Embed Size (px)
Citation preview

61 Chest Wall Lesions on Computed Tomography and Magnetic Resonance Imaging

CLINICAL IMAGAGINGAN ATLAS OF DIFFERENTIAL DAIGNOSIS
EISENBERG
DR. Muhammad Bin Zulfiqar PGR-FCPS III SIMS/SHL
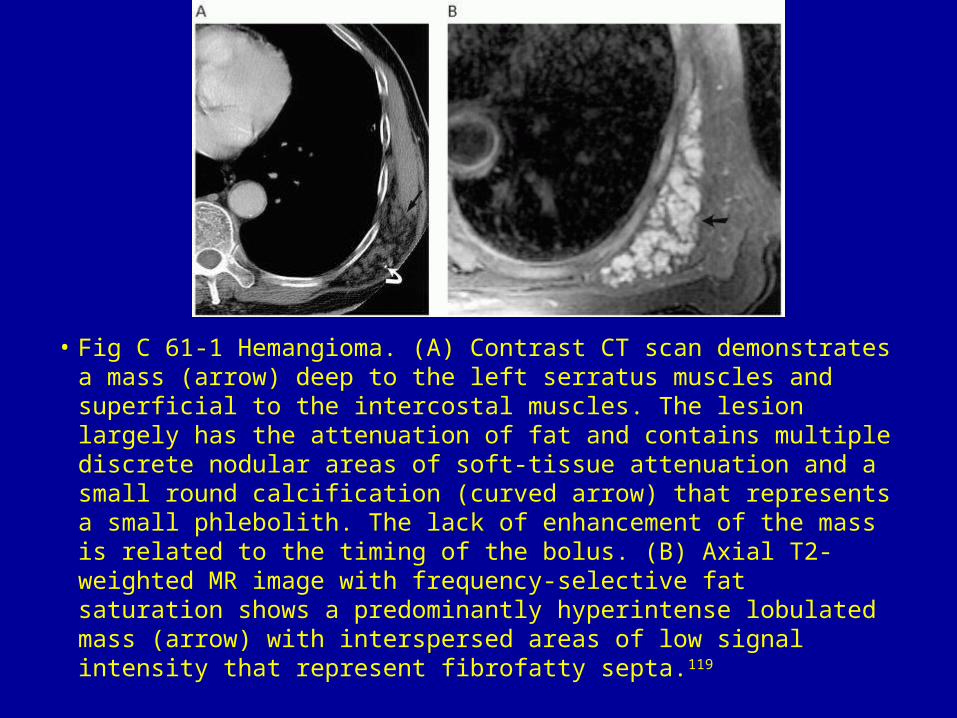
• Fig C 61-1 Hemangioma. (A) Contrast CT scan demonstrates a mass (arrow) deep to the left serratus muscles and superficial to the intercostal muscles. The lesion largely has the attenuation of fat and contains multiple discrete nodular areas of soft-tissue attenuation and a small round calcification (curved arrow) that represents a small phlebolith. The lack of enhancement of the mass is related to the timing of the bolus. (B) Axial T2-weighted MR image with frequency-selective fat saturation shows a predominantly hyperintense lobulated mass (arrow) with interspersed areas of low signal intensity that represent fibrofatty septa.119
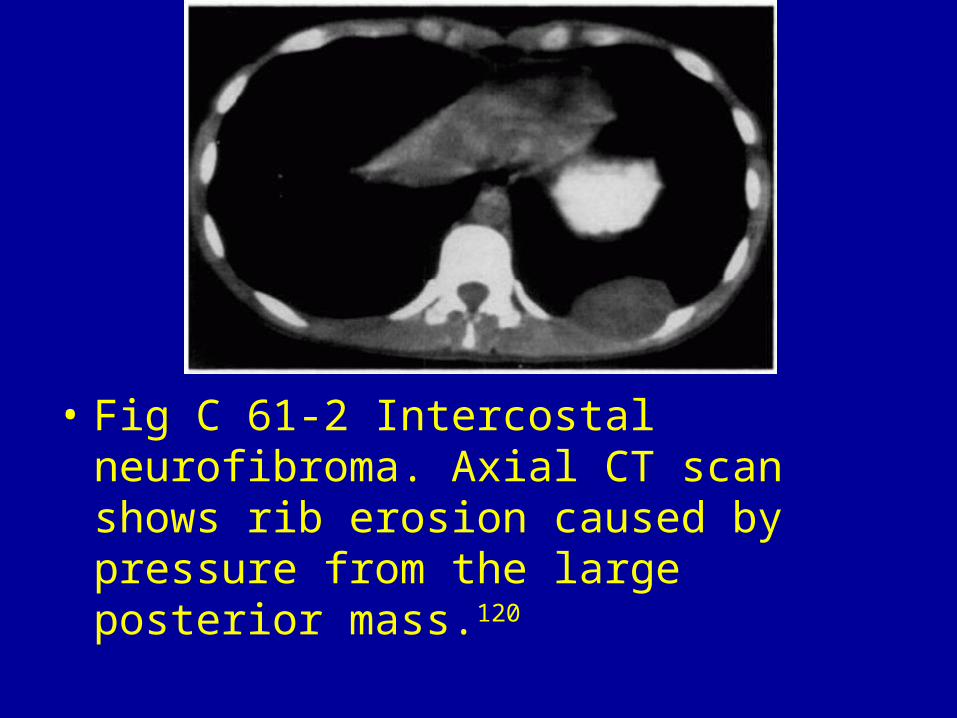
• Fig C 61-2 Intercostal neurofibroma. Axial CT scan shows rib erosion caused by pressure from the large posterior mass.120

