Embed Size (px)
Citation preview

overviewoverview
Anatomy & physiology of esophagus (gullet)
Anatomy & physiology of trachea, Tracheotomy
Anatomy of cervical part Neck masses Neck Dissection

Anatomy & physiology Anatomy & physiology of esophagusof esophagus

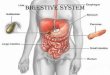
Esophageal AnatomyEsophageal AnatomyMuscular tubeMuscular tubeconnecting the connecting the pharynx to the pharynx to the Stomach, channelStomach, channelfor the transport of for the transport of foodfood 18 to 26 cm in le18 to 26 cm in le
ngthngth Back: vertebra Back: vertebra
(C6---T11)(C6---T11) Front: larynx & lFront: larynx & l
ower airwayower airway

Esophageal AnatomyEsophageal Anatomy
Upper EndUpper End : C6 : C6 (the inferi(the inferi
or pharyngeal constrictor merges or pharyngeal constrictor merges
with the cricopharyngeuswith the cricopharyngeus) __) __ UpUpper esophageal sphincter per esophageal sphincter (UES)(UES)Lower EndLower End: T11 : T11 (thickene(thickene
d circular smooth muscle)d circular smooth muscle) __ __ LoLower esophageal sphincter wer esophageal sphincter (LES) (LES)

Esophageal AnatomyEsophageal Anatomy
38-40cm from incisors38-40cm from incisors

Esophageal AnatomyEsophageal Anatomy
It is divided into three parts Cervical parts Thoracic parts Abdominal parts

Esophageal ConstrictionsEsophageal Constrictions
The esophagus has 3 areas of narrowing: Superiorly: level of cricoid cartilage, juncture with pharynx Middle: crossed by aorta and left main bronchus Inferiorly: diaphragmatic sphincter

Esophageal ConstrictionsEsophageal Constrictions
These narrowing areas have important clinical significance
where most esophageal foreign bodies become entrapped.

Esophageal AnatomyEsophageal Anatomy
Innervation mainly by celiac ganglia (Vagus n.)

Esophageal physiologyEsophageal physiology
1. swallow (Esophageal Transport by Gravity)
The oropharyngeal phase : Swallowing begins when a food bolus is propelled into the pharynx from the mouth. It is voluntary.
The esophageal phase. It is involuntary. It takes approximately 8 to 10 seconds fro
m initiation of the swallow to entry into the stomach .
In rapid sequence and with precise coordination, the larynx is elevated and the epiglottis seals the airway.

Esophageal physiologyEsophageal physiology
2.Secretion (submucosal mucous glands)
3.Protection : Gastroesophageal reflux (machenic , secretion )

Gastroesophageal reflux (GER)Gastroesophageal reflux (GER)
The gastric content (acid, pepsin, bile
salts, and pancreatic enzymes) refluxed into the esophagus.
It can damage the mucosa through the presence of hydrochloric.

TestsTests1. X-ray Plain X-ray : mental or some foreign bodies
Barium X-ray :As the oesophagus, stomach and duodenum are soft tissue structures, they are not usually seen on a plain X-ray. By using barium to coat the inner lining of these areas, the Radiologist can see them clearly on the X-ray screen; and can watch the way the organs function during this study.
Barium is a chalky substance that can be suspended in water and is visible on X-rays

Barium X-rayBarium X-ray

TestsTests X-ray barium test indications Difficulty or pain in swallowing; Be troubled by indigestion or acid reflux; An ulcer or blockage in the stomach is
suspected.

TestsTests Endoscopy (Rigid & flexible telescope-under sedation)
Rigid Endoscopy

TestsTests flexible telescope

Anatomy & physiology of Anatomy & physiology of the Respiratory tractthe Respiratory tract

The Respiratory tractThe Respiratory tract
The airway begins at the mouth or nose, and accesses the trachea via the pharynx through which air flows, to get from the external environment to the alveoli. Upper respiratory passages filter and humidify
incoming air Lower passageways include delicate conduction
passages and alveolar exchange surfaces

The Components of the Respiratory SystemThe Components of the Respiratory System
the mouth or nose, the
pharynx. the larynx
(cricoid cartilage), the
trachea, the left and
right main bronchi ,
large bronchioles,
clusters of alveoli.

The Components of the Respiratory SystemThe Components of the Respiratory System
The cricoid cartilage, or simply cricoid ("ring-shaped"), is the only complete ring of cartilage around the trachea. It is very important to support the airway.

