Embed Size (px)
Citation preview
Drugs affecting bone Drugs affecting bone mineral mineral
homeostasishomeostasisPrepared by: Mirza Anwar Baig Prepared by: Mirza Anwar Baig
M.Pharm (Pharmacology)M.Pharm (Pharmacology)Anjuman I Islam's Kalsekar Technical Campus,Anjuman I Islam's Kalsekar Technical Campus,
School of Pharmacy.School of Pharmacy.New Panvel,Navi MumbaiNew Panvel,Navi Mumbai
Topic learning outcomesTopic learning outcomes1. Mechanism of absorption,MOA & role of minerals on bones.2. Diagnosis and symptoms of bone mineral homeostasis related disorders.3. Drugs for bone disorders with MOA at receptor level, side effects. 4. Pharmacotherapeutics for bone disorders.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 22
CalciumCalciumØØ Ca2Ca2++ is vital for muscle contraction is vital for muscle contractionØØ Ca2Ca2++ is vital for fusion, and release of storage is vital for fusion, and release of storage
vesicles.vesicles.ØØ intracellular Ca2intracellular Ca2++ acts as a critical second messenger acts as a critical second messenger ØØ promote blood coagulationpromote blood coagulationØØ support the formation and continuous support the formation and continuous
remodeling of the skeletonremodeling of the skeleton..ØØ Cross-linking of structural proteins in bone matrix.Cross-linking of structural proteins in bone matrix.ØØ In adult men ~1300g and 1000g in women, In adult men ~1300g and 1000g in women, ØØ 99% is in bone and teeth99% is in bone and teeth. . ØØ Normal serum calcium con. Normal serum calcium con. 8.5-10.4 mg/dL8.5-10.4 mg/dL
ØØ ionized (50%), ionized (50%),ØØ protein-bound (40protein-bound (40%)-(Albumin accounts for some 90%) %)-(Albumin accounts for some 90%) ØØ complexed (10%). complexed (10%).
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 33
CalciumCalciumThe steady-state content of calcium in bone reflects The steady-state content of calcium in bone reflects the net effect of the net effect of bone resorption and bone formationbone resorption and bone formationA labile pool of bone Ca2A labile pool of bone Ca2++ exchanges readily with exchanges readily with interstitial fluid. interstitial fluid. This exchange is modulated by This exchange is modulated by hormones, vitamins, hormones, vitamins, drugs, and other factorsdrugs, and other factors that directly alter bone that directly alter bone turnover or that influence the Ca2turnover or that influence the Ca2++ level in level in interstitial fluid.interstitial fluid.a diet a diet lowlow in calcium leads to a compensatory in calcium leads to a compensatory increase in fractional absorption owing partly to increase in fractional absorption owing partly to activation of activation of vitamin Dvitamin D. . drugs such as drugs such as glucocorticoids and phenytoin depress glucocorticoids and phenytoin depress intestinal Ca2+ transportintestinal Ca2+ transport..
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 44
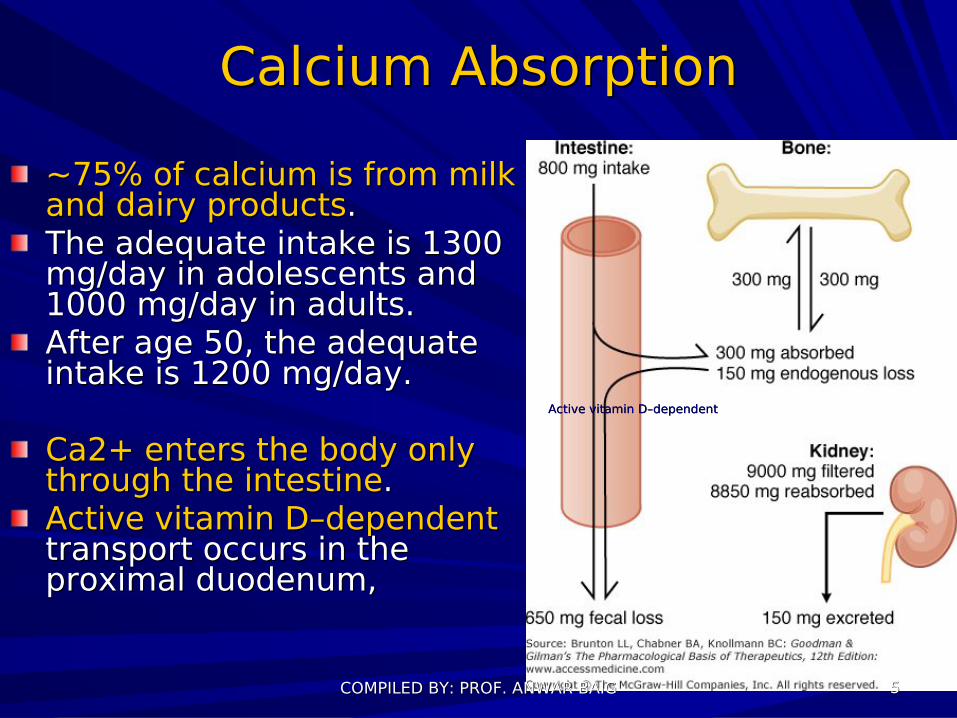
Calcium AbsorptionCalcium Absorption~75% of calcium is from milk ~75% of calcium is from milk and dairy productsand dairy products. . The adequate intake is 1300 The adequate intake is 1300 mg/day in adolescents and mg/day in adolescents and 1000 mg/day in adults. 1000 mg/day in adults. After age 50, the adequate After age 50, the adequate intake is 1200 mg/day.intake is 1200 mg/day.