• Fig C 61-3 Osteochondroma. CT scan shows a sessile mass with cortical and medullary continuity projecting into the lung. Note the calcification is the cartilaginous cap of the mass.121
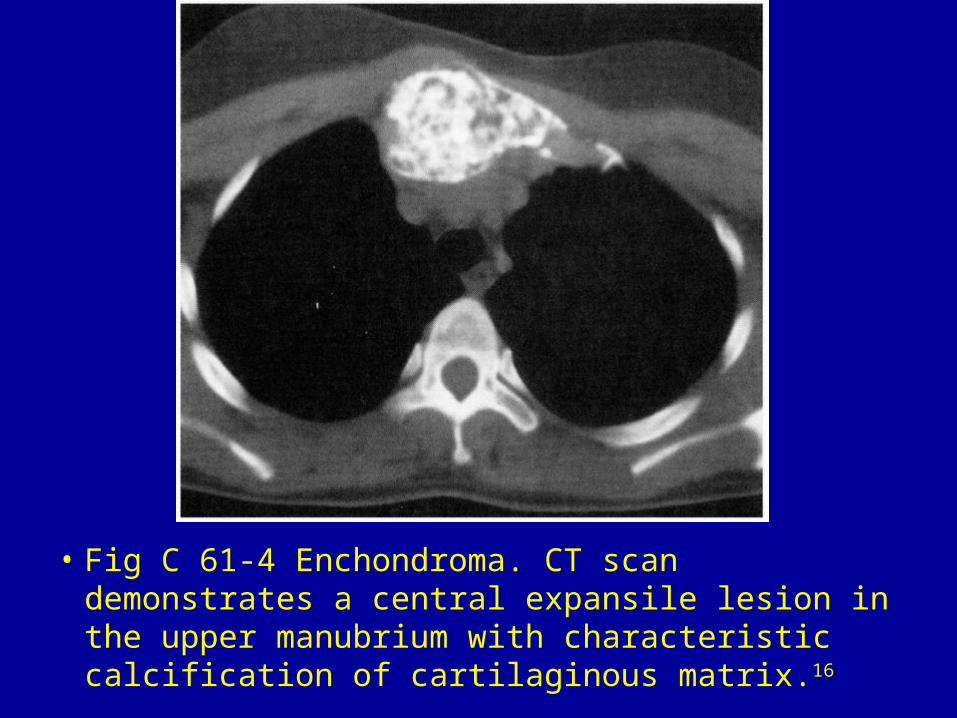
• Fig C 61-4 Enchondroma. CT scan demonstrates a central expansile lesion in the upper manubrium with characteristic calcification of cartilaginous matrix.16

• Fig C 61-5 Fibrous dysplasia. CT scan shows fusiform expansion of multiple ribs.120
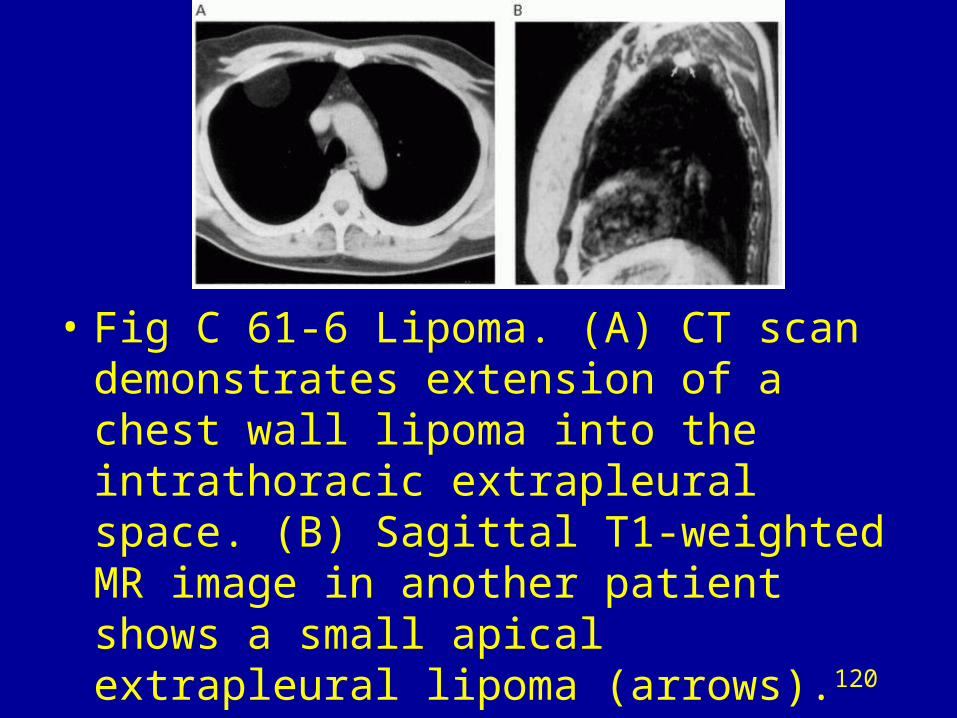
• Fig C 61-6 Lipoma. (A) CT scan demonstrates extension of a chest wall lipoma into the intrathoracic extrapleural space. (B) Sagittal T1-weighted MR image in another patient shows a small apical extrapleural lipoma (arrows).120
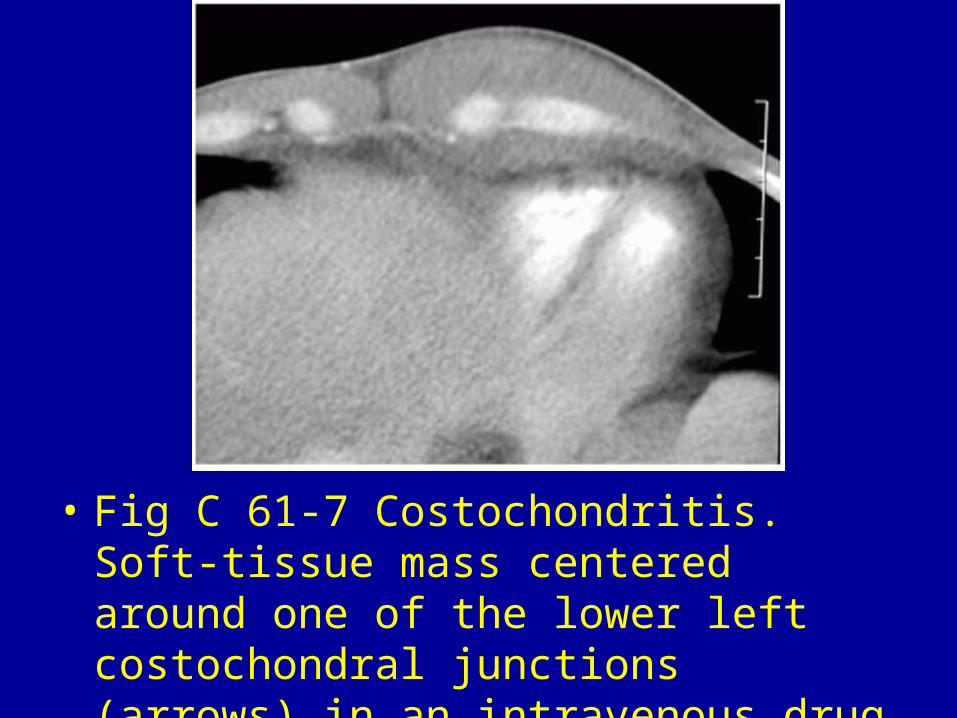
• Fig C 61-7 Costochondritis. Soft-tissue mass centered around one of the lower left costochondral junctions (arrows) in an intravenous drug abuser.10
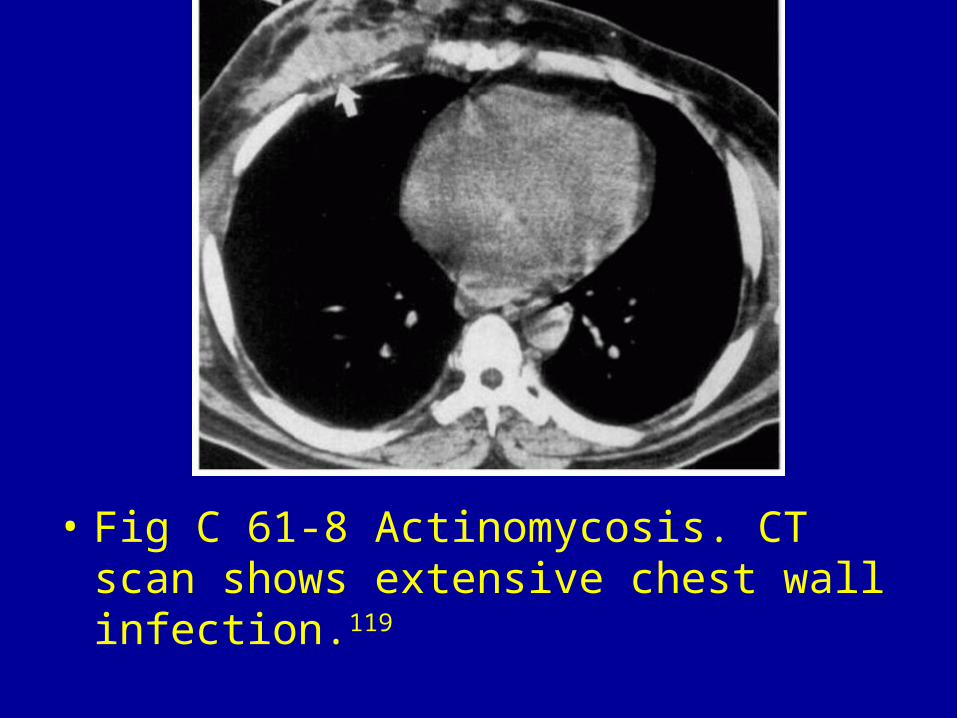
• Fig C 61-8 Actinomycosis. CT scan shows extensive chest wall infection.119
