Embed Size (px)
Citation preview

Is Extended Field Concurrent Chemoradiation an Option for Radiologic Negative Para-aortic Lymph Nodes Locally Advanced Cervical Cancer?
Asiri MA, Tunio MA, Mohamed R, Bayoumi Y, Alhadab A, Saleh RM, AlArifi MS, Alobaid A ,K Salama, B Obaidat

CCRT is The standard treatment for locally advanced cervical cancer .
Five randomized trials showing survival benefit
Patients with locally advanced cervical cancer harbor 17-37% para-aortic nodal micrometastasis at time of diagnosis.
15-25% of patients experience para-aortic nodal failures after receiving combined pelvic chemoradiation in long term follow up.

Radiotherapy alone failed to control biopsy proven para-aortic lymph nodes (PALN),
Poor 5 year survival rates ( 29 to 50%).
Chemotherapy with extended field irradiation for biopsy proven PALN are associated with significant gastrointestinal and hematological toxicities
Hypothesis : EF-CCRT leads to results better to those obtained by WP-CCRT in patients with locally advanced cervical cancer with radiologic enlarged pelvic nodes and normal para-aortic lymph nodes (PALN).

PATIENTS AND METHODS:
Starting July 2007 Pathology :
Squamous cell carcinoma, Adenocarcinoma Adeno-squamous cell carcinoma
Radiologic negative PALN and enlarged pelvic nodes > 1cm.Stages IIB-IVA WP-CCRT (36 patients) and EF-CCRT (38 patients)

External beam radiation Therapy (EBRT):
WP-CCRT: (GTV), uterus, pre-sacral (PS), common iliac (CI), internal iliac (II) and
external iliac (EI) lymph nodes, with 1 cm margins
(PTV-1) with 0.5 to 1 cm margins around CTV
Boost covering enlarged lymph nodes and parametria,
(OAR) including kidneys, small bowel, bladder, rectum and femoral heads
3D-CRT and intensity modulated radiation therapy (IMRT)
Radiation doses were 45-50.4 GY/25-28 fractions
Radiological enlarged lymph nodes were boosted to dose of 50.4-54 GY.
EF-CCRT: The pelvis was treated similarly as WP-CCRT
Additional paraaortic fields were added as a continuous area
Superior field border at the junction of T12/L1 to cover PALN up to level of renal hila.
The prescribed radiation dose to paln was 45 GY
HDR brachytherapy for both group 21 GY/ 3 fractions.

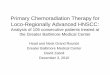
(A) EF-RT
(B) WP-RT)

(A) parametrial boost (PTV-2) of 5.4- 9 Gy with midline shielding
(B) high dose rate brachytherapy 21 Gy in three sessions

Concurrent chemotherapy:
Weekly cisplatin 40 mg/m2 before the administration of radiotherapy for six doses.

Toxicity scoring:
Week during CCRT.weight, performance status, hematologic and blood chemistry determinations3 monthly for the first 2 years, 6 monthly thereafter at radiation oncology and gynecology oncology clinics.
Response evaluationpelvic examination, Pap smear, CT chest and abdomen and pelvic MRI every 6 months for the first 2 years.

RESULTS:
WP-CCRT (36 patients) and EF-CCRT (38 patients) FIGO stage IIB (66.2%) FIGO stage IIIB (4.05%) Radiologic Enlarged pelvic lymph nodes (51.4%). The median follow-up time was 60 months. treatment protocol completion rate : 90 % in the WP-CCRT group 88.4% (95% CI,90-100) in the EF-CCRT group
Weekly concurrent cycles of cisplatin in both treatment arms were completed in all (100%) patients with no interruption.
Median duration of radiation therapy in both arms was 55.5 days with 95% CI: 48-58.

Variables Arm AExtended Field CCRT
(n=38)
Arm BPelvic Field CCRT
(n=36)p value
Age 52.3 years (32-78) 51.6 years (34-76) 0.9ECOG performance Scale 0-2 0-2 1.0
HistopathologySquamous cell Carcinoma
AdenocarcinomaAdeno-squamous cell carcinoma
34 (89.5%)3 (7.9%)1 (2.6%)
33 (91.7%)2 (5.6%)1 (2.8%)
0.7
FIGO stagingIIBIIIAIIIBIVA
24 (63.1%)6 (15.8%)4 (10.5%)4 (10.5%)
25 (69.4%)6 (16.6%)3 (8.3%)2 (5.6%)
0.8
Radiological Primary Tumor size<5 cm> 5 cm
13 (34.2%)25 (65.8%)
14 (38.9%)22 (61.1%)
0.6
Nodal EnlargementIliac
Common IliacPara-aortic
9 (23.7%)14 (36.8%)
-
13 (36.1%)2 (5.6%)
-
0.05
Pre-treatment hemoglobin>10 gm/dl<10 gm/dl
35 (92.1%)3 (7.9%)
34 (94.4%)2(5.6%)
0.9
Treatment3DCRTIMRT
EBRT:Whole PelvisPara-aortic
Parametrial/enlarged LN boostHDR-BT:
Dose/fractionTotal dose/fraction
Point A BEDICRU 38 rectal point BED
ICRU 38 bladder point BEDConcurrent weekly Cisplatin cycle:
Dose/weekMean cycles
30 (78.9%)8 (21.1%)
45 Gy (42-50.4)45 Gy (45-50.4)
9 Gy (5-9)
7 Gy/fraction21 Gy/3
86.4 Gy (80.5-102.7)85 Gy (80.5-100)86 Gy (80.5-102)
30mg/m2
5 (4-7)
36 (100.0%)-
45 Gy (42-50.4)-
9 Gy (5-9)
7 Gy/ fraction21 Gy/3
86.4 Gy (80.5-102.7)85 Gy (80.5-100)86 Gy (80.5-102)
30mg/m2
5 (4-7)
0.9
Patients’ characteristics

