Embed Size (px)
Citation preview
PsychologyBiological Rhythms and Sleep
RhythmsSleep stages
Theories
Shift work
Jet lag
Sleep
Disorders
Change
s
Types of rhythms:Circadian rhythms: • Occur once every 24 hours.• Many hormones (neurotransmitters, example:
cortisol) and other physiological processes show a similar circadian variation in activity.
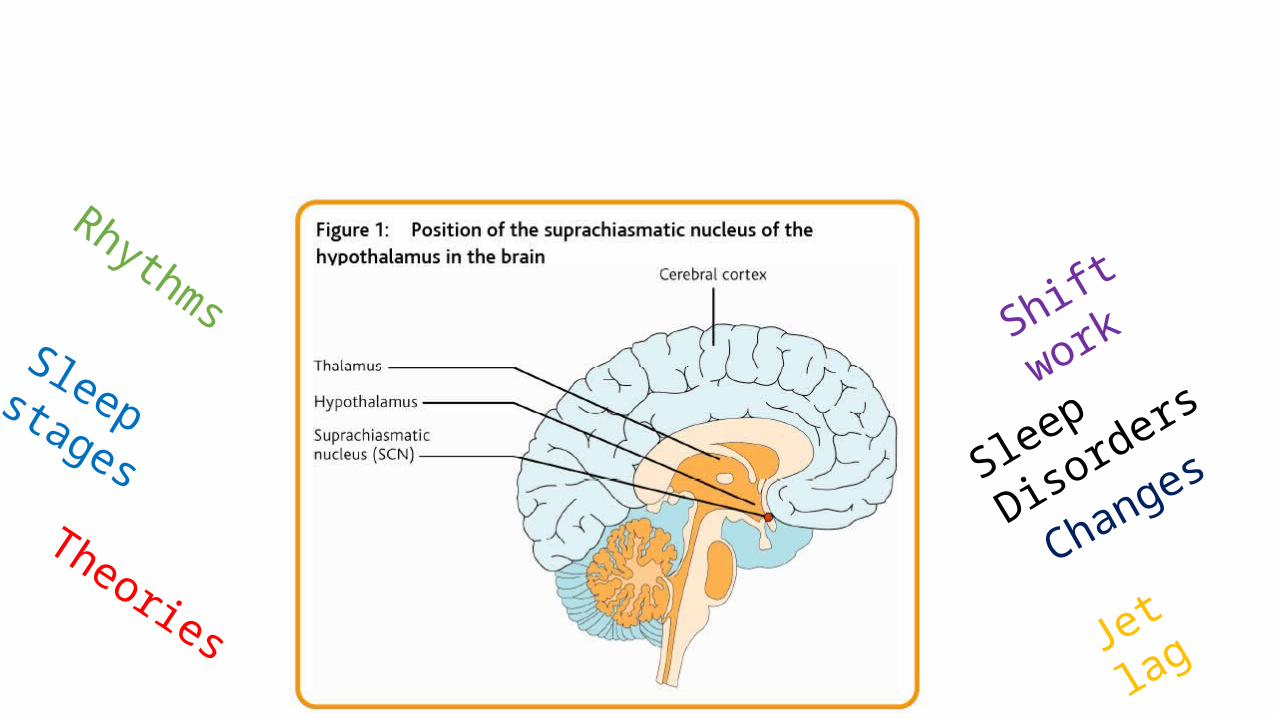
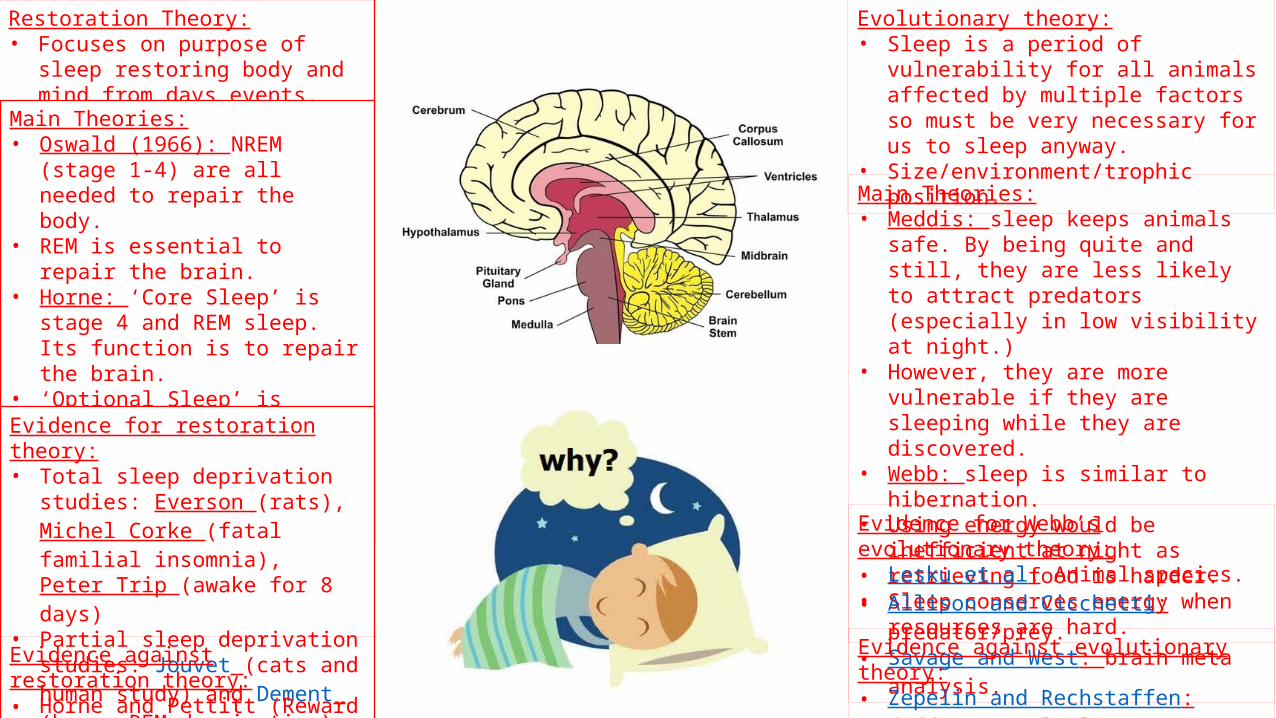
Examples:• Sleep/wake cycle (controlled by endogenous
pacemakers working as a body clock) with melatonin peaking at midnight to continue sleep according to light levels (darkest at 12)
• Body temperature (at its lowest at 4am, and highest in the afternoon. Also a dip after lunch (bigger dip if eaten but still occurs if not). Siestas relate to dip.))
• Cortisol is at its lowest around midnight and highest a 6am.
• Nocturnal animals sleep during the day, diurnal at night to provide energy when needed.
Key Studies:• Siffre (1972).• Folkard et al.
Infradian rhythms:• Occur less than once every 24
hours.Examples:• Menstrual cycle (every month)• Hibernation (for some animals
to conserve energy)• Migration.Key Studies:• Stephan and Zucker (1972).
Ultradian rhythms:• Occur more than once every
24 hours.Examples: • Eating cycle.• Sleep/wake stages.Key Studies:• Abraham, Gwinner and Van’t
Hof.• Binkley.