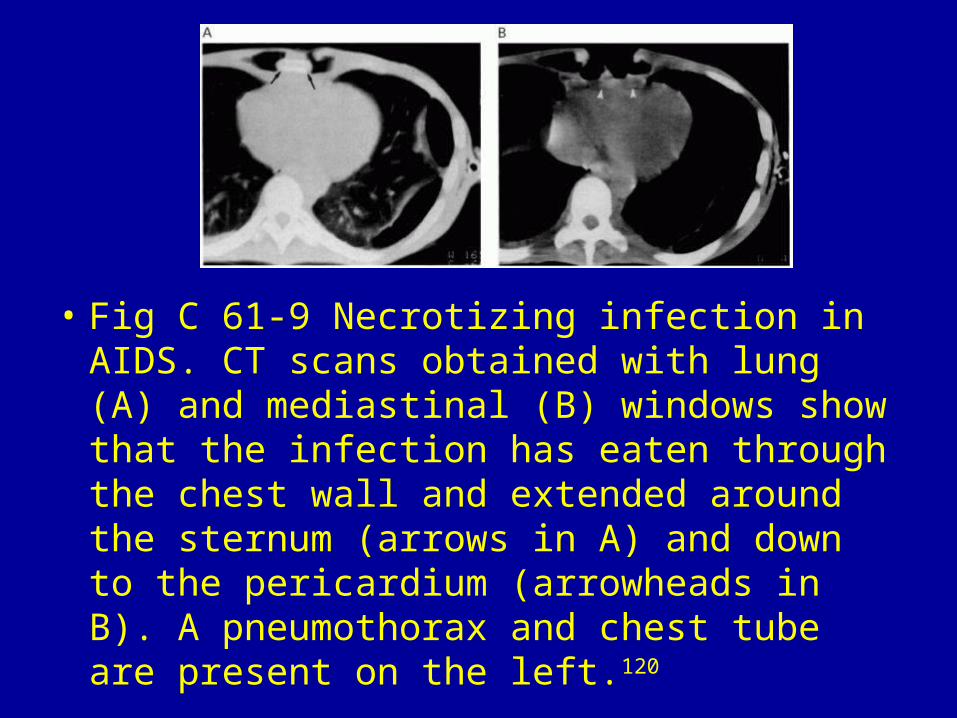
• Fig C 61-9 Necrotizing infection in AIDS. CT scans obtained with lung (A) and mediastinal (B) windows show that the infection has eaten through the chest wall and extended around the sternum (arrows in A) and down to the pericardium (arrowheads in B). A pneumothorax and chest tube are present on the left.120
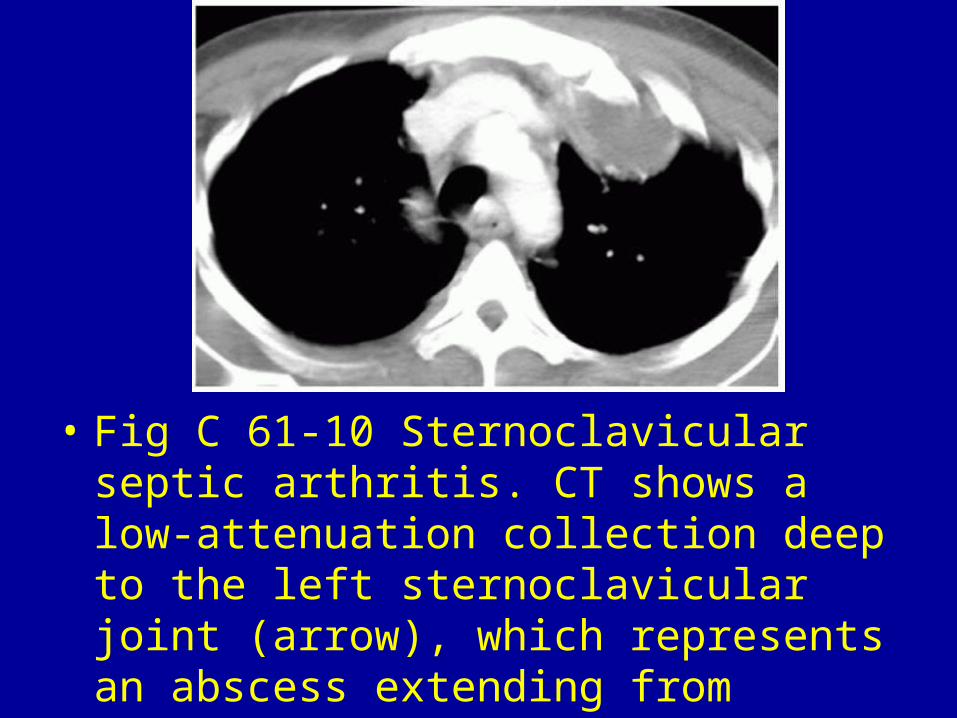
• Fig C 61-10 Sternoclavicular septic arthritis. CT shows a low-attenuation collection deep to the left sternoclavicular joint (arrow), which represents an abscess extending from infection of the joint in an intravenous drug abuser.10

• Fig C 61-11 Paget's disease. Bone enlargement with cortical thickening (arrow) involving the right posterior eighth rib.121
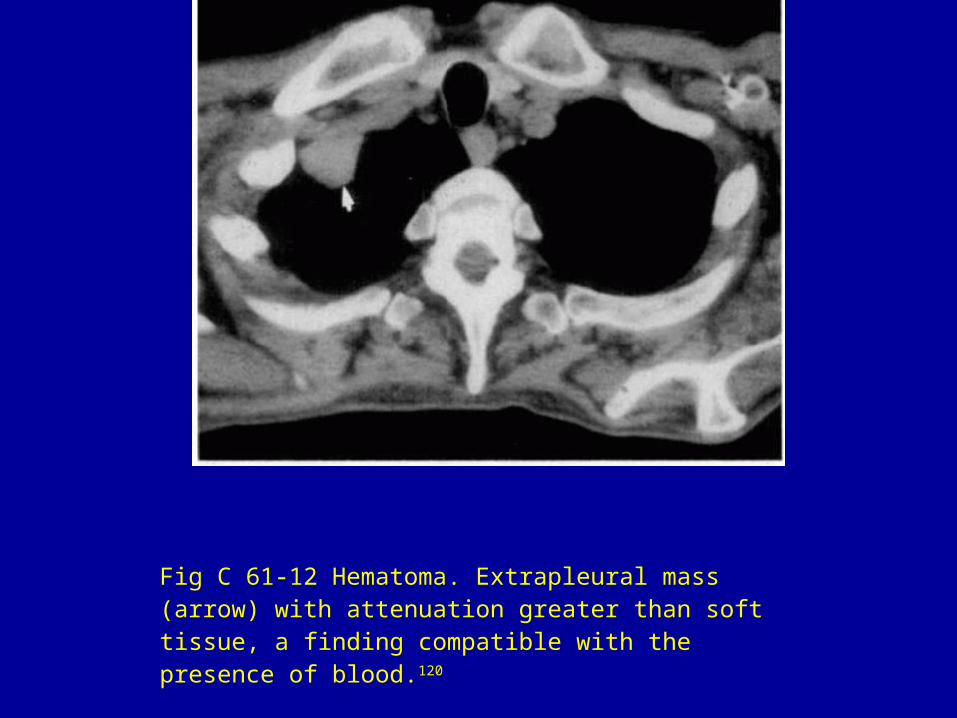
Fig C 61-12 Hematoma. Extrapleural mass (arrow) with attenuation greater than soft tissue, a finding compatible with the presence of blood.120
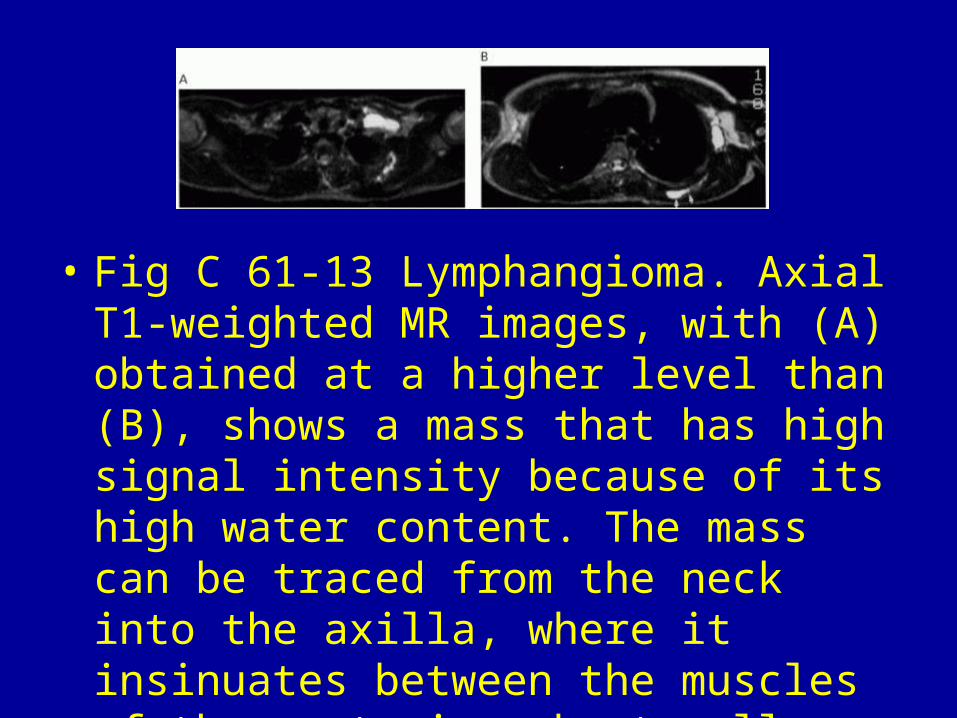