RESULTS: Toxicity :
grade 3 or 4 acute hematological and non-hematological
5.2% and 2.6% in the EF-CCRT
5.4% and 2.7% in the WP-CCRT
Both treatment arms had similar grade 3 or 4 acute gastrointestinal toxicity .
No patient in either arm underwent surgery for radiation-induced damage or died because of treatment related side effects.

Toxicity Arm AExtended Field CCRT
(n=38)
Arm BPelvic Field
CCRT(n=36)
p value
Acute:HematologicNeutropenia
ThrombocytopeniaAnemia
Non-hematologicNausea/vomiting
DiarrheaCystitis
Deranged Renal Functions
Deranged Liver Functions
G3 G4
1 (2.6%) 1 (2.6%)
0 00 0
0 01 (2.6%) 00 0
1. 00 0
G3 G4
1 (2.7%) 1(2.7%)
0 00 0
0 00 01 (2.7%) 0
1. 00 0
0.7
Late:Chronic cystitis
Intestinal obstructionProctitis
Neuropathy/ plexopathy
Hearing lossRenal
01 (2.6%)
0000
1.2.3.4.
1 (2.8%)0
0.8
Acute and Late treatment related toxicity profile

RESULTS: Pelvic, Para-aortic Relapse
Pelvic LR :
3 (8.3%) in WP-CCRT arm
3 (7.9%) in EF-CCRT,
Para-aortic nodal failures
5 (13.9%) in WP-CCRT
1 (2.6%) in EF-CCRT (p value 0.02)
5 para-aortic nodal failures were seen at level of junction L2 and L3 vertebrae and 2 (40%) at level of L1 vertebrae and in EF-CCRT arm one para-aortic nodal failure was seen at junction of T12 and L1 vertebrae.

RESULTS:
Distant failures 7 (19.4%) patients in WP-CCRT 4 (10.5%) patients from EF-
CCRT Combined distant and para-aortic
nodal failures 4 (11.4%) in WP-CCRT 1 (2.6%) in EF-CCRT group.

RESULTS:
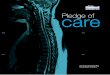
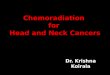
At the time of analysis, 32 patients in EF-CCRT and 27 patients in WP-CCRT group
were found without evidence of disease

para-aortic control
distant control
disease free survival
overall survival

RTOG 97-20 & 90-01 RTOG-97-20 trial,
EF-RT V WP-RT
10 Y FU
survival gain of 11% in EF-RT
No difference in LRC.
RTOG trial (RTOG 90-01)
EF-RT V WP-CCRT
5-year OS : (41% vs. 67% at 8 years) in favor of WP-CCRT
para-aortic failures : (7% WPCCRT vs. 4% EF-RT

Similar studies
Malfetano et al; weekly cisplatin concomitant EF-RT 67 women 75% of patients were alive without evidence of disease,
with no para-aortic failures.
Chung YL, 63 Concurrent cisplatin during first and fifth weeks of extended
field irradiation followed by two adjuvant cycles of cisplatin and 5-flouro-uracil
para-aortic nodal failures only 4.5% and OS rate of 81% at 3 years.

limitations of present study
Low sample size. Selection bias.Lack of baseline FDG/PET based
staging.

Recommendations :
Prophylactic EF-CCRT in patients with locally advanced cervical cancer patients with PET enlarged pelvic lymph nodes.
Multicenter, phase III trial using IMRT in prophylactic extended field irradiation with concurrent chemotherapy in FDG/PET negative PALN locally advanced cervical patients, to evaluate whether outcomes of EF-CCRT are truly better than those of WP-CCRT.

CONCLUSION:
Prophylactic EF-CCRT can be a reasonable option in patients with locally advanced cervical
cancer with radiologic enlarged pelvic lymph nodes and radiologic negative PALN.