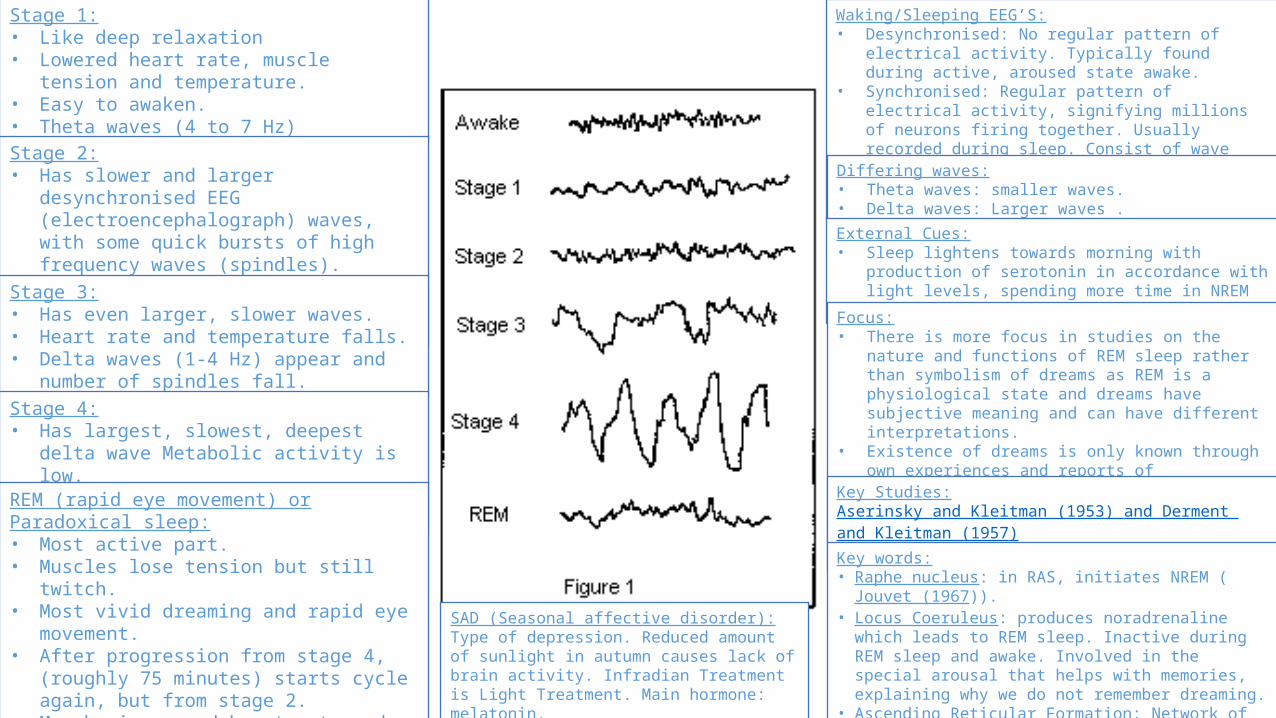
Sleep Stages:Stage 1:• Like deep relaxation• Lowered heart rate, muscle tension and
temperature.• Easy to awaken.• Theta waves (4 to 7 Hz)Stage 2:• Has slower and larger desynchronised EEG
(electroencephalograph) waves, with some quick bursts of high frequency waves (spindles).
• Theta waves dominant but periodic bursts of sleep spindles (12-16 Hz)
Stage 3:• Has even larger, slower waves.• Heart rate and temperature falls.• Delta waves (1-4 Hz) appear and number of
spindles fall.Stage 4:• Has largest, slowest, deepest delta wave
Metabolic activity is low.• Hard to wake as at this stage sleep is deepest.REM (rapid eye movement) or Paradoxical sleep:• Most active part.• Muscles lose tension but still twitch.• Most vivid dreaming and rapid eye movement.• After progression from stage 4, (roughly 75
minutes) starts cycle again, but from stage 2.• May be increased heart rate and blood pressure
(resulting in erections and an increase in vaginal flow) but difficult to awaken.
• Full cycle is around 90 minutes.
SAD (Seasonal affective disorder):Type of depression. Reduced amount of sunlight in autumn causes lack of brain activity. Infradian Treatment is Light Treatment. Main hormone: melatonin.
Waking/Sleeping EEG’S:• Desynchronised: No regular pattern of electrical activity.
Typically found during active, aroused state awake.• Synchronised: Regular pattern of electrical activity, signifying
millions of neurons firing together. Usually recorded during sleep. Consist of wave patterns of particular amplitude and frequency (Hz). Examples: deep sleep = one large wave per second.
Differing waves:• Theta waves: smaller waves.• Delta waves: Larger waves .
External Cues:• Sleep lightens towards morning with production of serotonin
in accordance with light levels, spending more time in NREM stages 2 and REM (easier to awaken)
Focus:• There is more focus in studies on the nature and functions of
REM sleep rather than symbolism of dreams as REM is a physiological state and dreams have subjective meaning and can have different interpretations.
• Existence of dreams is only known through own experiences and reports of participants.
• There is no objective method of measuring dreams unlike EEG’s for sleep waves.