• Fig C 61-13 Lymphangioma. Axial T1-weighted MR images, with (A) obtained at a higher level than (B), shows a mass that has high signal intensity because of its high water content. The mass can be traced from the neck into the axilla, where it insinuates between the muscles of the posterior chest wall (arrows in B).120

• Fig C 61-14 Malignant fibrous histiocytoma. Axial T1-weighted contrast image shows a large extraparenchymal mass in the right upper hemithorax with marked enhancement. Focal areas of low signal intensity (arrow) are consistent with necrosis and fluid. The origin of the lesion within the chest wall musculature helps distinguish this tumor from osteosarcoma or chondrosarcoma.134
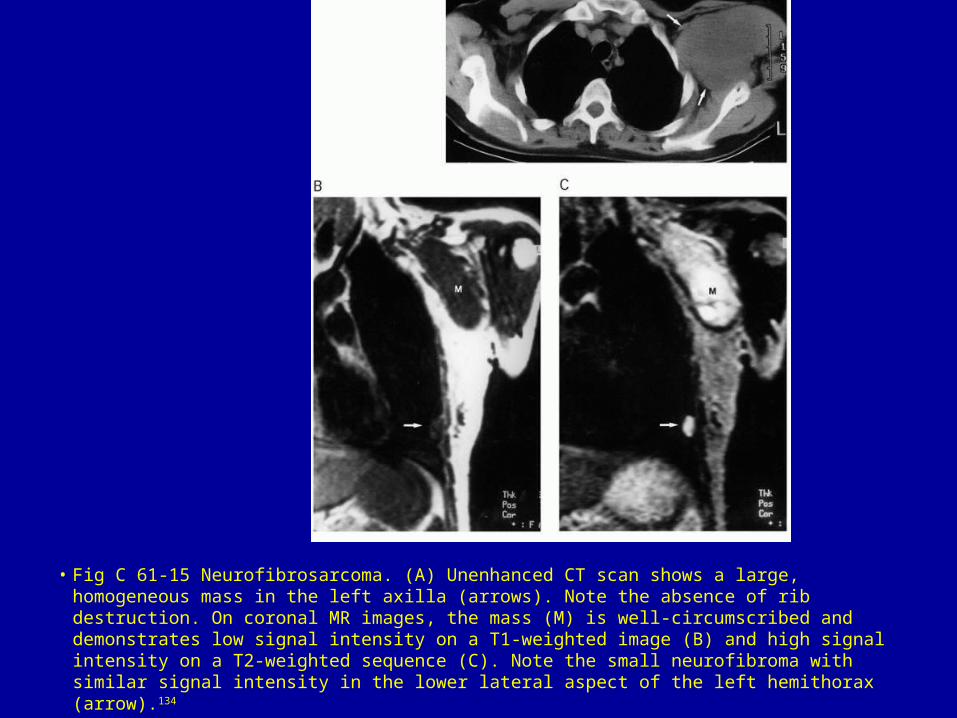
• Fig C 61-15 Neurofibrosarcoma. (A) Unenhanced CT scan shows a large, homogeneous mass in the left axilla (arrows). Note the absence of rib destruction. On coronal MR images, the mass (M) is well-circumscribed and demonstrates low signal intensity on a T1-weighted image (B) and high signal intensity on a T2-weighted sequence (C). Note the small neurofibroma with similar signal intensity in the lower lateral aspect of the left hemithorax (arrow).134
