given later and they don’t protect in that early period.”
Dr Jackson says one of the reasons Dunedin was chosen for the RV3 trial is that New Zealand had yet to add any of the other rotavirus vaccines to its schedule at that time.
“When you are developing vaccines you need to start by looking at efficacy and immunogenicity. What that means is you have to do a small study to see if the vaccine produces measurable protection in the child, and then you need to broaden it out to other areas.”
A larger scale efficacy study is also being done in Indonesia because previous studies have shown that while current vaccines have good efficacy in developed countries, in developing countries efficacy has been poor, even though that is where such vaccines are most needed.
Eventually it will be manufactured in Indonesia using proven oral vaccine production facilities used for the production of a vaccine for polio, which has been largely eradicated.
A robust randomised control trial used three different groups: one where they were given a placebo, and the second where they were given their first dose as an infant, at about
six weeks, then 16 and 24 weeks. Those in the third arm were given their first dose within the first five days of life, with follow-up doses at eight and 16 weeks.
“This was a world first. This is the first time that we’ve had an oral vaccine given to neonates,” explains Dr Jackson.
“Being able to give the vaccine early has a number of benefits. In developing countries, where there is the highest burden of rotavirus and the highest burden of deaths, many people may only see a birth attendant, or perhaps a midwife. If you can deliver an oral vaccine at that time when they are at greatest risk of death then you will prevent more deaths.”
Giving an oral vaccine early also negates the risk of intussusception, a complication seen with some rotavirus vaccines where the bowel telescopes into itself.
Dr Jackson says the trial results were better than expected with the vaccine providing a strong immune response in more than 90 per cent of those in both the newborn and infant group, which she describes as extraordinary figures. The vaccine was also well tolerated without any major problems or side effects.
A HRC International Investment Opportunity Fund grant worth over $450,000 was awarded to Professor Barry Taylor and his team in 2008 for their project looking at a human neonatal rotavirus vaccine for the global community.
Professor Barry Taylor
(Continued on page 16)

16
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
According to Professor Taylor, countries that have already brought in a rotavirus vaccine have had a 60 per cent reduction in hospital admissions for rotavirus after just one year.
One of the existing vaccines was introduced in New Zealand last year. However, it’s hoped that once this new oral vaccine is through its phase III trials that New Zealand will switch to using it, because it will be cheaper and will protect that first month to six weeks of life.
“The Government, through the HRC, have put some money into developing this, so there is a case for using it,” he says. “It might be another four or five years before it becomes a commercial product, but the aim is to produce it cheaply for third world countries.”
Both Professor Taylor and Dr Jackson are especially grateful for the support they have had from the Dunedin community, saying it takes an altruistic mother to allow a new vaccine to be trialed on her baby, especially when it involves three to four blood tests afterwards to see if it works.
“Dunedin families are remarkably altruistic and participate in research more than any other city in New Zealand,” says Professor Taylor. “It’s partly because the university has always been here and there is a reasonable amount of trust. We try and maintain that trust by ensuring things don’t go wrong and that people are treated well.”
Professor Taylor says the trial also had tremendous support from Emeritus Professor Don Roberton, Otago’s former Health Sciences Pro Vice Chancellor, who is an immunologist.
“We also had an excellent study coordinator in Amanda Muloch and some great nursing staff.”
The study is already spawning new lines of research, including Dr Mee-Yew Chen’s MD thesis on the vaccine and the role of maternal antibodies – the antibodies babies get from their mother – and whether they interfere with or even promote the oral vaccine.
“That research hasn’t been done before so it’s really exciting.”
Information: Dr Pamela JacksonDunedin School of Medicine, University of Otago✆ +64 3 474 0999 ext [email protected]
Professor Barry TaylorDunedin School of Medicine, University of Otago✆ +64 3 474 [email protected]
(Continued from page 15)
testing for HPeV3 as is carried out in the US, Japan, and Europe, and more recently in Australia, especially for rare cases of severe disease that can’t be explained,” says Dr Hall.
The development of any future diagnostic tests would be put together by ESR, the Ministry of Health, and DHB labs.