The Anatomy of the TracheaThe Anatomy of the Trachea
The trachea is a tubular structure which is located at the front of the neck Begins: the level of the C6 ( the thyroid cartilage). Bifurcating: into right and left main bronchi (the level of the T5)Length: 10 to 15cm Diameter :16-18 mm

The Anatomy of the TracheaThe Anatomy of the Trachea
Structure of the Trachea wall
Anterior wall: cartilaginous rings (16 to 20 C-shaped )Posterior wall: fibromuscular sheet (ligaments)Posterior : esophagus

Physiology of the TracheaPhysiology of the Trachea
Respiration: air moving in and out of the lungs
Filter particulate matter, humidify inspired air, and aid in expectoration of secretions.
Physiology of Airway Protection: coughing reflex

Physiology of the TracheaPhysiology of the Trachea
The hyaline cartilage in the tracheal wall provides support and keeps the trachea from collapsing.
The posterior soft tissue allows for expansion of the esophagus, which is immediately posterior to the trachea.

Tracheotomy

DefinitionDefinition
An opening surgically created through the neck into the trachea (windpipe). A tube is usually placed through this opening (tracheostomy tube also trach tube) to provide an airway and to allow removal of secretions from the lungs. It provides an alternative airway, by passing the upper passages .

Tracheostomy tubesTracheostomy tubes
Inserted through
the tracheostomy
to maomtaom a
patent airway Secured in place
by tapes tied
around the neck

PurposePurpose A tracheotomy is performed if enough air is not getti
ng to the lungs, if the person cannot breathe . The conditions in which a tracheotomy may be used 1. Acute setting Maxillofacial injuries Large tumors of the head and neck, congenital tumors, e.g.
branchial cyst Acute inflammation of head and neck2. Chronic / elective setting - when there is need for long term
mechanical ventilation to pump air into the lungs for a long period of time and tracheal toilet
comatose patients, surgery to the head and neck.

Operative procedures Emergency tracheotomy (cricothyroid
otomy) Surgical tracheotomy
(nonemergency tracheotomy )

(A). An incision is made in the skin just above the sternal notch Just below the thyroid,
(B). The membrane covering the trachea is divided
(C). The trachea itself is cut
(D). A cross incision is made to enlarge the opening
(E). A tracheostomy tube may be put in place
Completed
tracheotomy

Operative procedures
Completed tracheotomy1 - Vocal cords2 - Thyroid cartilage3 - Cricoid cartilage4 - Tracheal cartilages5 - Balloon cuff

ComplicationsComplications Bleeding. In very rare situations, the need for blood
products or a blood transfusion. Need for further and more aggressive surgery. Infection. Impaired swallowing and vocal function. Scarring of the neck. Air trapping in the surrounding tissues (subcutaneous e
mphysema) or chest (Pneumothorax). In rare situations, a chest tube may be required.
Need for a permanent tracheostomy. This is most likely the result of the disease process which made the a tracheostomy necessary, and not from the actual pr
ocedure itself.

Complications Complications (rare) (rare)
Damage to the larynx (voice box) or airway with resultant permanent change in voice
Airway obstruction (tube obstruction) and aspiration of secretions/ accidental decannulation –the most common cause of death.
Scarring of the airway or erosion of the tube into the surrounding structures

Postoperative carePostoperative care
Objective : ensure patent airway. Prevent the complications
Chest x- ray Antibiotics Suctioning and clearing the
tracheotomy tube Humidifying the air

Postoperative carePostoperative careNormally nasal breathing Humidifies, filters and warms air
before it enters the lungs The tracheostomy bypasses these
mechanisms so that the air is cooler, dryer, and not as clean. In response to these changes the body produces more mucous, which may require humidification to aid expulsion.

Postoperative carePostoperative care Tracheostomy tube changs
a. Tracheostomy tubes are changed weekly or any time a blockage is suspected.
b. To prevent build up of secretios on the wall of the tube

Postoperative carePostoperative care Some precautions with a Tracheostomy Water is a serious threat No swimming No showering Avoid clothing that blocks the Tracheos
tomy Accidental decannulation -most commo
n cause of death.

Postoperative carePostoperative care
The tube will be removed if the tracheotomy is temporary. Then the wound will heal quickly and only a small scar may remain.
Weaning is a gradual decrease in the tube size and ultimate removal of the tube.
If the tracheotomy is permanent, the hole stays open.