Ca2+ enters the body only Ca2+ enters the body only through the intestinethrough the intestine. . Active vitamin DActive vitamin D––dependentdependent transport occurs in the transport occurs in the proximal duodenum,proximal duodenum,
Active vitamin DActive vitamin D––dependentdependent
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 55
Urinary CaUrinary Ca2+2+ excretion excretionAbout About 9 g9 g of Ca2+ are filtered each day. of Ca2+ are filtered each day.Tubular reabsorption Tubular reabsorption >98%>98% Reabsorption is regulated by parathyroid Reabsorption is regulated by parathyroid hormone hormone (PTH) (PTH) loop of Henle Diuretics (e.g., loop of Henle Diuretics (e.g., furosemidefurosemide) ) increaseincrease calcium excretion. calcium excretion.By contrast, By contrast, thiazidethiazide diuretics diuretics diminishingdiminishing calcium excretion calcium excretion
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 66
PhosphatePhosphateEssential Essential component of all bodycomponent of all body tissues, tissues, present in plasma, extracellular fluid, cell present in plasma, extracellular fluid, cell membrane membrane phospholipidsphospholipids, intracellular , intracellular fluid, collagen, fluid, collagen, and bone tissueand bone tissue..> > 80%80% of body phosphorus is in of body phosphorus is in bonebone, and , and ~15% is in soft tissue~15% is in soft tissuephosphate roles:phosphate roles:–– energy metabolismenergy metabolism–– key regulator of key regulator of enzyme activityenzyme activity when when