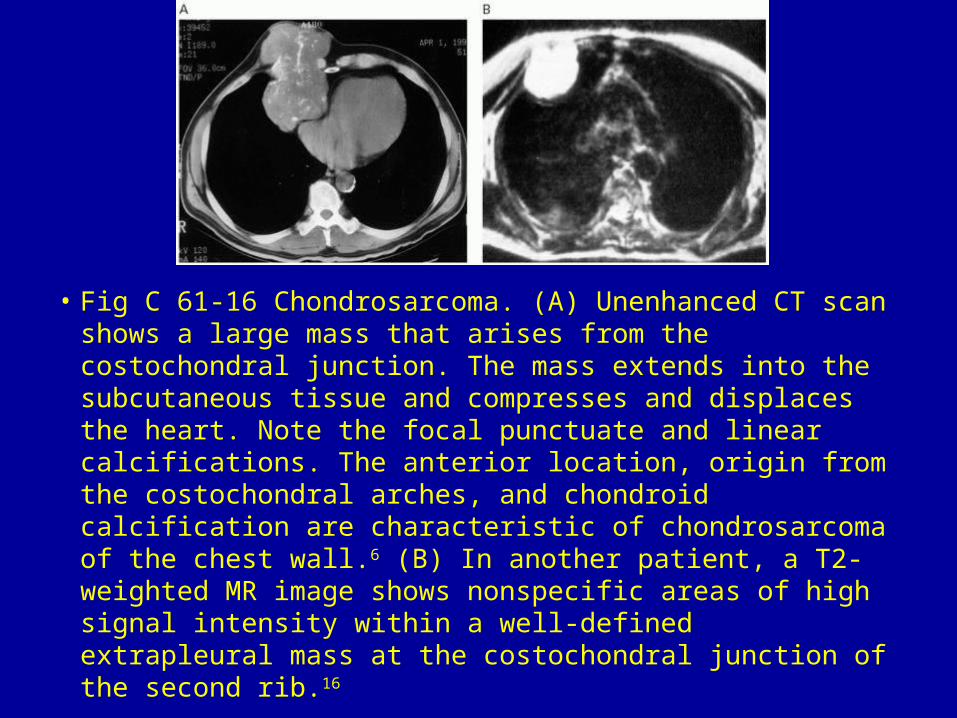
• Fig C 61-16 Chondrosarcoma. (A) Unenhanced CT scan shows a large mass that arises from the costochondral junction. The mass extends into the subcutaneous tissue and compresses and displaces the heart. Note the focal punctuate and linear calcifications. The anterior location, origin from the costochondral arches, and chondroid calcification are characteristic of chondrosarcoma of the chest wall.6 (B) In another patient, a T2-weighted MR image shows nonspecific areas of high signal intensity within a well-defined extrapleural mass at the costochondral junction of the second rib.16
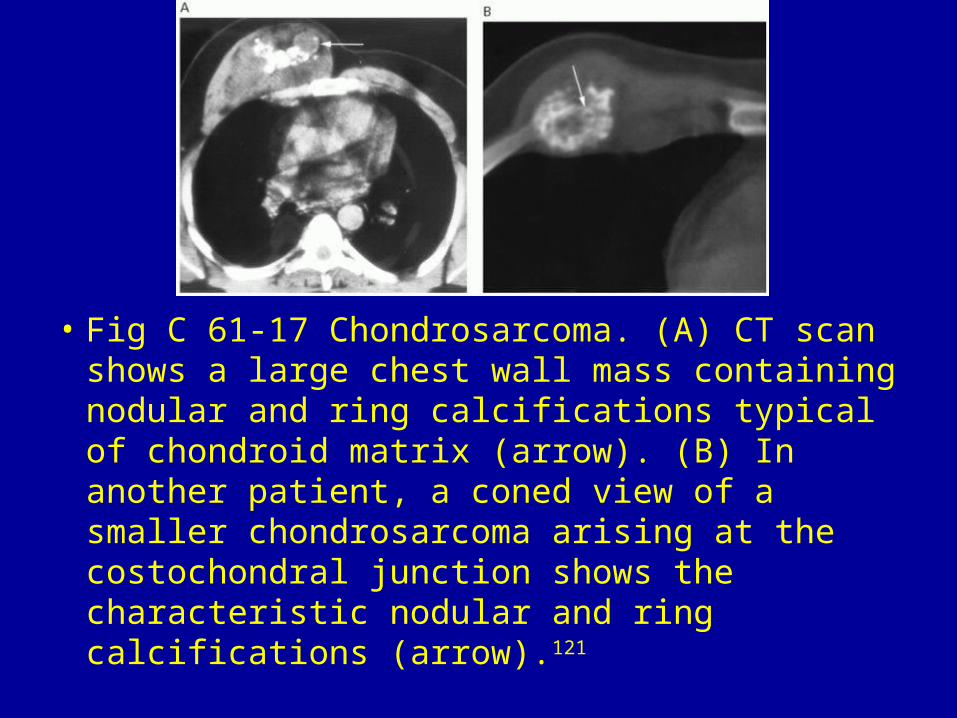
• Fig C 61-17 Chondrosarcoma. (A) CT scan shows a large chest wall mass containing nodular and ring calcifications typical of chondroid matrix (arrow). (B) In another patient, a coned view of a smaller chondrosarcoma arising at the costochondral junction shows the characteristic nodular and ring calcifications (arrow).121
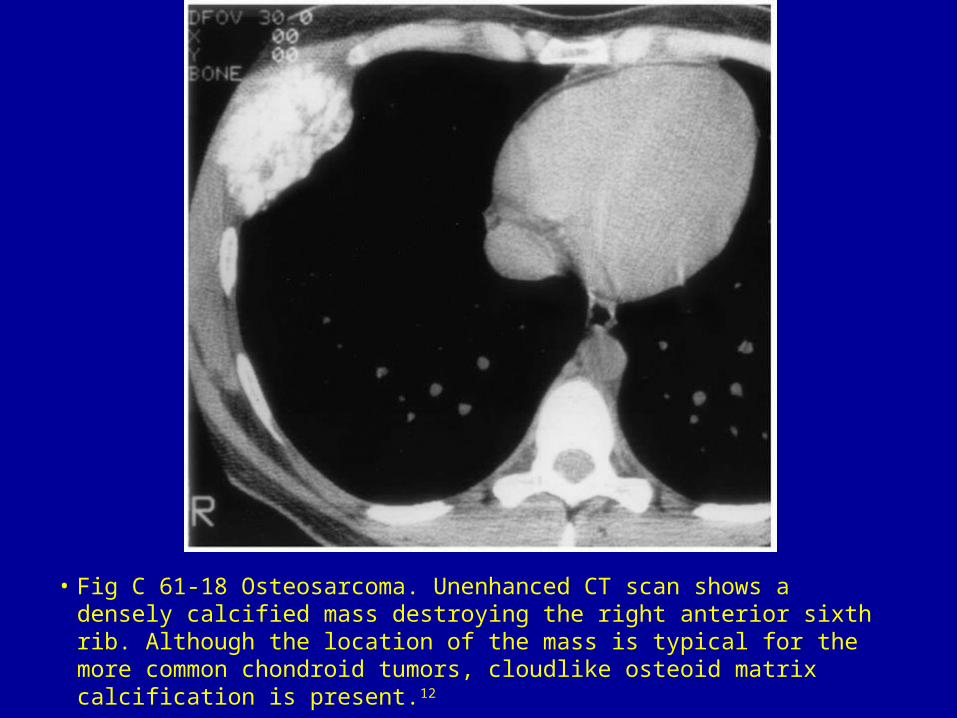