Anatomy of neckAnatomy of neck

Introduction Introduction The neck contains important
communications between the head and the body, including air and food passages, major blood vessels and nerves, and the spinal cord. Many vital structures are compressed into a narrow area which is engineered for maximal mobility to permit variation in head position relative to body.

Anatomy of neckAnatomy of neck Skeleton: vertebral
column,hyoid bone, and laryngeal and trac
heal cartilages Muscles Nerves Major Vascular
Structures Visceral Column
- pharynx, larynx, trachea, and esophagus.
Thyroid Gland Between Mandibular notch and Clavicle

Anatomic trianglesAnatomic triangles
The neck can be divided into two major triangles (anterior and posterior triangles) by the sternocleidomastoid (SCM), with multiple smaller triangles
Anatomic triangles

Anatomic trianglesAnatomic triangles
Two major triangles Anterior triangle - b
ordered by the anterior border of the SCM, midline of the neck, and the mandible
Posterior triangle - bordered by the posterior border of the SCM, t
rapezius, and clavicle
A: muscular triangle, carotid triangl, esubmen
tal triangle, submandibular triangle
P: supraclavicular triangle,
occipital triangle

MusclesMuscles of neck of neck

Major VascularMajor Vascular

Major VascularMajor Vascular
Major Vascular Structures bifurcates into:
Internal (intracranial) - no branches in the neck
External (extracranial) Thyrocervical trunk Vertebral artery Internal jugular vein (within c
arotid sheath) External jugular vein

Lymphatic drainageLymphatic drainage Lymphatic drainage: major he
ad and neck lymph node groups. The lymph nodes of the neck can be divided into six levels within the defined anatomic triangles.
I--Submental and submandibular nodes II--Upper jugulodigastric group III--Middle jugular nodes IV--Inferior jugular nodes V-- Posterior triangle group VI--Anterior compartment group

Lymphatic drainageLymphatic drainage These groups and the areas that
they drain are particularly important when locating and working up a "neck mass" or possible malignancy. The groups and drainage areas are as follows.

Lymphatic drainageLymphatic drainage
Individual Lymph Nodes in the Head and Neck

Lymphatic drainage (Lymphatic drainage (Level I)Level I)
Submental triangle (Ia) Anterior digastric Hyoid Mylohyoid
Submandibular triangle (Ib)
Anterior and posterior digastric
Mandible.

Lymphatic drainageLymphatic drainage Ia
Chin Lower lip Anterior floor of mout
h Mandibular incisors Tip of tongue
Ib Oral Cavity Floor of mouth Oral tongue Nasal cavity (anterio
r) Face

Lymphatic drainage (Lymphatic drainage (Level Level IIII)) Upper Jugular Nodes Anterior Lateral border of st
ernohyoid, posterior digastric and stylohyoid
Posterior Posterior border of SCM
Skull base Hyoid bone (clinical landmark) Carotid bifurcation (surgical la
ndmark)

Lymphatic drainage (Lymphatic drainage (Level Level IIII))
Oral Cavity Nasal Cavity Nasopharynx Oropharynx
Larynx Hypopharynx Parotid

Lymphatic drainage (Level III)Lymphatic drainage (Level III)
Middle jugular nodes Anterior Lateral border of s
ternohyoid Posterior Posterior border o
f SCM Inferior border of level II Cricoid cartilage lower border
(clinical landmark) Omohyoid muscle (surgical la
ndmark) Junction with IJV

Lymphatic drainage (Level III)Lymphatic drainage (Level III)
Oral cavity Nasopharynx Oropharynx Hypopharynx Larynx

Lymphatic drainage (Level IV)Lymphatic drainage (Level IV) Lower jugular nodes Anterior Lateral border of st
ernohyoid Posterior Posterior border o
f SCM Cricoid cartilage lower border
(clinical landmark) Omohyoid muscle (surgical lan
dmark) Junction with IJV Clavicle

Lymphatic drainage (Level IV)Lymphatic drainage (Level IV) The thoracic duct: Conveys lymph from the entire
body back to the blood Exceptions:Right side of head and
neck, RUE, right lung right heart and portion of the liver
Begins at the cisterna chyli Enters posterior mediastinum betw
een the azygous vein and thoracic aorta
Courses to the left into the neck anterior to the vertebral artery and vein
Enters the junction of the left subclavian and the IJV

