Embed Size (px)
DESCRIPTION
munir suwalem
Citation preview

SCROTAL SWELLING AND PAIN IN CHILDREN
Presented by Dr munir suwalem S.H.O Peadiatric surgery
B.M.C Benghazi - libya

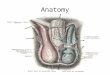
The Scrotum is a cutaneous pouch which contains the testes and parts of the spermatic cords. It is divided on its surface into two lateral portions by a ridge or raphé,
which is continued forward to the under surface of the penis, and backward, along the middle line of the perineum to the anus
the scrotum consists of two layers ,the outer layer is integument and the inner layer is dartos tunic, which divides the scrotal pouch into two cavities for the testes,

Vessels and Nerves.— The arteries supplying the coverings of the
testes are: the superficial and deep external pudendal branches of the femoral, the superficial perineal branch of the internal pudendal, and the cremasteric branch from the inferior epigastric. The veins follow the course of the corresponding arteries.
The lymphatics end in the inguinal lymph glands.
The nerves are the ilioinguinal and lumboinguinal branches of the lumbar plexus, the two superficial perineal branches of the internal pudendal nerve, and the pudendal branch of the posterior femoral cutaneous nerve.

The function of the scrotum appears to be to keep the temperature of the testes slightly lower than that of the rest of the body.
the temperature should be one or two degrees Celsius below body temperature (around 37 degrees Celsius or 99 degrees Fahrenheit);
higher temperatures may be damaging to sperm count.

CLASSIFICATIONscrotal swelling is usually classified as:
Painful or painless
Acute or chronic

Acute scrotal swelling with pain
Torsion of spermatic cord Torsion of appendix testis Acute epididymitis-orchitis Trauma Insect bite Thrombosis of spermatic vein Fat necrosis inguinal Hernia(incarcerated) Folliculitis Henoch-Schönlein purpura

Scrotal swelling without pain
Tumor Idiopathic scrotal edema Hydrocele Inguinal Hernia Henoch-Schönlein purpura

Chronic scrotal swelling
Hydrocele Inguinal Hernia Varicocele Spermatocele Sebaceous cyst Tumor


EPIDEMIOLOGYPrevalence
Inguinal hernias and hydroceles are the most common causes of scrotal swelling.
Testicular torsion occurs in 1:4000 boys.
Varicoceles are present in 15% of male adolescents and adults.

EPIDEMIOLOGYAge Hernias can occur at any age but are more
common in premature infants. Testicular torsion most commonly occurs
between the ages of 12 and 18 years. Idiopathic scrotal edema affects children < 14
years. Acute inflammation of the epididymis or testis,
including mumps orchitis, can occur at any age but is uncommon before adolescence.
Varicoceles are usually asymptomatic and are usually detected between 10 and 15 years of age.

MECHANISMAcute scrotal swelling with pain Torsion of the testicle
Twisting of the spermatic cord, with resulting compromise of the blood supply to the testis
Torsion of the appendix testisWhen the appendix testis torses,
inflammation and swelling of the testis and epididymis ensue, causing testicular pain and scrotal erythema.


MECHANISM Acute epididymitis-orchitis usually after
UTI Results from an anomaly of the urinary tract, either congenital or acquired:
Renal duplications and posterior urethral valves are among the more common anomalies.
With intermittent catheterization, the condition can occur from retrograde passage of bacteria back from ejaculatory ducts at the level of the prostate to the testis and epididymis.

MECHANISM Henoch-Schönlein purpura
Systemic vasculitis that can cause abdominal and joint pain , May involve the scrotal wall in a minority of cases
Trauma A similar appearance can follow a difficult
breech deliverySevere blunt trauma affecting the scrotal
contents Scrotal skin disease
Insect bites, folliculitis, and allergic dermatitis may cause erythema and edema of the scrotal wall.

MECHANISMScrotal swelling without pain Hernias and hydroceles
Most are caused by persistent patency of the processus vaginalis
Layers of the processus vaginalis condense late in gestation or early postnatally.
Obliteration of the processus vaginalis only around the testis leads to an indirect inguinal hernia with protrusion of fluid (or other contents) through the internal ring to the end of the pouch and potentially to the scrotum.

MECHANISM
Communicating hydrocele occurs when fluid travels through a processus vaginalis into the tunica vaginalis around the testis.
Scrotal hydrocele occurs after complete obliteration proximally with patency distally.
Hydroceles of the cord occur when the processus vaginalis obliterates proximally and distally, leaving a patent area in the midportion with retained fluid.