transferred by protein kinases from ATP to transferred by protein kinases from ATP to phosphorylatable serine, threonine, and phosphorylatable serine, threonine, and tyrosine residues.tyrosine residues.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 77
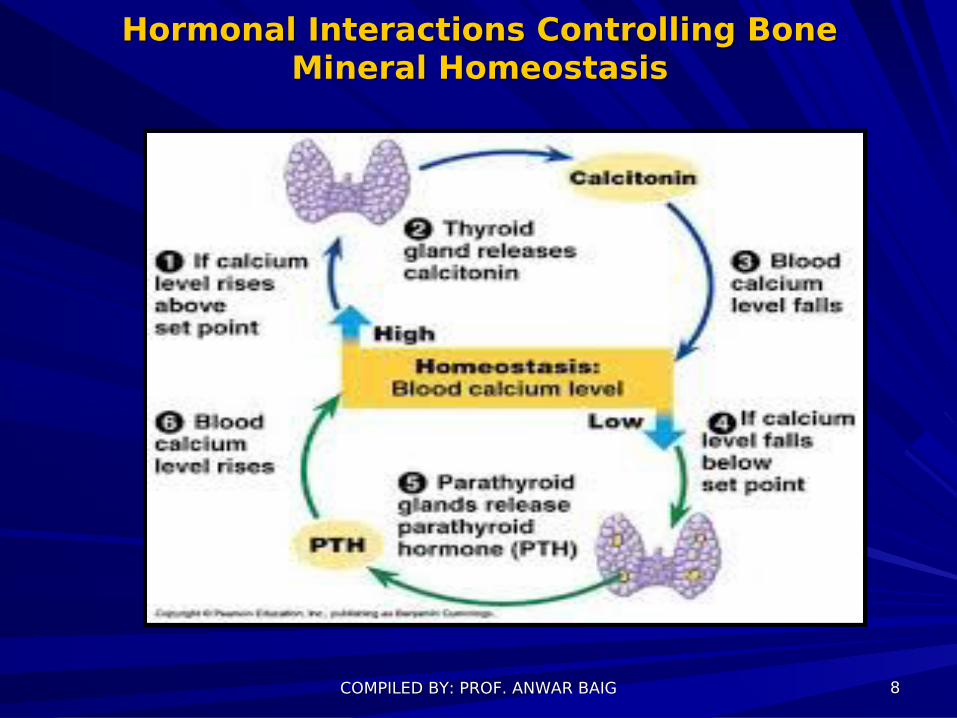
Hormonal Interactions Controlling Bone Hormonal Interactions Controlling Bone Mineral Homeostasis Mineral Homeostasis
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 88
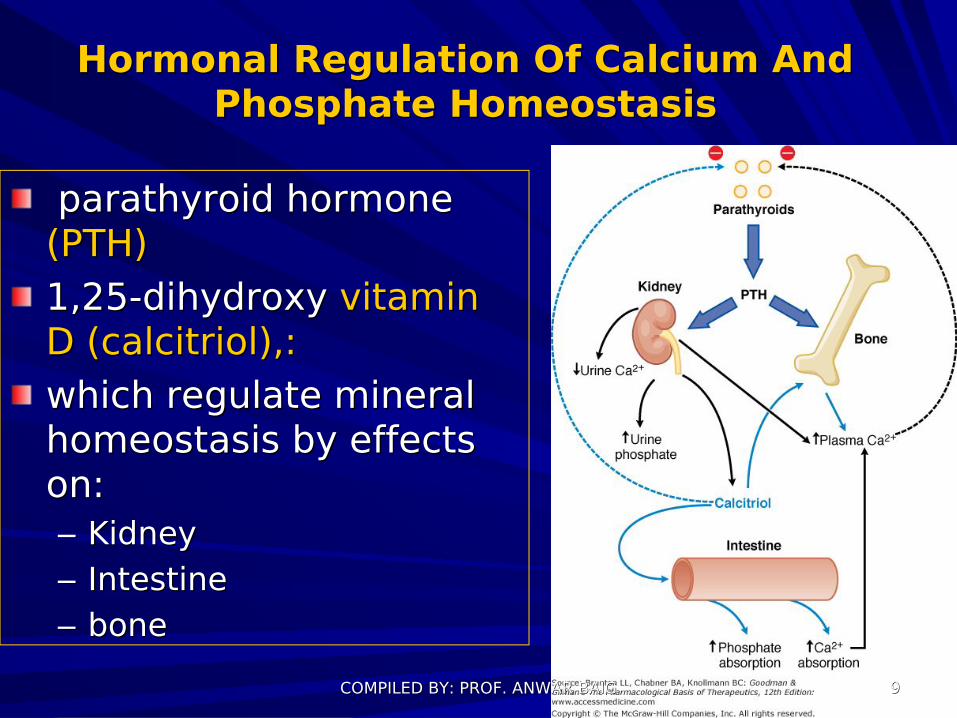
Hormonal Regulation Of Calcium And Hormonal Regulation Of Calcium And Phosphate HomeostasisPhosphate Homeostasis
parathyroid hormone parathyroid hormone (PTH)(PTH)1,25-dihydroxy 1,25-dihydroxy vitamin vitamin DD (calcitriol),:(calcitriol),: which regulate mineral which regulate mineral homeostasis by effects homeostasis by effects on:on:–– KidneyKidney–– IntestineIntestine–– bonebone
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 99
Parathyroid Hormone Parathyroid Hormone (PTH)(PTH)
PTH regulate plasma Ca2+ by PTH regulate plasma Ca2+ by affecting:affecting:–– Bone resorption/formationBone resorption/formation–– Renal Ca2+ excretion/reabsorptionRenal Ca2+ excretion/reabsorption–– Calcitriol synthesis (thus GI Ca2+ Calcitriol synthesis (thus GI Ca2+
absorption).absorption).