Key Studies:Aserinsky and Kleitman (1953) and Derment and Kleitman (1957)Jouvet (1967)
Key words:• Raphe nucleus: in RAS, initiates NREM (Jouvet (1967)).• Locus Coeruleus: produces noradrenaline which leads to REM
sleep. Inactive during REM sleep and awake. Involved in the special arousal that helps with memories, explaining why we do not remember dreaming.
• Ascending Reticular Formation: Network of neurons. Controls brain arousal state.
Disrupting Rhythms:Jet Lag:• Rapid disruption of sleep rhythms. • Most frequently encountered.• Dislocation between body clock and local zeitgebers,
resulting in extreme tiredness, depression, slow mental/physical reactions.
Phases:• Phase delay: east to west.• Wants to sleep in early evening and wake in early hours.• Correctable by attempting to be alert/active when you
need to sleep.• Phase advance: west to east.• time is later than internal clock so have to advance o
catch up.• More difficult to correct.• Leads to tiredness, confusion and desynchronisation of
other rhythms (shown in Siffre’s study).Key Studies:• Recht, Lew and Schwartz.• Beaumont et al • Sack et al Reduce effects:• Sleep well before flight.• Avoid caffeine.• Try to adjust – sleep at correct times.• Go out in daylight ASAP.Factors effecting severity:• Direction of travel (phase delay/phase advance)• Number of time zones crossed.• Age.• Individual Differences (some people are phase tolerance.)
Shift Work:• Started in 19th century with the invention
of light bulbs – allowing unnatural distribution of external zeitgebers.
Concerns:• Performance affected.• Depression.• Fatigue.• Illness.Explanation:• Between 2-4am, body tried to sleep.• Also results in sleep deprivation
(prolonged exposure to little sleep) as try to stay up to have social life.
Key Studies:• Czeiser, Moore-Ede and Coleman• Gordon et al• Sack et al.Rotation types:• Forward shift rotation: Shift hours go
forward (Nights, mornings, days)• Backward shift rotation: traditional shift
work. Harder on participants.Shift lengths:• Multiple studies have found that longer
shift patterns (of around 21 days compared to traditional 7 days) and better on the worker, socially and biologically.
Theories for sleep:Restoration Theory:• Focuses on purpose of sleep restoring
body and mind from days events.
Main Theories:• Oswald (1966): NREM (stage 1-4) are