Lymphatic drainage (Level IV)Lymphatic drainage (Level IV)
Hypopharynx Larynx Thyroid Cervical esophagus

Lymphatic drainage (Level V )Lymphatic drainage (Level V )
Posterior triangle of neck Posterior border of SCM Clavicle Anterior border of trapezius Va Spinal accessory nodes Vb Transverse cervical arte
ry nodes Radiologic landmark: Inferior bor
der of Cricoid Supraclavicular nodes

Lymphatic drainage (Level V )Lymphatic drainage (Level V )
Nasopharynx, Oropharynx, Posterior neck and scalp

Lymphatic drainage (Level VI )Lymphatic drainage (Level VI ) Thyroid Larynx(glottic and subglottic) Pyriform sinus apex Cervical esophagus

A Neck MassA Neck Mass

Introduction Introduction
Neck masses are very common Inflammatory and infectious causes : cervic
al adenitis Congenital masses : branchial anomalies and th
yroglossal duct cysts
Neck masses resulting from trauma: hemato
mas firm masses because of fibrosis. Neoplasms (benign and malignant) Maligna
ncy is the greatest concern in a patient with a neck mass.

Normal AnatomyNormal Anatomy The central portion : the hyoid bone, t
hyroid cartilage, and cricoid cartilages, the thyroid gland .
Carotid arteries are pulsatile and can be quite prominent if atherosclerotic disease is present.
The sternocleidomastoid muscles should be palpated along their entirety

DiagnosisDiagnosis Normal variations in anatomy can be
distinguished from true pathology without the need for additional diagnostic testing
The only easy way to diagnose a neck mass is to know exactly what the patient has before you begin.
your only challenge is to prove it The next most challenging is to have some idea of
what the patient has, perform a few tests, narrow the differential, and then prove the final diagnosis.

DiagnosisDiagnosis
The patient's age and the size and duration of the mass are the most significant predictors of neoplasia
Malignancy is the greatest concern in a patient with a neck mass.

DiagnosisDiagnosis
The occurrence of symptoms and their durat
ion must also be determined. Acute symptoms, such as fever, sore throat, and coug
h, suggest adenopathy resulting from an upper respiratory tract infection.
Chronic symptoms of sore throat, dysphagia, change in voice quality, or hoarseness are often associated with anatomic or functional alterations in the pharynx or larynx.

Diagnostic StepsDiagnostic Steps History: A careful medical history can provide importa
nt clues to the diagnosis of a neck mass. Developmental time course Associated symptoms (dysphagia, otalgia, voice) Personal habits (tobacco, alcohol) Previous irradiation or surgery
Physical Examination Complete head and neck exam (visualize & palpat
e) Emphasis on location, mobility and consistency endoscopic evaluation, with possible excisional biopsy o
r neck dissection.


Fine needle aspiration biopsy Fine needle aspiration biopsy (FNAB)(FNAB)
Diagnostic yields reach as high as 90% for both infection and neoplasm.

Imaging techniquesImaging techniques Computed tomography (CT) or with
contrast Magnetic resonance imaging (MRI)
or with contrast Ultrasonography Nuclear scanning Positron emission tomography (PET)
the metabolic activity of the tissues


BiopsyBiopsy
Biopsy should be considered for neck masses with progressive growth, location within the supraclavicular fossa, or size greater than 3 cm.
Biopsy also should be considered if a patient with a neck mass develops symptoms associated with lymphoma. Frozen-section examination of the mass followed by neck dissection should be performed if the mass proves to be metastatic carcinoma.
The risk of having a malignant neck mass becomes greater with increasing age.

Lymph node groups with the most likely sites of the primary lesion.
Diagnosis Diagnosis (metastatic lymph node)(metastatic lymph node)

algorithm


Evaluation and management of a neck mass in the adult patient. (PPD = purified protein derivative)
Algorithm

ManagementManagement Many inflammatory lymph nodes resolve with
no treatment, although close observation is required.
A single course of therapy with a broad-spectrum antibiotic and reassessment in one to two weeks is a reasonable treatment choice when a patient with a neck mass has signs and symptoms of an inflammatory process (i.e., fever, painful mass, erythema) or a history of recent infection

ManagementManagement
Benign neoplasm: surgical treatment

Neck DissectionNeck Dissection

overviewoverview Anatomy
Nodal levels Common nodal drainage patterns
Staging Classification Sentinel Lymph Node

IntroductionIntroduction The neck dissection is a surgical procedure for co
ntrol of neck lymph node metastasis from squamous cell carcinoma (SCC) of the head and neck.
The aim of the procedure is to remove lymph nodes from one side of the neck into which cancer cells may have migrated.
The metastases may originate from SCC of the upper aerodigestive tract, including the oral cavity, tongue, nasopharynx, oropharynx, hypopharynx, and larynx, as well as the thyroid, parotid and posterior scalp.