MECHANISM Varicoceles
A predilection for the left side exists, reflecting anatomy of the left gonadal vein entering the left renal vein at a right angle.
The right gonadal vein enters the vena cava directly at an angle, precluding reflux of venous blood.

HISTORYAcute scrotal swelling with pain Torsion of the testicle
Acute onset of constant, severe scrotal pain aggravated by physical activity
Nausea and vomiting may occur.Possible history of incidental antecedent
scrotal trauma, but pain usually occurs during rest or sleep
Neonatal testicular torsion Can exhibit at delivery as a nontender hard scrotal mass

HISTORY Torsion of the appendix testis
Onset of pain and swelling is commonly acute but can be progressive, usually occurring during rest.
Pain can be severe, but nausea and vomiting are less common than with testicular torsion.
Acute epididymitis-orchitisHistory can reveal acute or more protracted
onset of pain.The patient may have fever or dysuria or
pyuriaEpididymal inflammation may arise after
scrotal trauma.

HISTORY
Henoch-Schönlein purpuraOnset may be insidious or acute,
producing a variable degree of erythema and edema.
In more severe cases, the process may involve the testis and epididymis, mimicking testicular torsion.
Focal fat necrosisCan exhibit with scrotal pain and
swelling, usually after trauma in an obese boy

HISTORY
TraumaHistory (eg, injury from zipper entrapment
of scrotal skin) can be definitive.
Mumps orchitisRarely occurs in isolation; pain and swelling
usually occur within a week after parotitis.
Scrotal skin diseaseHistory may be of limited utility.

HISTORYScrotal swelling without pain Inguinal hernias and hydroceles
HerniaSwelling expands with increases in intraabdominal pressure (eg, crying, bowel movements, coughing).
The parent or child often reports the swelling to be smallest in the morning and largest late in the day.

HISTORY Hydrocele Whether the hydrocele is acute
or whether the scrotum has been chronically enlarged is often unclear.
The patient may have a history of trauma to the scrotum that stimulates production of serous fluid.
When the scrotum changes size during the day, suspect a communicating hydrocele.

HISTORY Tumors
Usually present as a hard, painless mass (or vague heavy feeling) in the testicle detected by the child, parent, or examining physician
Spermatoceles and epididymal cystsPainless and round, they usually remain stable
in size but can sometimes enlarge.

PHYSICAL EXAMAcute scrotal swelling with pain Torsion of the testicle
Scrotal erythemaSwelling of the involved hemiscrotumHigher-than-normal position of the testis within the
scrotumPalpation may show a horizontal rather than normal
vertical orientation of the testicle.Evaluation of the cremasteric reflex should begin on
the contralateral side; palpate the apparently unaffected testis to confirm normal size and position.Unilateral loss of the cremasteric reflex on the side of the swelling and pain highly correlates with the presence of torsion.

PHYSICAL EXAM The testis should then be palpated.
Despite the pain this maneuver may cause, it helps differentiate torsion from epididymitis.
Actual point of torsion of the spermatic cord can sometimes be palpated.
Associated hydrocele may be palpated and confirmed by transillumination.

PHYSICAL EXAM torsion of the appendix testis May demonstrate
hemiscrotal erythema and swelling A blue-dot sign, if the necrotic appendage
visible through the scrotal skin, can help make the diagnosis.
A normal cremasteric reflex is present bilaterally, and the testis is normally positioned within the scrotum.
Testicular discomfort, if present, is typically mild, but point tenderness may be elicited from uppermost pole of the testis near the head of the epididymis.

PHYSICAL EXAM Acute epididymitis-orchitis Scrotal
erythema and swelling are present, along with an intact cremasteric reflex.
Palpation during early phase of the inflammatory process demonstrates tenderness limited to the epididymis.
In the later phase, tenderness and inflammation include both epididymis and testis, and the distinction between the 2 structures may be difficult to appreciate.
The Prehn sign (relief of pain with testicular elevation) may be positive.

PHYSICAL EXAM Trauma
Examination must include both hemiscrotums and surrounding structures (penis, perineum), assessing for swelling, ecchymosis, and bleeding.
Tenderness may be limited to testis or epididymis, depending on extent of trauma.
Mumps orchitisTender testis
Scrotal skin diseaseRedness and edema limited to scrotum, with
normal testicle and spermatic cord

PHYSICAL EXAMScrotal swelling without pain Inguinal hernias and hydroceles
Feel for the testis first and keep it in mind during the rest of the examination.
Avoid confusing testis with contents of an incarcerated hernia.