all needed to repair the body.• REM is essential to repair the brain.• Horne: ‘Core Sleep’ is stage 4 and
REM sleep. Its function is to repair the brain.
• ‘Optional Sleep’ is stages 1-3 and is not needed.
• Restoration of the body happens when we are awake and relaxed.
Evidence for restoration theory:• Total sleep deprivation studies:
Everson (rats), Michel Corke (fatal familial insomnia), Peter Trip (awake for 8 days)
• Partial sleep deprivation studies: Jouvet (cats and human study) and Dement (human REM deprivation)
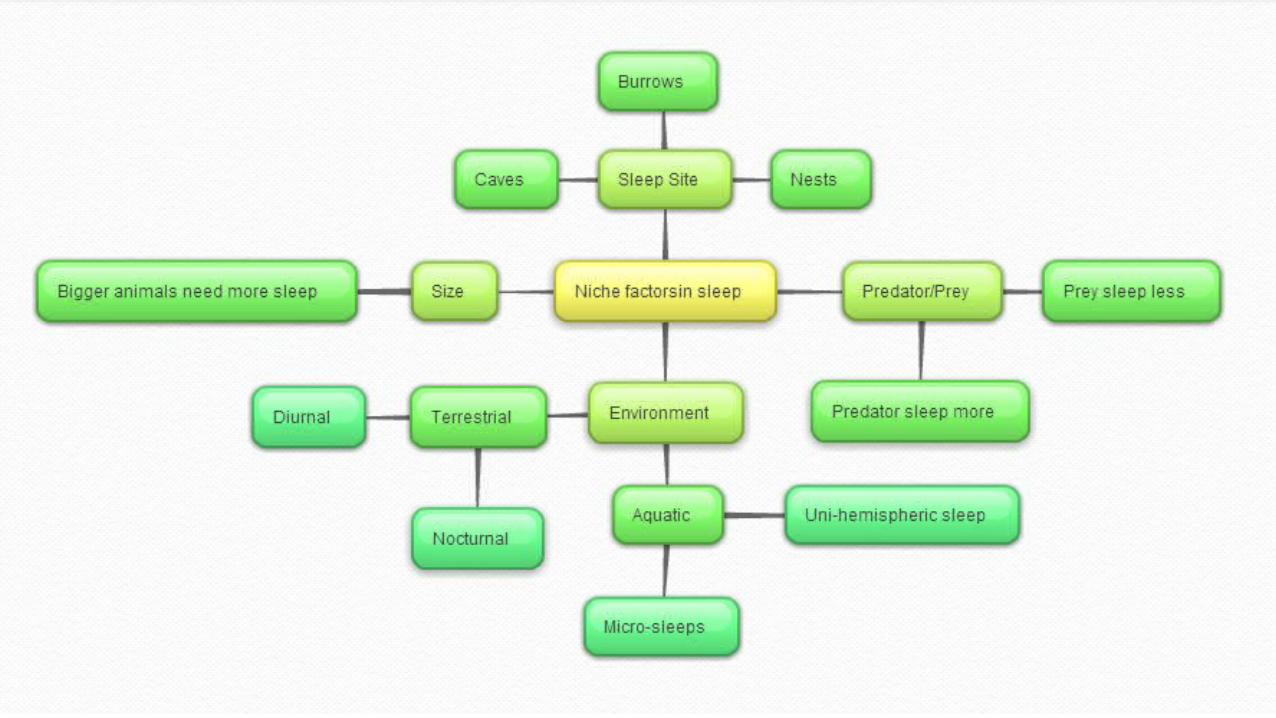
Evolutionary theory:• Sleep is a period of vulnerability for all
animals affected by multiple factors so must be very necessary for us to sleep anyway.
• Size/environment/trophic position.
Main Theories:• Meddis: sleep keeps animals safe. By being
quite and still, they are less likely to attract predators (especially in low visibility at night.)
• However, they are more vulnerable if they are sleeping while they are discovered.
• Webb: sleep is similar to hibernation.• Using energy would be inefficient at night
as retrieving food is harder.• Sleep conserves energy when resources are
hard.
Evidence against restoration theory:• Horne and Pettitt (Reward overcomes
deprivation to extent)
Evidence for Webb’s evolutionary theory:• Lesku et al: Animal species.• Allison and Cicchetti: predator/prey.• Savage and West: brain meta analysis.
Evidence against evolutionary theory:• Zepelin and Rechstaffen: different
calculators.
Changes in sleep:Newborns:• Sleep on average 16-18 hours a day.• In early months, an infant sleep is divided
equally between REM and NREM (different for premature babies).
• EEG of sleeping infant in REM sleep is highly similar to waking EEG.
• In REM, infants are restless, with arms and legs moving almost constantly (also happens before birth).
• Different sleep stages: entering REM sleep immediately after falling to sleep. Not until around 3 months that NREM and REM are established.
• Regular sleeping pattern is normally established around 20 weeks.
1-5:• Usually sleep about 13-14 hours.• Sleep stages occur ever 45-60 minutes.
5-10:• Sleep stages increase to around 70
minutes. (Borbely).• Between 5 and 12, nocturnal sleep drops
to around 9-10 hours.
10-12:• Experience ‘sleep-wake utopia’, studied
by Dement.