• Fig C 61-18 Osteosarcoma. Unenhanced CT scan shows a densely calcified mass destroying the right anterior sixth rib. Although the location of the mass is typical for the more common chondroid tumors, cloudlike osteoid matrix calcification is present.12
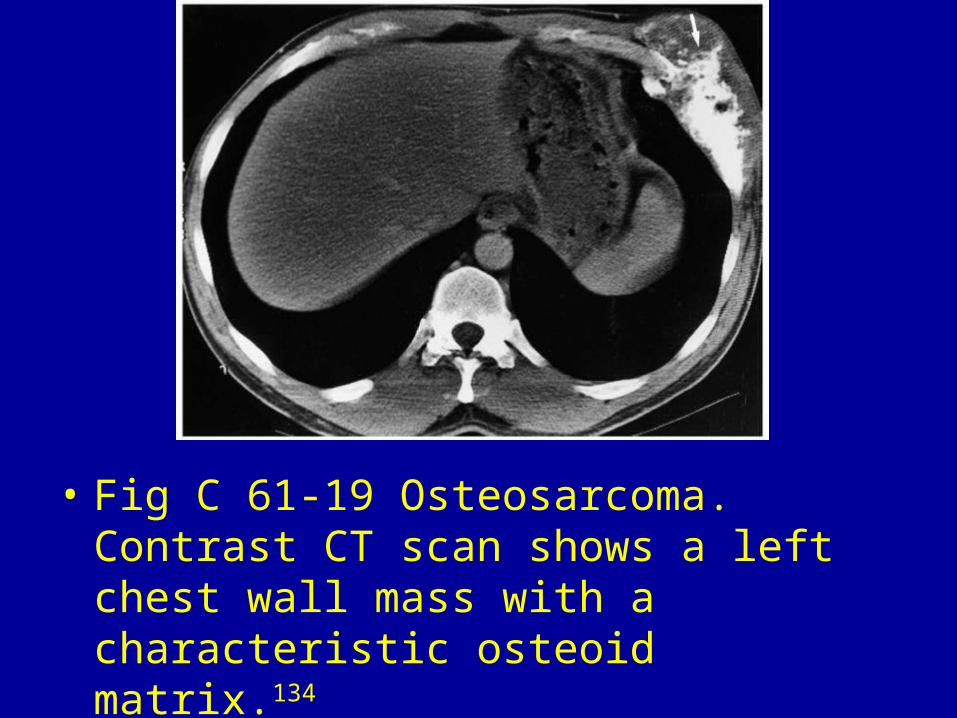
• Fig C 61-19 Osteosarcoma. Contrast CT scan shows a left chest wall mass with a characteristic osteoid matrix.134

• Fig C 61-20 Ewing's sarcoma. (A) Unenhanced CT scan shows a huge heterogeneous mass within the left hemithorax. There is destruction and inward displacement of a left rib (long arrow). Note the local invasion into the subcutaneous tissues (short arrow). (B) Coronal contrast T1-weighted MR image shows heterogeneous enhancement consistent with necrosis and hemorrhage. Note the marked displacement of mediastinal structures into the right hemithorax. LV = left ventricle.134
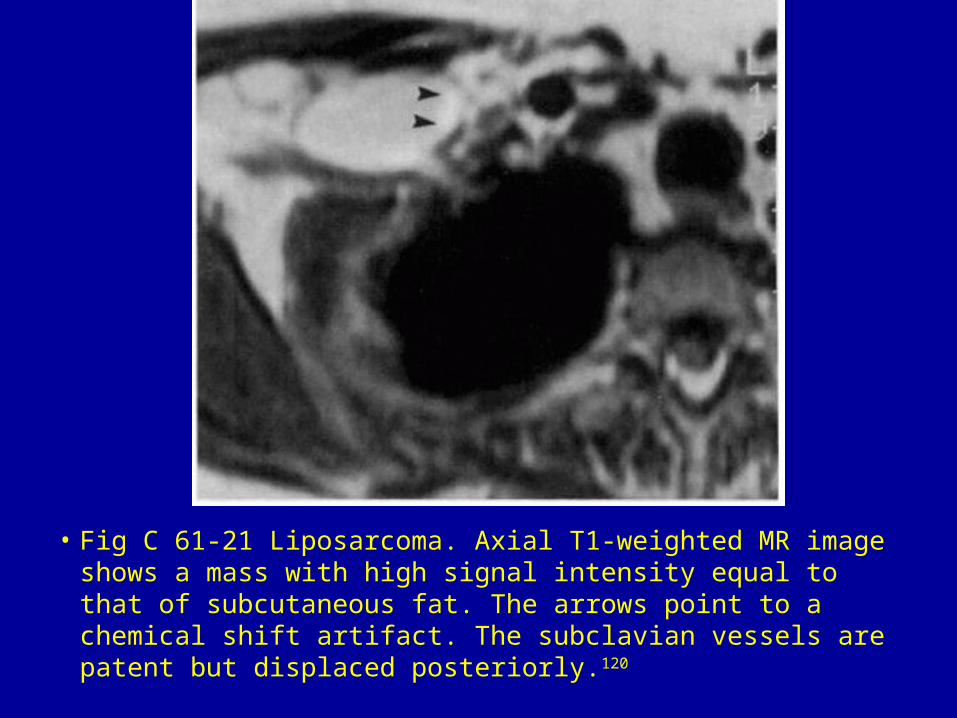