The study team used the latest high-throughput DNA sequencing technology offered by New Zealand Genomics Limited to test the anonymous faecal samples. The techniques used were able to capture any known virus listed in the GenBank database at the National Center for Biotechnology Information in the US. The list of DNA sequences generated was huge – enough to fill up
34,140 volumes of Pride and Prejudice.
In addition to HPeV3, the data analysis also revealed a spectrum of other viruses and parasites that may have caused the previously unsolved outbreaks. Two viruses were identified that are already known to cause such outbreaks – sapovirus and rotavirus. Dr Hall says these viruses must have escaped detection during routine laboratory testing. The new information collated from this study has been used to refine current laboratory testing methods, allowing for more outbreaks to be resolved.
“Viruses cause a huge percentage of the 4.5 million cases of vomiting and diarrhoea that happen in New Zealand every year. They are usually very contagious and can quickly be
passed on and affect a vast number of people. These viruses are like the $2 coins in your wallet: they are very common and change hands a lot. If you’ve had something like norovirus, you can be shedding viral particles for up to three weeks.”
The full results of this study have been published in the top international Journal of Clinical Microbiology1.
Information: Dr Richard HallInstitute of Environmental Scienceand Research (ESR)✆ +64 4 529 0605 [email protected]
1 Moore N E, Wang J, Hewitt J, Croucher D, Williamson D A, Paine S, Yen S, Greening G E, Hall R J (2015). Metagenomic analysis of viruses in feces from unsolved outbreaks of gastroenteritis in humans. Journal of Clinical Microbiology, 53:15–21.
(Continued from page 14)
About HRC NewsHRC News can be viewed on the HRC website: www.hrc.govt.nzEditor: Kristine ScherpWriters: Suzy Botica Mark WrightEmail: [email protected]: PO Box 5541, Wellesley Street Auckland, 1141, New ZealandPhone: (09) 303 5200Fax: (09) 377 9988Contributions are welcome. All articles in HRC News may be reprinted, provided the writer and the source are acknowledged.ISSN 1178-9565 (Print) ISSN 1178-9557 (Online)

17
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Shaping palliative care for MāoriBy Mark Wright
Research carried out as part of an HRC partnership project with the Ministry of Health has provided valuable information to develop more appropriate palliative care for Māori.
Lead researcher Dr Lesley Batten, from the Research Centre for Māori Health and Development at Massey University, says at the time the Request for Proposals was released they were already working on clinical issues around Māori end of life care with Arohanui Hospice in Palmerston North.
“When the Liverpool Care Pathway (LCP) – which was the gold standard end of life pathway for the last 24 to 48 hours of life – was introduced to New Zealand, Arohanui Hospice was one of the key organisations that introduced and evaluated it.”
Dr Batten says Māori have not been accessing hospice care in the same numbers as other groups, and they have been identified as a population with special needs in the New Zealand Palliative Care Strategy.
A multiphase study was launched, beginning with a stocktake of the LCP, to examine cultural goals and how those operated in practice.
The researchers also interviewed stakeholders to get their perspectives about cultural care.
Dr Maureen Holdaway, the Associate Director of the Research Centre at Massey, says they interviewed patients, whānau, Māori health providers, and community support people – including kaumatua, kuia, and health workers – to find out what
they felt Māori end of life care should involve.
“One of the key things to come out of this was that some of the issues whānau had around cultural understanding, communication, information and support services hadn’t improved greatly over a long period of time.
“But there were also some very good examples of how well some support services, especially aged care facilities, accommodated whānau and whānau needs. Simple things like being able to have co-care and sing waiata, and accommodating the family without them feeling like they were an imposition on staff,” she says.
“Other positive things included providing special foods and enabling whānau to be part of the process by doing some of the basic care and attending to cultural needs to ensure their whānau member had a good journey.