PHYSICAL EXAMHernia
A bulge in the inguinal region with fluid that can be gently reduced back into the abdomen is diagnostic of an inguinal hernia.
In the cooperative child who can increase his intraabdominal pressure, this procedure may be repeatedly shown, particularly with the child standing.
Presence of thickened spermatic cord or silk-stocking sign (the feel of the layers of the processus vaginalis being rubbed against each other) suggests patency of the processus vaginalis or a hernia.

PHYSICAL EXAM Hydrocele When fluid is limited to the
testis and spermatic cord can be palpated above the fluid, a hydrocele is present.
Hydrocele of the spermatic cord feels distinct from the testis and is round or ovoid, possibly mimicking the presence of an additional testis.
Hydroceles (communicating, scrotal, or of the cord) are rarely associated with tenderness on palpation

PHYSICAL EXAM
TumorsOn palpation, mass is harder than the
substance of the testis, but this distinction may be difficult to discern.
Mass may bulge from surface of the testis.
Spermatoceles and epididymal cystsSeparate from the testis and can be
transilluminated


Diagnosis
Suggestive features on history
Suggestive features on examination
Torsion of the testis
Sudden onset testicular pain and
swelling; occasionally nausea, vomiting.
Note: pain may be in the iliac fossa
Discolouration of scrotum; exquisitely
tender testis, riding high
Torsion of
(hydatid of
Morgagni)
More gradual onset of testicular pain
Focal tenderness at upper pole of testis;
"blue dot" sign – necrotic appendix seen through
scrotal skin
Epididymoorchitis
Onset may be insidious; fever,
vomiting, urinary symptoms; rare in pre-pubertal boys, unless underlying
genitourinary anomaly, when
associated with UTI.
Red, tender, swollen hemiscrotum;
tenderness most marked posteriolateral to testis. Pyuria may be present.

Incarcerated
inguinal hernia
History of intermittent
inguinoscrotal bulge, with associated irritability
Firm, tender, irreducible,
inguinoscrotal swelling
Idiopathic scrotal oedema
Swelling noted but child not distressed
Bland violaceous oedema of
scrotum, extending into perineum + penis; testes not
tenderHydrocel
eSwollen
hemiscrotum in well, settled baby
Soft, non-tender swelling adjacent
to testis; transilluminates
brightly.

Henoch Schonlein
purpura
Painful scrotal oedema, with
purpuric rash over scrotum. May have
associated vasculitic rash of buttocks and
lower limbs, arthritis, abdominal
pain with GI bleeding, and
nephritis
may be difficult to distinguish from
testicular torsion in absence of other
features
Testicular or
epididymis rupture
Scrotal trauma eg. straddle injury,
bicycle handlebars, sports injury.
Delayed onset of scrotal pain and
swelling.
Tender swollen testis. Bruising, oedema,
haematoma, or haematocele may be
present.


LABORATORY EVALUATION
Urinalysis may help distinguish orchitis from torsion of the spermatic cord or testicular appendage when leukocytes or nitrites are present.
Acute scrotal swelling with painTorsion of the testicle
Urinalysis is unremarkable.Although the leukocytes count may be mildly elevated, it is not discriminating.

LABORATORY EVALUATIONAcute epididymitis-orchitis
Urinalysis may prove positive for leukocytes and nitrite but is often unremarkable among adolescents.
The leukocyte count is usually elevated

LABORATORY EVALUATIONScrotal swelling without pain Inguinal hernias and hydroceles
Laboratory tests are useful only for incarcerated inguinal hernias, with an elevated leukocyte count and possible acidosis.
TumorsPreoperative tumor markers (α-
fetoprotein, β-human chorionic gonadotropin) should be measured and used for postoperative monitoring.

IMAGINGAcute scrotal swelling with pain
Torsion of the testicleImaging by Doppler ultrasonography
or nuclear scintigraphy should be done if the diagnosis of testicular torsion is in question.
Perform imaging only when it will not delay surgical exploration if torsion exists, adding to the risk of testicular loss.