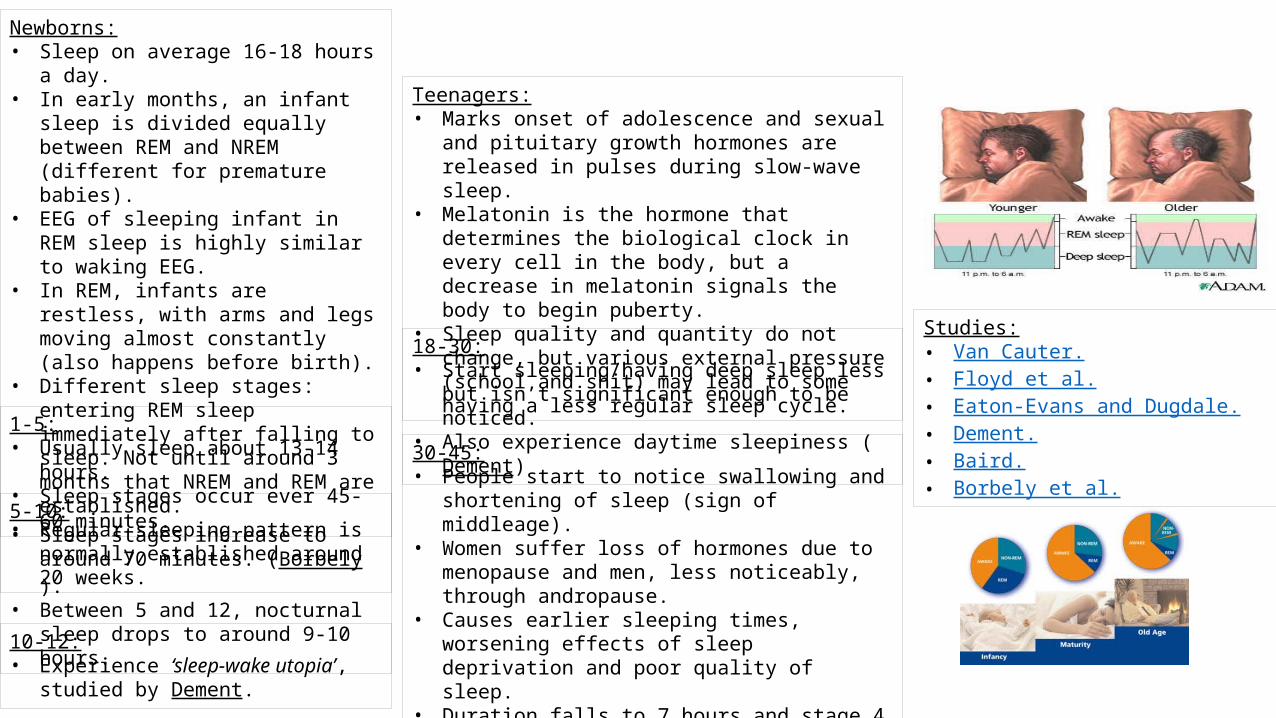
Teenagers:• Marks onset of adolescence and sexual and pituitary
growth hormones are released in pulses during slow-wave sleep.
• Melatonin is the hormone that determines the biological clock in every cell in the body, but a decrease in melatonin signals the body to begin puberty.
• Sleep quality and quantity do not change, but various external pressure (school and shit) may lead to some having a less regular sleep cycle.
18-30:• Start sleeping/having deep sleep less but isn’t
significant enough to be noticed.• Also experience daytime sleepiness (Dement)
30-45:• People start to notice swallowing and shortening of
sleep (sign of middleage).• Women suffer loss of hormones due to menopause and
men, less noticeably, through andropause.• Causes earlier sleeping times, worsening effects of
sleep deprivation and poor quality of sleep.• Duration falls to 7 hours and stage 4 all but disappears. • Age related effects on the prostrate mean sleep is
disturbed.
Studies:• Van Cauter.• Floyd et al.• Eaton-Evans and Dugdale.• Dement.• Baird.• Borbely et al.
Sleep Disorders:Dyssomnias:• Problems with
amount/quality/time of sleep.• Often produces daytime tiredness.• Including insomnia and narcolepsy.
Parasomnias:• Behavioural/psychological events
during sleep.• Rarely associated with daytime
tiredness.• Include sleep walking and
nightmares.
Insomnia:• Secondary insomnia: single, underlying medical,
psychiatric or environmental cause, meaning insomnia is a symptom for another, main disorder (depression/heart disease).
• Common for those who do shift work or have circadian rhythm disorders – result of environmental factors such as caffeine.
• Diagnosis: sleep onset latency of 30 minutes. Sleep efficiency of less than 85%. Increased number of night time awakening. Symptoms reoccur more than 3 times a week.
• Duration: transient insomnia (less than one week and often associated with something in particular. Short term – 1-4 week.) Chronic/clinical insomnia (more than one month. Has significant and distressing effect on daytime functioning due to tiredness ad irritability.)