Dr Maureen Holdaway and Dr Lesley Batten (Photo courtesy of Massey University)
Dr Maureen Holdaway and her team were awarded $803,763 for a project, which commenced in March 2011, to research culturally appropriate end of life care for Māori. This project was a joint venture funded through the HRC’s Partnership Programme initiative, in conjunction with the Ministry of Health. For more information about the HRC’s Partnership Programme, go to www.hrc.govt.nz/about-us/PartnershipProgramme.
(Continued on page 19)
18
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
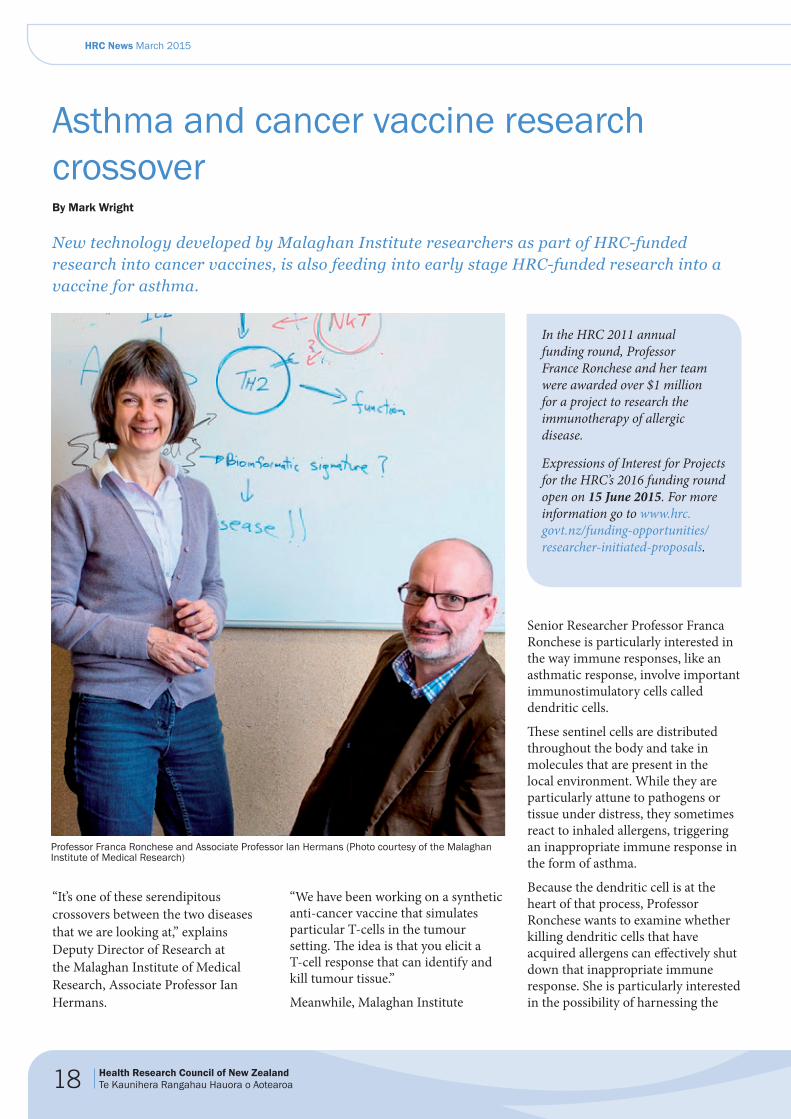
Asthma and cancer vaccine research crossoverBy Mark Wright
New technology developed by Malaghan Institute researchers as part of HRC-funded research into cancer vaccines, is also feeding into early stage HRC-funded research into a vaccine for asthma.
“It’s one of these serendipitous crossovers between the two diseases that we are looking at,” explains Deputy Director of Research at the Malaghan Institute of Medical Research, Associate Professor Ian Hermans.
“We have been working on a synthetic anti-cancer vaccine that simulates particular T-cells in the tumour setting. The idea is that you elicit a T-cell response that can identify and kill tumour tissue.”
Meanwhile, Malaghan Institute
Senior Researcher Professor Franca Ronchese is particularly interested in the way immune responses, like an asthmatic response, involve important immunostimulatory cells called dendritic cells.