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 1010
PTH PTH CHEMISTRYCHEMISTRY
PTH - PTH - single polypeptidesingle polypeptide chains of 84 chains of 84 amino acids with molecular masses amino acids with molecular masses of ~9500 Da.of ~9500 Da.Biological activity is associated Biological activity is associated binding to the binding to the PTH receptorPTH receptor..signaling pathways: signaling pathways: CAMP or CAMP or IP3IP3––Ca2+.Ca2+.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 1111
PTH Regulation of SecretionPTH Regulation of Secretion
At LOWAt LOW Ca2+ PTH secretion Ca2+ PTH secretion increasesincreases. . hypocalcemiahypocalcemia induces parathyroid induces parathyroid hypertrophyhypertrophy and hyperplasia. and hyperplasia. Ca2+Ca2+ itself appears to regulate itself appears to regulate parathyroid gland parathyroid gland growthgrowth as well as hormone synthesis and as well as hormone synthesis and secretion.secretion.Adrenergic Adrenergic receptor agonists and dopamine receptor agonists and dopamine increaseincrease parathyroid cell cyclic AMP levels, and parathyroid cell cyclic AMP levels, and increase PTH secretion, increase PTH secretion,
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 1212
PTH Effects on BonePTH Effects on BonePTH enhances bone PTH enhances bone resorptionresorption and and thereby increases Ca2+ delivery to the thereby increases Ca2+ delivery to the extracellular fluid,extracellular fluid,The primary skeletal target cell for PTH is The primary skeletal target cell for PTH is the the osteoclastosteoclast, , PTH also recruits PTH also recruits osteoblastosteoblast precursor cells precursor cells to form new bone remodeling units. to form new bone remodeling units. PTH PTH in vivoin vivo reflects not only hormone reflects not only hormone action on individual cells but also the action on individual cells but also the increased total number of active increased total number of active osteoblasts, owing to initiation of new osteoblasts, owing to initiation of new remodeling units. remodeling units.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 1313
Vitamin DVitamin DVitamin D Vitamin D permit efficient absorption of permit efficient absorption of dietary calciumdietary calcium and to allow full and to allow full expression of the actions of PTH. expression of the actions of PTH. Vitamin D is actually a Vitamin D is actually a hormonehormone rather rather than a vitamin;than a vitamin;synthesized in synthesized in mammals andmammals and, under ideal , under ideal conditions, probably is not required in the conditions, probably is not required in the diet. diet. Receptors for the activated form of Receptors for the activated form of vitamin D are expressed in many cells: vitamin D are expressed in many cells: lymphocyteslymphocytes, epidermal cells, , epidermal cells, hair follicleshair follicles, , adipose tissueadipose tissue, pancreatic islets, muscle, , pancreatic islets, muscle, and neurons.and neurons.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 1414
Bone homeostasisBone homeostasis1.1.It involves multiple but coordinated cellular and molecular It involves multiple but coordinated cellular and molecular events.events. Two main types of cells are responsible for bone Two main types of cells are responsible for bone metabolism: metabolism: osteoblastsosteoblasts (which secrete new bone), and (which secrete new bone), and osteoclastsosteoclasts (which break bone down). (which break bone down). 2.2.The structure of bones as well as adequate supply of The structure of bones as well as adequate supply of calciumcalcium requires close cooperation between these two cell requires close cooperation between these two cell types.types.3.3.Bone metabolism relies on complex signaling pathways Bone metabolism relies on complex signaling pathways and control mechanisms to achieve proper rates of growth and control mechanisms to achieve proper rates of growth and differentiation. and differentiation. 4.4.These controls include the action of several hormones, These controls include the action of several hormones, including including parathyroid hormoneparathyroid hormone (PTH), (PTH), vitamin D, growth vitamin D, growth hormone, steroidshormone, steroids, and , and calcitonincalcitonin, as well as several , as well as several bone bone marrowmarrow-derived membrane and soluble -derived membrane and soluble cytokines cytokines and and growth factors. growth factors.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 1515
Bone remodeling unitBone remodeling unit
Subsequent to appropriate signaling, Subsequent to appropriate signaling, osteoclasts osteoclasts movemove to to resorb the surface of the bone, followed by resorb the surface of the bone, followed by deposition of bonedeposition of bone by osteoblasts. by osteoblasts.
Together, the cells that are responsible for bone Together, the cells that are responsible for bone remodeling are known as the remodeling are known as the basic multicellular unit basic multicellular unit (BMU)(BMU), and the temporal duration (i.e. lifespan) of , and the temporal duration (i.e. lifespan) of the BMU is referred to as the the BMU is referred to as the bonebone remodeling remodeling periodperiod..
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 1616
Bone remodelingBone remodelingBone remodelingBone remodeling (or (or bone metabolismbone metabolism) is a lifelong process ) is a lifelong process
where mature where mature bonebone tissuetissue is removed from the skeleton (a is removed from the skeleton (a process called process called bone resorptionbone resorption) and new bone tissue is ) and new bone tissue is formed (a process called formed (a process called ossificationossification or or new bone new bone formationformation). ).
These processes also control the reshaping or replacement These processes also control the reshaping or replacement of bone following injuries like of bone following injuries like fracturesfractures but also but also micro-micro-damagedamage (normal activity). (normal activity).
