Wound ConstructionDr. Devin Prabhakar MS,DNB,FRCS

????????? WTR/ATR/None
In pseudophakia, low, simple, ATR myopic astigmatism is better than WTR astigmatism because it provides superior uncorrected near visual acuity.

What is WTR astigmatism?
This is when the axis of the +cylinder in a pair of glasses is at 90 degrees. WTR astigmatism is typically seen in children, ATR is seen in older eyes.

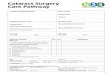
Astigmatism
With-theRule This is when the vertical meridian is
steepest. Against the-Rule
This is when the horizontal meridian is steepest.
Oblique This is when the steepest curve lies
in between 120 and 150 degrees and 30 and 60 degrees.

???? Limbus: Blue/White

Effect of Incision
Eventual flattening of surgical meridian
Longer Incision: Greater Flattening
Closer to corneal Apex: Greater Flattening

Incision
Site Position Shape Length


Temporal Incision
By Fine Less Manipulation No need for birdle suture Less Astigmatism Natural drainage of irrigating fluid Undergoes ATR Astigmatism Good red glow Good for topical anesthesia

Creating a scleral incision
Make a fornix-based conjunctival peritomy Make a shallow groove-incision in the sclera
(preferably frown), slightly larger than the width of your keratome,
Tunnel in the sclera. Move keratome to both sides. Advance the keratome in the cornea, going
slightly up-hill Having advanced up to clear cornea, tilt the
keratome so thatthe keratome’s tip points to the macula and cut through Descemet’s membrane
Once through Descemet’s membrane, advance the knife parallel to the iris-plane until the shoulders of the keratome have passed the internal edge of the incision.

Tips for creating incisions
Maintain appropriate pressure in anterior chamber.
Underpressure will lead to a tunnel that is too long and wound’s edges that are not straight
Overpressure will lead to a tunnel that is too short
When in doubt, perform a Seidel test with a fluorescein strip to test for leakage
Fixate the eye by grasping the conjunctiva at the limbus with forceps

Creating a clear corneal incision
Make a shallow straight groove-incision in the clear cornea, as large as the width of your keratome,
Place the tip of your keratome in the groove and advance the keratome through the corneal stroma, going slightly up-hill
Having advanced ± 2 mm in the cornea, tilt the keratome so that the keratome’s tip points to the macula and cut through Descemet’s membrane,
Once through Descemet’s membrane, advance the knife parallel to the iris-plane until the shoulders of the keratome have passed the internal edge of the incision








ON AXIS CATARACT INCISION AND OPPOSITE CCI
3.2 mm incision induces 0.25 to 0.50 D of astigmatism. Incision on the steep axis will lower the Pre Existing Astigmatism.
By adding an identical, penetrating Clear Corneal Incision opposite it is possible to correct about 1.0 to 4.0D of astigmatism.
No extra instruments or training.






Confusion Cleared
"The idea that you should leave a little WTR or ATR are old myths that come from articles written about 10 or 15 years ago," said Dr. Holladay. "It's not true. Residual astigmatism is like any other aberration. The best vision and the best result are with zero residual astigmatism. WTR or ATR are not beneficial. They blur the image, particularly if you don't wear glasses."

Please do join us on
www.facebook.com/DivyaPrabhaEyeHospital
www.facebook.com/devin.prabhakar
www.DivyaPrabha.in
Recommended