These sentinel cells are distributed throughout the body and take in molecules that are present in the local environment. While they are particularly attune to pathogens or tissue under distress, they sometimes react to inhaled allergens, triggering an inappropriate immune response in the form of asthma.
Because the dendritic cell is at the heart of that process, Professor Ronchese wants to examine whether killing dendritic cells that have acquired allergens can effectively shut down that inappropriate immune response. She is particularly interested in the possibility of harnessing the
In the HRC 2011 annual funding round, Professor France Ronchese and her team were awarded over $1 million for a project to research the immunotherapy of allergic disease.
Expressions of Interest for Projects for the HRC’s 2016 funding round open on 15 June 2015. For more information go to www.hrc.govt.nz/funding-opportunities/researcher-initiated-proposals.
Professor Franca Ronchese and Associate Professor Ian Hermans (Photo courtesy of the Malaghan Institute of Medical Research)

19
HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
immune system to do the job.
Associate Professor Hermans says the vaccines they have been developing are designed to generate a particular phenotype of T-cell that has the ability to select cells and kill them.
“What we’ve done with our vaccine in asthma is to push their activity into killing anything that has acquired an allergen, so effectively these T-cells could kill dendritic cells.”
“That is where the two paths cross: around this ability to stimulate killer T-cells to a defined product. In this case, it’s an allergen, and in the case of a tumour, it’s to a tumour-associated protein.”
The vaccine design has already proved effective in an animal model of asthma, and is also looking very promising in cancer models.
One of the key components of the new vaccine technology is an adjuvant, which was developed in collaboration with synthetic chemist Dr Gavin
Painter from the Ferrier Research Institute at Victoria University of Wellington.
Associate Professor Hermans says the adjuvant is attached to the vaccine to strengthen the immune response. The aim is to generate a large population of T-cells which are specific to an allergen, if you want to treat asthma, or to a tumour protein, if you want to treat cancer.
“We’ve been focusing on a very unusual adjuvant that brings a third immune cell type called an NKT cell into the equation, which actually helps the killer T-cell response develop.”
These NKT cells recognise glycolipids rather than proteins, or peptide fragments from the proteins. The researchers chemically link glycolipids to the vaccine in such a way that the vaccine remains inactive until delivered to speciallised cells within the body that drive killer T-cell responses. The components are then separated by intracellular enzymes
and go their separate ways. They end up on the cell’s surface in the right orientation to stimulate NKT cells, and push the killer T-cells to divide.
In the case of the asthma vaccine, the aim is to encourage killer T-cells that are specific to the allergen to divide rapidly over the next few days, so that millions of cells can then circulate to the lungs and surrounding lymphoid tissues that drain from the lung, and kill off any dendritic cells involved in causing asthma.
The new vaccine technology also raises the possibility of looking at this model for other allergic diseases later down the track.
Information: Associate Professor Ian HermansMalaghan Institute of Medical Research✆ +64 4 903 3043 [email protected]
“Death and dying was just one stage in the journey. For whānau it was also important to have the time to think and talk about what was going to happen after, and for providers to accommodate some of the things that they wanted.”
Dr Batten says one of the key things to emerge from the findings of that part of the project was that cultural care wasn’t just about someone’s ethnicity. Rather, it was about all of the care being integrated so that there was respect for communication and coordinated care.
“It wasn’t a case of the hospice or health service taking over the cultural matters. If the health services had their work sorted, the whānau could get on and do their work – and the two of those together made culturally appropriate care.”
The third phase of the study was translational: taking what was learned from the first two phases and working with the providers to set up pilot projects.
One project involved providing specific education for undergraduate nurses, while another ran an intensive integrated toolkit programme in an aged residential care organisation. This included an audit and staff education and a number of other activities.
Another part of the study involved making changes to the LCP document that is being used in New Zealand to standardise things like ethnicity documentation to meet national standards. This included doing simple things like creating space for both a next of kin and a whānau spokesperson, and allowing for a tohunga or Māori spiritual advisor,
alongside religious support.
Dr Batten feels that they now have the framework for something that could be rolled out.