In the first year of life, almost 100% of the skeleton is In the first year of life, almost 100% of the skeleton is replaced. In adults, remodeling proceeds at about 10% perreplaced. In adults, remodeling proceeds at about 10% per
YYear.ear.[[
An imbalance in the regulation of bone remodeling's two An imbalance in the regulation of bone remodeling's two sub-processes, bone resorption and bone formation, results sub-processes, bone resorption and bone formation, results in many metabolic bone diseases, such as in many metabolic bone diseases, such as osteoporosisosteoporosis..
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 1717
OsteoporosisOsteoporosisOsteoporosis is a disease of the skeleton in which bones Osteoporosis is a disease of the skeleton in which bones become "thin" and prone to fracture. become "thin" and prone to fracture. In other words, the bone loses calcium and density. At In other words, the bone loses calcium and density. At age 65, about 30% of women have osteoporosis, and age 65, about 30% of women have osteoporosis, and nearly all of them are unaware of their condition. After nearly all of them are unaware of their condition. After age 80, up to 70% of women develop osteoporosis.age 80, up to 70% of women develop osteoporosis.OsteoporosisOsteoporosis is a major risk factor for fracture in the is a major risk factor for fracture in the spine and hip. The decrease in bone density can also spine and hip. The decrease in bone density can also lead to bone loss in the jaw and subsequent tooth decay.lead to bone loss in the jaw and subsequent tooth decay.Over Over 2 million2 million osteoporosis-related fractures occur in the osteoporosis-related fractures occur in the United States annually, with an estimated cost of $17 United States annually, with an estimated cost of $17 billion billion The prevalence of osteoporosis may be on the The prevalence of osteoporosis may be on the riserise, in , in part, due to a decrease in the overall routine utilization part, due to a decrease in the overall routine utilization of hormone replacement therapy of hormone replacement therapy (HRT)(HRT) for most for most postmenopausalpostmenopausal women. women. Also, while osteoporosis is less prevalent in men than Also, while osteoporosis is less prevalent in men than women, men account for almost 30% of low bone mass women, men account for almost 30% of low bone mass related (fragility) fracturesrelated (fragility) fractures COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG
1818
Secondary Hormonal RegulatorsSecondary Hormonal Regulators of Bone Mineral Homeostasis of Bone Mineral Homeostasis
CalcitoninCalcitonin: secreted by thyroid, T: secreted by thyroid, T1/21/2= 10 min,= 10 min, lower lower serum serum calcium and phosphatecalcium and phosphate by actions on by actions on bone bone and kidney.and kidney.GlucocorticoidsGlucocorticoids alter bone mineral homeostasis by alter bone mineral homeostasis by antagonizing vitamin D-stimulatedantagonizing vitamin D-stimulated intestinal calcium intestinal calcium transport, by stimulating renal calcium excretion, transport, by stimulating renal calcium excretion, and by blocking bone formation.and by blocking bone formation.Estrogens,Estrogens, prevent accelerated prevent accelerated bone lossbone loss by: by:–– reduce bone-resorbing action of PTH.reduce bone-resorbing action of PTH.–– increased 1,25(OH)2D level in bloodincreased 1,25(OH)2D level in bloodMay increased risk of breast cancer from continued May increased risk of breast cancer from continued
estrogen use estrogen use
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 1919
1. Calcitriol and
Analouges2. Bisphosphonates3. Calcimimetics:
Cinacalcet4. Calcitonin5. Estrogen6. Calcium7. Parathyroid hormone
Drugs for osteoporosis
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2020
1- Calcitriol and Analouges1- Calcitriol and Analouges