IMAGING Torsion of the appendix testis
If an inflammatory process resulting from torsion of the appendage makes differentiation from true spermatic cord torsion impossible, imaging may be helpful.
Scrotal Doppler ultrasonography or nuclear scintigraphy will show normal or increased flow to ipsilateral testis.

IMAGING Acute epididymitis-orchitis Ultrasonography and nuclear
scintigraphy show normal symmetric blood flow or increased blood flow to an enlarged epididymis or testis.
Voiding cystourethrography has been a routine part of the evaluation, but its yield is low with a normal ultrasound and a sterile urine.

IMAGING
TraumaScrotal ultrasonography can document
the integrity of the testis and of the tunica albuginea and the adequacy of blood flow.

IMAGINGScrotal swelling without pain Ultrasonography can determine cystic
or solid nature of a tense scrotal mass (eg, hydrocele, tumor) or spermaticoInguinal hernias and hydrocelesUltrasonography can delineate
scrotal contents, especially when a large or tense hydrocele limits physical examination of mass (eg, hydrocele of the cord, paratesticular tumor).

IMAGING Tumors
Scrotal ultrasonography is used to delineate the mass.
VaricocelesTesticular size, most accurately
assessed by ultrasonography, should be measured; significant loss of testicular volume is an indication for surgery.

TREATMENTAcute scrotal swelling with pain
Torsion of the testicleSurgical intervention is indicated not
only when testicular torsion is strongly suspected, but also in equivocal cases when torsion cannot be convincingly excluded.
The likelihood of salvaging the testis is highest when surgery is done shortly after onset of pain.

TREATMENTWith surgery, first explore the affected
testis, and, when torsion is present, detorse the cord.
Explore the contralateral testis (will have the same defect in anatomy) and fix it in place to avert a future torsion.
If the testis can be saved, fix it in the scrotum.

TREATMENT Torsion of appendix testis Management
is nonsurgical. The patient should rest and use
nonsteroidal pain relievers and cold compresses for several days to reduce inflammation, swelling, and pain.
Surgical intervention is indicated only when acute testicular torsion cannot be excluded.In these cases, the infarcted
appendage is removed at surgical exploration.

TREATMENT Acute epididymitis-orchitis Treat with
antibiotics based on the results of the urine culture and sensitivities.
Anti inflammatory agents, scrotal elevation, and rest should be prescribed.

TREATMENT Trauma
Testicular or spermatic cord contusions: Manage symptomatically.
Testicular rupture requires surgical exploration, evacuation of the hematoma, debridement, and repair (when possible).
Mumps orchitisTreatment is symptomatic.

TREATMENTScrotal swelling without pain Inguinal hernias and hydroceles
Repair on diagnosis to prevent incarceration , Perform surgery inguinally; isolate the sac from the cord structures and ligate it at the level of the internal ring.
Inspect the contralateral ring using diagnostic laparoscopy through the isolated ipsilateral sac.If the internal ring is open, proceed with contralateral surgical correction.
If the hydrocele is painful, then surgery should proceed sooner.

TREATMENT Tumors Perform radical orchidectomy
through an inguinal approach. If the mass is not suspicious for cancer, a
possible approach is to enucleate the mass and proceed with orchidectomy only if the frozen section is positive.
Spermatoceles and epididymal cysts Management typically is observation.
Surgery may be indicated when pain or significant enlargement is present.

PROGNOSISAcute scrotal swelling with pain Torsion of the testicle
Spermatogenesis may be compromised after 4–6 hours of ischemia.
Testicular salvage is time dependent, with universal loss of the testis after 24 hours of torsion.
Neonatal testicular torsionNeonatal testicular torsion can exhibit at delivery
as a nontender hard scrotal mass.Salvage in these cases is rare.
.

PROGNOSIS
Mumps orchitisInfertility may occur when the condition
results in atrophy of both testicles.Scrotal swelling without pain hydroceles
Most hydroceles resolve spontaneously by 1 year and should be repaired if they persist beyond this age.

Thank you for attention









![cdigital.dgb.uanl.mxcdigital.dgb.uanl.mx/la/1030000589/1030000589_041.pdf · Ch3P. XL.] INGUINO-SCROTAL TUMOURS. 521 If the swelling appeared suddenly at the groin, and extended into](https://img.pdfslide.us/doc/110x75/600ba6974c30cf209970b2dd/ch3p-xl-inguino-scrotal-tumours-521-if-the-swelling-appeared-suddenly-at-the.jpg)