“This research was developed from the beginning as translational research. That meant there was always the expectation that the people in positions of influence in clinical situations would have something to work with at the end of it, and we have developed some clinical tools that could be used in clinical practice.”
Information: Dr Maureen HoldawayResearch Centre for Māori Health & DevelopmentMassey University✆ +64 9 414 0800 ext [email protected]
(Continued from page 17)

HRC News March 2015
Health Research Council of New ZealandTe Kaunihera Rangahau Hauora o Aotearoa
Right dose – right resultBy Mark Wright
“It’s about the right dose, of the right drug, for the right time, in the right patient, which leads to the right result.”
“It’s about the right dose, of the right drug, for the right time, in the right patient, which leads to the right result.”
It is a simple and succinct explanation, but Dr Paul Chin, from the University of Otago, Christchurch says it neatly sums up the aim of his pharmacology research undertaken after he was awarded the 2012 HRC Clinical Research Training Fellowship.
“The overall thrust was to work out better ways to dose patients with various medications. With all drugs you have to balance the risk of side effects against the potential benefits.”
During his two-year fellowship Dr Chin focused on two medications: the antibiotic gentamicin, which has been around for about 50 years, and a relatively new blood thinner called dabigatran.
Dr Chin says that although gentamicin is used widely, it has side effects such as deafness and kidney damage.
“Despite the potential for those complications, it has been a really good antibiotic and is still used today.”
Dabigatran, like the warfarin it replaces, can cause bleeding.
“It’s about trying to dose those things
better and try and find tools that prescribers can use to help with the dosing and ensure patients are not getting too much or too little.”
Both drugs are eliminated through the kidneys and while tools, such as kidney markers for measuring kidney function, are being refined all the time, they also need better equations to evaluate those measurements.
Dr Chin says he has investigated new equations that are better at working out what sort of dose the patient should be on – particularly in relation to gentamicin – so that the chances of kidney damage can be reduced.
They found dabigatran had some added levels of complexity in terms of what happens to it in the body.
“Even using the best equation for kidney function, the prescriber can really only account for about 40 per cent or so of the information they would need to get a good handle on what sort of dose the patient requires. There is still a large amount of variability to explain and I wanted to see if there was a better way of doing it.”
Dr Chin says they looked to blood markers, comparing those to clotting tests on blood samples, then successfully correlated those with dabigatran levels to work out what the levels should be.
“One of the original selling points of dabigatran is that you don’t have to subject the patient to regular blood tests; you can prescribe the pill and walk away. With warfarin, the medicine it is meant to replace, we usually do regular blood tests to see if the blood is thin enough or too thin.
“We’ve shown that about 20 per cent of patients using dabigatran are going
to have blood that is either too thick or too thin. Being able to identify those patients would be quite helpful in terms of trying to reduce their risks of clots or bleeds.”
Dr Chin says that having a test to measure dabigatran levels can tell you whether they are getting too much medication or whether there is some other medicine the patient is taking that is affecting it.
As a result, they have been able to provide an optimum range of levels for prescribers to target to avoid both over-treatment and under-treatment.
“The next step is to work out whether targeting those levels actually improves outcomes,” he says.
“In New Zealand we already have 15,000 patients on dabigatran, even though it is new, so it is an extremely important medicine for us to get a good handle on.”
Information: Dr Paul ChinDepartment of Clinical PharmacologyUniversity of Otago, Christchurch✆ +64 3 364 [email protected]
Dr Paul Chin
Dr Paul Chin was awarded a HRC Career Development Award – a Clinical Research Training Fellowship – worth over $150,000 in 2012.
Clinical Research Training Fellowships for the HRC’s 2016 funding round open on 4 June 2015. Go to www.hrc.govt.nz/funding-opportunities/career-development for more details.



























![ASA Trial Workshop Slides for Archives NZ [2016-09-28]](https://img.pdfslide.us/doc/110x75/5874d4231a28abd05f8b51bf/asa-trial-workshop-slides-for-archives-nz-2016-09-28.jpg)