Narcolepsy:• Mitler – ‘sleepiness one feels when trying to complete a boring
task at 3 a.m. after 72 hours of total sleep deprivation.’• Extreme tiredness in the day, many also have cataplexy (brief
and sudden loss of muscle tone with no loss of consciousness – range of severity, from mild weakness to collapses), disturbed sleep, sleep attacks, hypnogogic (sleep onset) and hypnopompic (sleep offset) hallucinations (vivid dream like experiences lasting seconds to 20 minutes but easily aroused by touch or noise) and sleep paralysis. These can occur immediately or after.
• Uncommon – affects between 0.03% and 0.18% of the population (Nishino et al)
• Occurs in late teens, early twenties in most but 25% only get symptoms at around 40 (Honda et al)
• Main symptom – sleep attack. Occur at times of physical inactivity/boredom and preceded with drowsiness. But can occur at any time with no warning.
• They are easily awoken, feel refreshed, with another attack unlikely for several hours.
• Most common trigger is sudden emotion – surprise, laughter or anger.
Neural explanation:• Hypocretin is believed to be a main factor.
Key Studies:• Broughton et al.• McMahon et al.• Scammell et al.• Arii et al.
Folkard et al:• Studied 12 participants, living in a cave for 3 weeks.• They agreed to go to bed when the clock read 11.45 and wake
at 7.45. • Gradually quickening the clock to a 22 hour day – circadian
rhythms continued running on a 24 hour cycle.• After experiment, it only took participants a short amount of
time to resynchronise (showing importance of external zeitgebers)
Conclusion:• Circadian rhythms can only be guided to a limited extent by
external cues.(Evaluation same a Siffre)
Peter Tripp:• NYC disc jockey, stayed awake for 8 days for charity. Suffered
delusions and hallucinations (desk on fire).
Stephan and Zucker:• Damaged SCN (superchiasmatic nucleus) of rats.• Influenced circadian rhythms. Examples:• Changed drinking patterns.• Running on wheel at differing times.Conclusion:• SCN is one of the key endogenous pacemakers. Strengths:• Zucker, Boshes and Darks squirrel study and
Rasak and Zuckers hamster study showed similar results.
• Laboratory based study (reliable and easy to determine cause and effect.)
Weaknesses:• High death rate (only 11/25 survived).• Lacks ecological validity, generalizability and
mundane realism as performed on rats.
Siffre:• Measured brain, heart, blood pressure and body temperature while in a cave for six months to
study the effect of external zeitgebers on circadian rhythms.• His days extended to 27 to 35 hours with no external zeitgebers.• Sleep and temperature remained normal.Conclusion:• Maintenance of normal circadian rhythms is dependent on external zeitgebers, resulting in free
running rhythms. Strengths:• Laboratory based (reliable)• Folkard et al study showed similar results• Abraham, Gwinner and Vant Hof, Injected sparrows with melatonin and made them sleep,
showing melatonin's importance in sleep.• Binkley: Injected melatonin into chickens. Found it lower at dawn, suggesting its role in sleep.Weaknesses:• Siffre appeared depressed in the cave but was offered no counselling/debriefing before, during
or after the study.• Case study – may not be generalizable.
Recht, Lew and Schwartz:• Studied American baseball teams (US has four
time zones.)• Teams travelling west to east before games won
37% of games.• Teams travelling east to west before games won
44% of games.Conclusion:• Teams suffering from phase advance suffered
from the effects of jet lag less and those teams with phase delay.
Strengths:• Over whole season – reliable• Sack et al found that the effects decrease with
age. • Beaumont et al found that melatonin sped up
resynchronisation by taking it at bedtime 3 days before and 5 days after travel.
Weaknesses:• May have just been differences in the teams
performance.
Czeiser, Moore-Ede and Coleman:• Changed rotation of shifts while measuring stress levels, health
and productivity to find which rotation is better.• Increased shift size from 7 days to 21 days.Conclusion:• Suggested forward shift rotation (phase delay) is better after
finding in a 9 month study on participants working phase delay type shifts had less stress, fewer sleep/health problems and increased productivity.
Strengths:• Gordon et al: Studies Philadelphia police on 18 day forward
shift rotation courses, finding 30% less sleeping on the job, 40% less accidents, better sleep and less stress than while on shorter, backward shift rotations.