Available for Available for oraloral administration or administration or injectioninjection..I.V highI.V high doses of doses of calcitriol or one of calcitriol or one of its derivatives. its derivatives. predominant predominant used for patients used for patients with with chronic chronic kidney diseasekidney disease and and end-stage end-stage kidney disease.kidney disease.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2121
Therapeutic Indications for Therapeutic Indications for Vitamin DVitamin D
The major therapeutic uses of The major therapeutic uses of vitamin D may be divided into four vitamin D may be divided into four categories:categories:
–– ProphylaxisProphylaxis and cure of nutritional and cure of nutritional ricketsrickets (softening of bones in children) (softening of bones in children)
–– treatment of treatment of metabolic ricketsmetabolic rickets and and osteomalacia, particularly in the osteomalacia, particularly in the setting of chronic renal failuresetting of chronic renal failure
–– prevention and treatment of prevention and treatment of osteoporosisosteoporosis
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2222
Adverse Effects of Vitamin D TherapyAdverse Effects of Vitamin D Therapy
HypercalcemiaHypercalcemia, with or without , with or without hyperphosphatemia, may limit its hyperphosphatemia, may limit its use at doses that effectively use at doses that effectively suppress PTH secretion.suppress PTH secretion.Hypervitaminosis D is treated by:Hypervitaminosis D is treated by:–– immediate withdrawal of the vitaminimmediate withdrawal of the vitamin–– low-calcium dietlow-calcium diet–– administration of glucocorticoidsadministration of glucocorticoids–– loop diuretics is also useful. loop diuretics is also useful.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2323
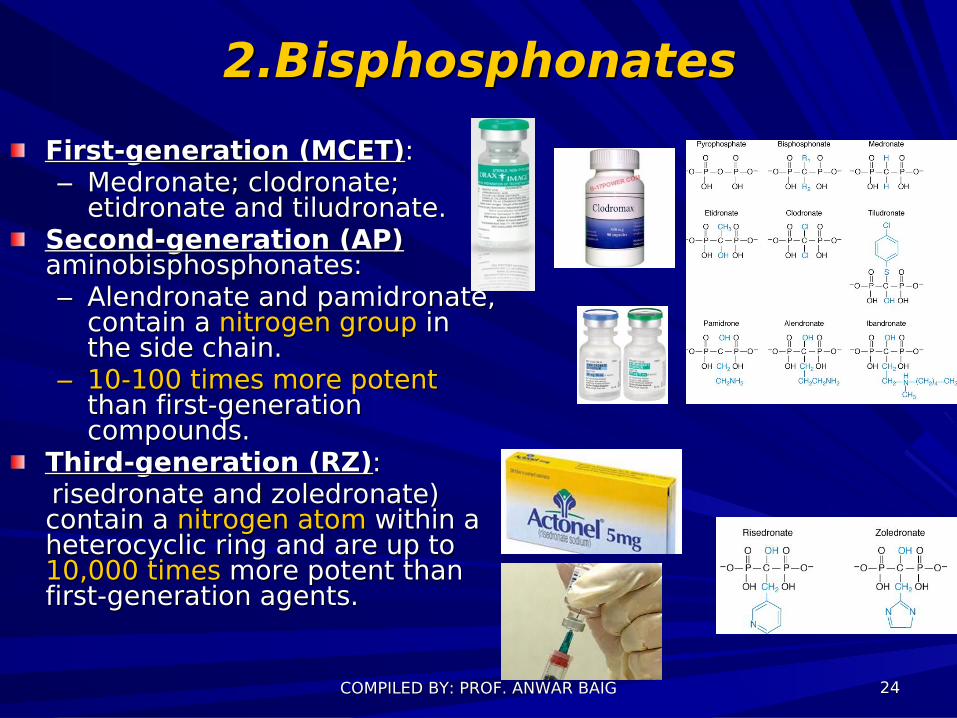
2.Bisphosphonates2.BisphosphonatesFirst-generation (MCET)First-generation (MCET)::–– Medronate; clodronate; Medronate; clodronate;
etidronate and tiludronate. etidronate and tiludronate. Second-generation (AP)Second-generation (AP) aminobisphosphonates:aminobisphosphonates:–– Alendronate and pamidronate, Alendronate and pamidronate,
contain a contain a nitrogennitrogen groupgroup in in the side chain. the side chain.
–– 10-100 times10-100 times more potentmore potent than first-generation than first-generation compounds.compounds.
Third-generation (RZ)Third-generation (RZ):: risedronate and zoledronate) risedronate and zoledronate)
contain a contain a nitrogen atomnitrogen atom within a within a heterocyclic ring and are up to heterocyclic ring and are up to 10,000 times10,000 times more potent than more potent than first-generation agents.first-generation agents.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2424
Bisphosphonates- MOABisphosphonates- MOAconcentrate at sites of active remodelingconcentrate at sites of active remodelingIncorporated into the Incorporated into the bone matrixbone matrix Analogue of pyrophosphateAnalogue of pyrophosphateAccelerate apoptosis of osteoclast reducing their Accelerate apoptosis of osteoclast reducing their numbernumberDisruption of cytoskeletal of osteoclastDisruption of cytoskeletal of osteoclastInhibit differentiation of osteoclast precursorInhibit differentiation of osteoclast precursorInactivation of osteoclast by disturbing Inactivation of osteoclast by disturbing mevalonate pathway (lipid synthesis)mevalonate pathway (lipid synthesis)
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2525
Uses of Bisphosphonates Uses of Bisphosphonates
Osteoporosis: Osteoporosis: Alendronate,risedronate are more Alendronate,risedronate are more effective than calctonineffective than calctoninPagets disease: Pagets disease: (Honey comb like bone)(Honey comb like bone)
Alendronate,risedronate,Pamidronate,zolendronate Alendronate,risedronate,Pamidronate,zolendronate are cheaper than calctonin.are cheaper than calctonin.
