Embed Size (px)
Citation preview

2015/8/28 B.S. Andersson
Timing of Allogeneic sCT for
Hodgkin’s Lymphoma
Borje S. Andersson, MD, Ph.D.
Molecular Pharmacology and Translat.
Drug Development Program,
Department of Stem Cell Transplantation
UT MD Anderson Cancer Center
August 28, 2015.

Gemcitibine+Busulfan+MelphalanImprove Survival in Refractory
Hodgkin’s Lymphoma
Carmustine (BiCNU)EtoposideCytarabine (Ara-C)Melphalan

-3 -2 -1-4-6 -5 +14 +21 +100 >1800
Graft
RIC ?
Conditioning
Supportive Care
GVHD prophylaxis and therapy
Patient
(age, gender, CMV,
comorbidities…)
1
2
35
6
4
Malignant
Disease
Features
Optimize Therapy to Improve outcome?

Myeloablative allo-SCT in HL
0
10
20
30
40
50
60
70
Early TRM (%) Total TRM (%) PFS (%) OS (%) PD (%)
IBMTR
JHOC
FHCRC

Hodgkin Lymphoma: current issues in allogeneic stem cell
transplantation (allo-SCT)
• Reduced-intensity conditioning (RIC) now widely
used. No consensus on “optimal” regimen.
• Transplant-related mortality (TRM) low but disease
progression (PD) major problem. Patient outcome
negatively affected.
• Recognition of prognostic value of complete
response (CR) pretransplant.
• Availability of brentuximab vedotin and optimization
of its use.

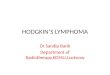
G-FM140: treatment schema
G8: Gemcitabine 800 mg/m2; ADM: Hospital admission;
F= Fludarabine 33 mg/m2; M = Melphalan 70 mg/m2;
T= Thymoglobulin 2 mg/kg (MUDs/MM);
SCT: stem cell transplant; GVHD prophylaxis: tacrolimus – miniMTX.
DAYS
-7 -1 -6 -5 -4 -3 -2 0
F F F F
M M SCTRest
TT
ADMG

Patient CharacteristicsTotal
N=27
Age a 31 (20-46)
Gender 15 M / 12 F
Prior chemotherapy regimensa 4 (2-10)
Prior autologous SCTb, n (%) 19 (70%)
Donor type
Matched related
Matched unrelated
16 (60%)
11 (40%)
Response status at allo-SCT, n (%)
CR/CRu 17 (63%)
PR 9 (33%)
Other 1 (4%)
TTP after autologous SCT (mo) 5 (1-68)
a Median (range). SCT: stem cell transplant; TTP: time to progression. CR/CRu:
complete response/undetermined. PR: partial response.

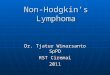
Brentuximab Vedotin (BV)
• SGN-35 antibody-drug conjugate
– CD30-targeted antibody (cAC10) conjugated to an auristatin (MMAE), an anti-tubulin agent
• Selectively induces apoptosis in
HL and ALCL cells:
– Binds to CD30
– Becomes internalized
– Releases MMAE
SGN-35 Antibody-Drug
Conjugate
SGN-35
binds
CD30
Endocytosis
ADC traffics to
lysosome
Enzymatic
linker cleavage
releases MMAE
from ADC
MMAE binds
tubulin
G2/M cell
cycle arrest
& apoptosis
CD30
SGN-35 Antibody-Drug
Conjugate
SGN-35
binds
CD30
Endocytosis
ADC traffics to
lysosome
Enzymatic
linker cleavage
releases MMAE
from ADC
MMAE binds
tubulin
G2/M cell
cycle arrest
& apoptosis
CD30
BV was granted accelerated approval by the FDA in Aug 2011 Courtesy of Dr. A. Younes

PFS by Best Response (by PET/CT) - HL
Time (months)
% P
atie
nts
Fre
e of
PD
or
Dea
th

Brentuximab (BV)-treated vs BV-
näive: Complete Response (CR) rates
• The seven patients who received BV as last line of tx prior to allo-SCT are a/w in
CR/CRu
BV-treated
n=14
n (%)
BV-näive
n=13
n (%)
Total
N=27
p value
CR rate pre-allo SCT 11/14 (79%) 6/13 (46%) 0.12 (Fisher’s)
CR-rate post-allo SCT 12/14 (85%) 11/13 (85%) ns

Patient outcomes
• Six deaths, three early ones (< day 100).
• Causes of death: PD n=2, graft rejection n=1,
pneumonia n=2, respiratory failure n=1.
• 21 patients alive.
• TRM (day 100/overall): 15%.
• Acute GVHD (grade II-IV): 19% (95% CI 9-42).
• Chronic GVHD: 39% (95% CI 24-65).
• Median follow up: 18 months (4-55).
PD: progressive disease. TRM: Transplant-related mortality

Overall survival (OS)
and progression-free survival (PFS)
0 10 20 30 40 50 60
Months Post Transplant
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Cum
ulat
ive
Prop
ortio
n Su
rviv
ing
OS
PFS
69%
55%
N= 27

Disease progression (PD)
Median time to PD: 13 months (2-22)
0 3 6 9 12 15 18 21 24
Months Post Transplant
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Cum
ula
tive In
cid
ence o
f Dis
ease P
rogre
ssio
n
30% (95% CI 15-61)

FM140 vs G-FM140 comparison
a Haematologica 2008; 93:257
b Study group included patients (n=28) with < PR
Variable
FM140a
n=58
n (%)
G-FM140
n=27
n (%)
Age (yrs) 32 (19-59) 31 (20-46)
Brentuximab vedotin pre-SCT (Y/N) 0 / 58 14 / 13
CR/CRu pretransplant 24%b 63%
TRM (day 100/overall) 7% / 15% 15% / 15%
OS (2-year) 64% 78%
PFS (2-year) 32% 55%
PD (2-year) 55% 30%
Time to PD after allo-SCT (mo) 4.5 (1-35) 13 (2-22)

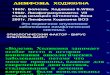
Progression-Free Survival after RIC Matched Sib SCT
Hodgkins lymphoma, N. America
- by disease status -
CR
ResistantPR
n = 87

Summary
• Even in the face of refractory relapse or relapse after
a previous auto-SCT, allo-SCT may yield long-term
disease control in Hodgkin’s Lymphoma.
• The outcomes with RIC-conditioning is becoming
the preferred choice.
• The relatively high TRM-risk suggests that auto-SCT
should still be the preferred initial choice for most
patients with recurrent HL