• Ecologically/population valid.• Generalizable.• Phillips et al stated that no shit changes are better.• Sack et al found that planned napping reduces tiredness on
night shifts (Extreme Crabbers) Weaknesses:• Attrition (long study)• Could be other factors.• Coren studies rapid rotations, 2/3 day rotations, but had no
evidence and participants appeared depressed at lack of social life.
Aserinsky and Kleitman (1953) improved by Derment and Kleitman (1957):• Progression from stage 1-4 of NREM (none-REM) sleep is accompanied by physiological
changes :1) decreased in respiration, heart rate and blood pressure. 2) blood flow to brain slows, indicating reduced activity.
• Also found REM sleep is associated with dreaming by waking people at various stages. 80% of people awoken during REM sleep remembered dreaming while only 20% reported dreaming if awoken during NREM sleep.
Jouvet:• Lesioned raphe systems in cats and found
that this resulted in sleeplessness, concluding serotonin and raphe nucleus initiate sleep.
Everson:• 10 rats kept awake on disc (died). Lost weight,
ate more.
Michel Corke:• Really bad insomnia that kills.(appearing at
30 to 60). Showing that sleep is important.
Dement:• Students woken every time EEG showed they
were entering REM sleep. When stopped, they needed more REM sleep, which returned to normal after 5 days. Concluded REM is needed as more was required when prevented.
Horne and Pettitt:• 3 groups; 1) 72 hours without sleep with no
reward 2) 72 hours without sleep with incentive 3) normal sleep. All did auditory tasks – 2+3=same on first day, 2 worse on second but 1 worse throughout. (only 15 ppts. – 4th group)
Lesku et al:• 54 animal species, measured mass, brain mass, BMR, trophic position.
Allison and Cicchetti:• 39 species of predators and prey – prey have more
sleep – opposing Meddis.
Savage and West:• Meta analysis.• Focuses on brain size.• 96 species.
Zepelin and Rechstaffen:• May use different BMI calculators, resulting
in negative correlation.
Dement:• Pre-teens are bursting with energy in the day,
sleeping soundly at night and instantily wide awake come morning.
Dement:• 53% of 18-29 year olds suffer from daytime sleepiness as they need
as much sleep as teens but get less because of social pressures.
Van Cauter:• Examined several sleep studies involving male participants. • Sleep was found to decrease during two life periods: between the
ages of 16 to 25 and 35 to 50.
Floyd et at:• Reviewed almost 400 sleep studies, finding that REM sleep
decreased by about 0.6% a decade. • Proportion of REM sleep increases from about age 70, though this
may be due to overall sleep duration declining.
Eaton-Evans and Dugdale:• Found that the number of sleep periods for a baby decreases until
about 6 months, then increases until 9 months of age, before slowly decreasing again.
• May be from teething problems.
Dement:• Reported that over 40% of a group of healthy men and women aged
65 to 88 had some form of sleep apnoea. The majority being frequent ‘micro-arousals’, which are unremembered brief awakening lasting 3 or less seconds, occurring between 200 and 100 times a night.
Baird et al:• Found that infants aged 6-12 months with an increased risk of
waking between midnight and 6a.m. had mothers who had experience depressive symptoms prior to becoming pregnant.
• Night waking in the first year of child's life is associated with sleep disruption at 3 and later behaviour problems and learning difficulties, demonstrating the importance of early sleeping patterns and the mental health of woman prior to conception.
Borbely:• Questioned adults aged 65-83 on their sleeping habits, finding that
60% of them reported taking frequently daily naps.• Sleep in the elderly is more interrupted, but they continue to need
the same amount of sleep as they did in early adulthood, hence the need for naps.
Broughton et al:• 80% of a sample of narcolepsy sufferers had fallen asleep during
work more than once.
McMahon:• Compared to a sample of 2406 non-sufferers, narcolepsy sufferers
reported more family problems (21%), social isolation (35%), and physical/emotional health impairments (25%).
Scammell:• Reported on 23 year old who got narcolepsy after damaged to his
hypothalamus after a stroke. • He tested his cerebrospinal fluid showed reduced amount of
Hypocretin
Arii at al:• Reported that case of someone who showed signs of narcolepsy as
a result of a tumor.