Hypercalcaemia of malignancy:Hypercalcaemia of malignancy: Pamidronate or zoledronate Pamidronate or zoledronate Combine with calcitonin Combine with calcitonin
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2626
BisphosphonatesBisphosphonates Absorption, Fate, and Excretion Absorption, Fate, and Excretion
All oralAll oral, , very poorly absorbed from the intestinevery poorly absorbed from the intestine, , low bioavailability (<1% [alendronate, low bioavailability (<1% [alendronate, risedronate] to 6% [etidronate, tiludronate]).risedronate] to 6% [etidronate, tiludronate]).Food reduces absorption:Food reduces absorption: Should be Should be administered with a administered with a full glassfull glass of water following of water following an overnight an overnight FASTFAST and at least 30 minutes and at least 30 minutes before breakfast.before breakfast.Oral bisphosphonates Oral bisphosphonates HAVE NOT BEEN used used widely in widely in CHILDRENCHILDREN or adolescents because of or adolescents because of uncertainty of long-term effects of uncertainty of long-term effects of bisphosphonates on the bisphosphonates on the growing skeletongrowing skeleton..Excreted by kidneys.Excreted by kidneys.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2727
Pamidronate is not available as an oral preparation because it causes gastric irritationHowever, with the possible exception of etidronate, all currently available bisphosphonates have this complication.~50% of absorbed drug accumulates in bone; rest excreted unchanged in the urine. Contraindications: esophageal motility disorders, peptic ulcer renal failer disease
BisphosphonatesBisphosphonates Absorption, Fate, and Excretion Absorption, Fate, and Excretion
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2828
Bisphosphonates Adverse EffectsBisphosphonates Adverse Effects
Very safeVery safeAt At higher doseshigher doses: gastric (etidronate) and : gastric (etidronate) and esophageal (pamidronate& alendronate) esophageal (pamidronate& alendronate) irritationirritation Irritation Irritation minimizedminimized by taking the drug by taking the drug with with glass of waterglass of water and remaining and remaining upright upright for 30for 30 minutes. minutes. Rare, Rare, OSTEONECROSISOSTEONECROSIS of the jaw ( of the jaw (ONJONJ), ), 1/100,000 with 1/100,000 with I.VI.V doses of doses of zoledronate zoledronate are used to control bone are used to control bone metastases and metastases and cancer-inducedcancer-induced hypercalcemia. hypercalcemia.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 2929
3- Calcimimetics: 3- Calcimimetics: CinacalcetCinacalcetCinacalcet: Cinacalcet: Cinacalcet blocks PTH secretionCinacalcet blocks PTH secretion
a a new classnew class of drugs that of drugs that activates the calcium sensing receptoractivates the calcium sensing receptor (CaR).(CaR).CaR is widely distributed but has its greatest concentration in the CaR is widely distributed but has its greatest concentration in the parathyroid gland. parathyroid gland.
Mechanism of actionMechanism of actionCinacalcet is a drug that acts as a Cinacalcet is a drug that acts as a calcimimetic calcimimetic by allosteric by allosteric activation of the calcium-sensing receptor . The calcium-sensing activation of the calcium-sensing receptor . The calcium-sensing receptors on the surface of the chief cell of the parathyroid gland receptors on the surface of the chief cell of the parathyroid gland is the principal regulator of parathyroid hormone secretion (PTH). is the principal regulator of parathyroid hormone secretion (PTH). Cinacalcet increases the sensitivity of calcium receptors on Cinacalcet increases the sensitivity of calcium receptors on parathyroid cells to reduce parathyroid hormone (PTH) levels and parathyroid cells to reduce parathyroid hormone (PTH) levels and thus decrease serum calcium levelsthus decrease serum calcium levels. As receptors are already . As receptors are already block from the calcimimetic (Cinacalcet) the native rise and fall of block from the calcimimetic (Cinacalcet) the native rise and fall of Ca levels now interact with the remaining receptors, effectively Ca levels now interact with the remaining receptors, effectively lowering the threshold for activation of feedback on the lowering the threshold for activation of feedback on the parathyroid chief cells.parathyroid chief cells.Approved for the treatment ofApproved for the treatment of secondary secondary hyperparathyroidismhyperparathyroidism in chronic in chronic kidneykidney disease and for the treatment of disease and for the treatment of parathyroid parathyroid carcinomacarcinoma..