IntroductionIntroduction
Lymph node metastasis reduces the survival rate of patients with squamous cell carcinoma by half.
The survival rate is less than 5% in patients who previously underwent surgery and have a recurrent metastasis in the neck.
Therefore, the control of the neck is one of the most important aspects in the successful management of these particular tumors.

AnatomyAnatomy Lymph Node Levels: To describe the lymph nodes of the neck
for neck dissection, the neck is divided into 6 areas called Levels

Common Nodal DrainageCommon Nodal Drainage
Level I: Chin, Lower lip, Anterior floor of mouth, Mandibular incisors, Tip of tongue, Oral Cavity, Floor of mouth, Oral tongue, Nasal cavity (anterior), Face
Level II: Oral Cavity, Nasal Cavity, Nasopharynx, Oropharynx, Larynx, Hypopharynx, Parotid
Level III: Oral cavity, Nasopharynx, Oropharynx, Hypopharynx,Larynx

Common Nodal DrainageCommon Nodal Drainage
Level IV: Hypopharynx, Larynx,
Thyroid, Cervical esophagus
Level V: Nasopharynx,
Oropharynx, Posterior neck and
scalp
Level VI: Thyroid, Larynx
(glottic and subglottic), Pyriform
sinus apex, Cervical esophagus

ClassificationClassification
Radical Neck Dissection (RND) Gold standard operation
Modified Radical Neck Dissection (MRND) Preservation of non lymphatic structures
Selective Neck Dissection (SND) Preservation of lymph node groups
Extended Neck Dissection Removal of additional lymph node groups or
non lymphatic structures

Radical Neck DissectionRadical Neck Dissection Removes
all ipsilateral cervical lymph node groups I-V
SCM, IJV, XI Submandibular gland, tail of parotid
Preserves Posterior auricular Suboccipital Retropharyngeal Periparotid Perifacial Paratracheal nodes

Modified Radical Neck DissectionModified Radical Neck Dissection
Removes Nodal groups I-V
Preserves SCM, IJV, XI (any c
ombination) Notate according to whi
ch structures are preserved

Selective Neck DissectionSelective Neck Dissection
Remove high risk lymph node groups based on tumor site.
For oropharyngeal, hypopharyngeal and laryngeal cancers, SND (II-IV) is the procedu
re of choice.

Extended Neck DissectionExtended Neck Dissection
To removal of one or more additional lymph node groups or nonlymphatic structures, or both, not encompassed by the RND
Notated by naming the structure(s) removed.

Operative TechniqueOperative Technique
Limited incision guided by lymphoscintigraphy and gamma probe
Frozen section analysis (incised margin )

ComplicationsComplications
Nerve injury: Shoulder dysfunction (the accessory nerve )
Vessel injury : Bleeding
Infections: Wound infections may also occur and can usually be managed in the clinic with antibiotics and minor wound care.

ComplicationsComplications
Lymphatic Leak Major lymph channels are encountered at the
lower aspect of the neck, especially on the left side.
Occasionally a lymphatic leak occurs despite these efforts.
Food in the stomach can increase the amount of lymphatic flow. A diet change and a pressure dressing can usually control this problem,
Return to the operating room for repair if necessary .

EmphasisEmphasis Anatomy features of the trachea and
physiology . What is tracheotomy? What is the
indications? What important structures in the neck? Esophageal three Constrictions. What are
the clinic significance?

EmphasisEmphasis
Two major triangles of the neck How many levels of Lymphatic
drainage of the neck Neck masses classification and
algorithm of diagnosis Classification of the neck dissection

无论遇到什么事,无论遇到什么事,我一定会支持你,绝对不让你掉下去。我一定会支持你,绝对不让你掉下去。
Thank you如果你感到郁闷,如果你也不开心,
那一定要告诉我。我要把所有的快乐和你一起分享,那你就把你的烦恼给我一半好了。