Embed Size (px)
Citation preview

A brief review by :
Dr. Mohammad Baghaei
Pharmacist and cosmetic scientist
Adult Atopic Dermatitis

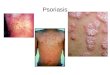
Atopic dermatitis (AD) is a chronic, pruritic inflammatory skin
disease of unknown origin that usually starts in early infancy, but
also affects a substantial number of adults.
AD is commonly associated with elevated levels of
immunoglobulin E (IgE) . That it is the first disease to present in
a series of allergic diseases — including food allergy, asthma,
and allergic rhinitis, in order—has given rise to the “atopic
march” theory, which suggests that AD is part of a progression
that may lead to subsequent allergic disease at other epithelial
barrier surfaces .
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Adult Atopic Dermatitis

Signs and symptoms
Primary physical findings include the following:
• Xerosis
• Lichenification
• Eczematous lesions
The eczematous changes and its morphology are
seen in different locations, depending on the age of
the patient (ie, infant, child, or adult).
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Signs and symptoms The following is a constellation of symptoms and features
commonly seen in AD:
• Pruritus
• Early age of onset
• Chronic and relapsing course
• IgE reactivity
• Peripheral eosinophilia
• Staphylococcus aureus superinfection
• Personal history of asthma or hay fever or a history of atopic
diseases in a first-degree relative
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Diagnosis
Essential features (must be present) are as follows:
• Pruritus
• Eczema (acute, subacute, chronic): (1) Typical morphology and
age-specific patterns (facial/neck/extensor involvement in children,
flexural involvement in any age group, sparing the groin and
axillary regions); (2) chronic or relapsing history
Important features (supports the diagnosis) are as follows:
• Early age of onset
• Atopy: (1) Personal and/or family history; (2) IgE reactivity
• Xerosis
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Associated features(nonspecific but suggest the
diagnosis of AD) are as follows:
• Atypical vascular responses (eg, facial pallor,
delayed blanch response)
• Keratosis pilaris/pityriasis alba/hyperlinear
palms/ichthyosis
• Ocular/periorbital changes
• Other regional findings (eg, perioral
changes/periauricular lesions)
• Perifollicular accentuation/lichenification/prurigo
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Exclusionary conditions (conditions that should be
excluded) are as follows:
• Scabies
• Seborrheic dermatitis
• Contact dermatitis
• Ichthyoses
• Cutaneous T-cell lymphoma
• Psoriasis
• Photosensitivity dermatoses
• Immune deficiency diseases
• Erythroderma of other causes
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Additional considerations in the diagnosis
of AD are as follows:
• No reliable biomarker exists for the diagnosis of AD
• Laboratory testing is seldom necessary but a complete blood cell count can be useful to exclude immune deficiency; an IgE level can be helpful to confirm an atopic pattern; a swab of skin can be helpful to identify S aureussuperinfection
• Allergy and radioallergosorbent testing is of little value
• Biopsy shows an acute, subacute, or chronic spongiotic dermatitis pattern that is nonspecific but can be helpful to rule out other conditions (eg, cutaneous T-cell lymphoma)
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Differential Diagnoses
• Allergic Contact Dermatitis
• Immunodeficiency
• Irritant Contact Dermatitis
• Lichen Simplex Chronicus
• Mollusca contagiosa with dermatitis
• Mycosis fungoides
• Nummular Dermatitis
• Plaque Psoriasis
• Relative zinc deficiency
• Scabies
• Seborrheic Dermatitis
• Tinea Corporis
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Treatment is important because it can:
Prevent the AD from getting worse.
Calm the skin, relieving pain and itch.
Reduce emotional stress.
Prevent infections.
Stop the skin from thickening. Thickened skin
often itches all the time — even when the AD is
not flaring.
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Management
Medicine and other therapies will be prescribed as
needed to:
Control itching.
Reduce skin inflammation (redness and swelling).
Clear infection.
Loosen and remove scaly lesions.
Reduce new lesions from forming.
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Management
Agents typically used to treat AD include the following:
• Moisturizers: Petrolatum, Aquaphor, or newer agents such as
Atopiclair and Mimyx
• Topical steroids (current mainstay of treatment; commonly used in
conjunction with moisturizers): Hydrocortisone, triamcinolone, or
betamethasone; ointment bases are generally preferred,
particularly in dry environments
• Immunomodulators: Tacrolimus and pimecrolimus (calcineurin
inhibitors; generally considered second-line therapy)
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Management
Other treatments that have been tried include the following:
• Ultraviolet (UV)-A, UV-B, a combination of both, psoralen plus UV-A
(PUVA), or UV-B1 (narrow-band UV-B) therapy
• In severe disease, methotrexate, azathioprine, cyclosporine, and
mycophenolate mofetil
• Everolimus
• Probiotics
• Antibiotics for clinical infection caused by S aureus or flares of disease
• Intranasal mupirocin ointment and diluted bleach (sodium hypochlorite)
baths
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist

Nonmedical measures that may be
helpful include the following:
• Using soft clothing (eg, cotton) next to the skin; wool
products should be avoided
• Maintaining mild temperatures, particularly at night
• Using a humidifier (cool mist) in both winter and
summer
• Washing clothes in a mild detergent, with no bleach or
fabric softener
• Avoiding specific foods as appropriate if there is
concomitant food allergy
Dr. Mohammad Baghaei
Pharmacist and cosmetic
scientist