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 3030

4- CALCITONIN4- CALCITONIN
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 3131
4- CALCITONIN4- CALCITONIN Calcitonin lowers plasma Ca2+ and phosphate concentrations in patients with hypercalcemia; by DECREASED BONE RESORPTION. Although calcitonin is effective for up to 6 hours in the initial treatment of hypercalcemia, LESS ACTIVE after a few days due to receptor downregulation.Development of antibodies with prolonged therapy.Salmon calcitonin is available as a NASAL SPRAY, introduced for once-daily treatment of postmenopausal osteoporosis. Side effects: Nausea, hand swelling, urticaria, rarely, intestinal cramping.
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 3232
5- Estrogen5- EstrogenHelping to maintain a Helping to maintain a normal bonenormal bone resorption rate. resorption rate. SUPPRESSES THE PROLIFERATION SUPPRESSES THE PROLIFERATION AND DIFFERENTIATION OF AND DIFFERENTIATION OF OSTEOCLASTSOSTEOCLASTS Increases Increases osteoclast apoptosisosteoclast apoptosis..DecreasesDecreases the production of several the production of several cytokines that are cytokines that are potent stimulators potent stimulators of osteoclastsof osteoclasts (IL-1. IL-6, TNF) (IL-1. IL-6, TNF)Decreases the production of Decreases the production of RANKLRANKL and increases the production of OPG; and increases the production of OPG; both of which both of which reduce reduce osteoclastogenesisosteoclastogenesis. .
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 3333
EstrogenEstrogenPostmenopausal or estrogen Postmenopausal or estrogen deficiency deficiency increases riskincreases risk for for osteoporosisosteoporosisEstrogen replacementEstrogen replacement effective in effective in conservation of bone and protection conservation of bone and protection against osteoporotic fracture after against osteoporotic fracture after menopausemenopause Side effects: increased risks of Side effects: increased risks of heart heart diseasedisease and and breast cancerbreast cancer were were found in chronic treatmentfound in chronic treatment
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 3434
RALOXIFINE (Evista)RALOXIFINE (Evista)Selective estrogen receptor Selective estrogen receptor modulatormodulatorDecrease bone resorptionDecrease bone resorption60mg 1Xday60mg 1XdaySide effectsSide effects::–– Hot flushesHot flushes–– leg crampsleg cramps–– Thrombolism Thrombolism Contraindicatin:Contraindicatin:–– Pregnancy/lactationPregnancy/lactation–– Pulmonary embolism Pulmonary embolism COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 3535
6- Calcium6- Calcium
There isThere is controversy controversy about the role of calcium about the role of calcium during the early years after menopause, when during the early years after menopause, when the primary basis for bone loss is estrogen the primary basis for bone loss is estrogen withdrawal. withdrawal.
Patients who are Patients who are unable or unwillingunable or unwilling to increase to increase calcium by dietary means alone may choose calcium by dietary means alone may choose from many palatable, from many palatable, low-cost calcium low-cost calcium preparationspreparations. . ORAL ORAL CALCIUM CARBONATECALCIUM CARBONATE, which , which should should be taken withbe taken with mealsmeals to facilitate dissolution and to facilitate dissolution and absorption. absorption. Traditional dosing of calcium Traditional dosing of calcium is ~1000 mg/dayis ~1000 mg/day, , nearly the amount present in a quart of milk. nearly the amount present in a quart of milk. Adults >50 years of age need 1200 mg of Adults >50 years of age need 1200 mg of calcium daily. calcium daily. COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 3636
7- Parathyroid hormone:7- Parathyroid hormone:TERIPATIDE (Forteo)TERIPATIDE (Forteo)
ACTS AS PARATHYROID HORMONE (PTH)ACTS AS PARATHYROID HORMONE (PTH)Increase bone formation by stimulation of Increase bone formation by stimulation of OsteoblastsOsteoblastsIncrease Increase renal reabsorptionrenal reabsorption of calcium of calcium20mg 1xday20mg 1xday
Side effectsSide effects::–– Orthostatic hypotensionOrthostatic hypotension–– HypercalcemiaHypercalcemia
ContraindicationContraindication::–– HypercalcemiaHypercalcemia–– HypersinsitivityHypersinsitivity
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 3737
THE ENDTHE END
COMPILED BY: PROF. ANWAR BAIGCOMPILED BY: PROF. ANWAR BAIG 3838