• Fig C 61-21 Liposarcoma. Axial T1-weighted MR image shows a mass with high signal intensity equal to that of subcutaneous fat. The arrows point to a chemical shift artifact. The subclavian vessels are patent but displaced posteriorly.120

• Fig C 61-22 Lymphoma. Axial T1-weighted MR image shows a parasternal mass involving the chest wall and left internal mammary node. The pericardial black line (arrows) is compressed and then obliterated, indicating invasion of this structure.119

• Fig C 61-23 AIDS-related lymphoma. CT scan shows a large mediastinal mass growing through the anterior chest wall in a parasternal location.120

• Fig C 61-24 Metastasis (breast cancer). CT scan shows a large ulcerating mass invading the upper chest wall. The sternum is eroded, and the tumor has grown into the suprasternal notch.120

• Fig C 61-25 Metastasis (hepatoma). CT scan shows a lytic rib lesion with large soft-tissue component.120

• Fig C 61-26 Metastasis (prostate cancer). CT scan demonstrates a mass that arises from the anterior fourth rib and has extensive underlying bone sclerosis.121
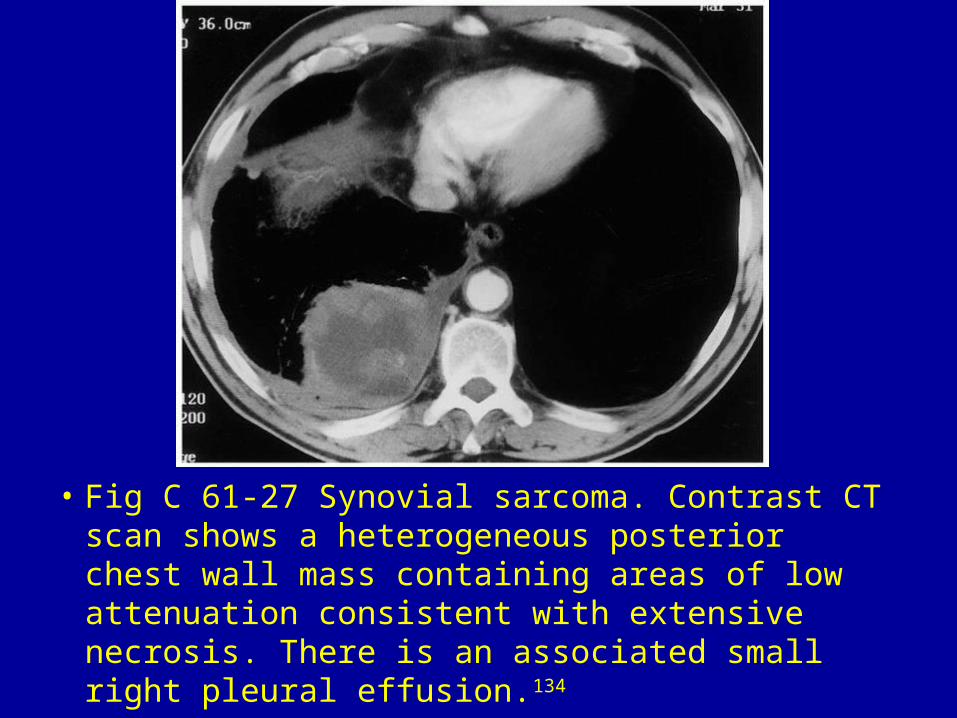
• Fig C 61-27 Synovial sarcoma. Contrast CT scan shows a heterogeneous posterior chest wall mass containing areas of low attenuation consistent with extensive necrosis. There is an associated small right pleural effusion.134

• Fig C 61-28 Pancoast tumor. (A) CT scan shows a mass in the apex of the right lung that destroys the first rib and invades the adjacent T2 vertebral body (arrows).2 (B) In another patient, a sagittal T2-weighted MR image shows a large mass arising in the apex of the right lung that has abnormal high signal intensity and infiltrates the supraclavicular fossa and surrounding brachial plexus.120

• Fig C 61-29 Mesothelioma. (A) CT scan shows a huge mass involving the anterior chest and abdominal wall with growth of tumor (arrows) beneath the xiphoid process and lower ribs. The tumor appears to be contiguous to the pericardium (arrowheads) and it is difficult to determine whether this structure has been invaded. (B) Corresponding axial T1-weighted MR image shows the intact black line of the pericardium (arrowheads), indicating no invasion.120


































