Letters
Where next with Loa loa encephalopathy? Data arebadly needed
Charles Mackenzie1, Timothy Geary2, Roger Prichard2 and Michel Boussinesq3
1 Filarial Diseases Laboratory, Michigan State University, East Lansing, MI 48824, USA2 Institute of Parasitology, McGill University, 21 111 Lakeshore Road, Ste-Anne de Bellevue H9X 3V9, Quebec, Canada3 Institut de Recherche pour le Developpement, Departement Societes et Sante, 213 rue La Fayette, 75480 Paris Cedex 10, France
Update TRENDS in Parasitology Vol.23 No.6
Loa loa encephalopathy, a serious adverse event (SAE)that is associated with the administration of ivermectin(IVM) when treating this infection, has remained both apathophysiological conundrum and a programmaticimpediment to mass treatment for over a decade. Weagree that: (i) the risk of developing an SAE is relatedto the pretreatment microfilarial load of L. loa; (ii) aproportion of individuals do not develop an SAE despitepresenting with a high microfilaremia; (iii) uncharacter-ized cofactors might have a role in the appearance of theneurological condition; and (iv) these cofactors could berelated to the host genotype or to other host factors, suchas coinfections that might produce inflammatorydamages at the level of the brain capillaries. The reasonsbehind the incomplete understanding of the pathophy-siology of this unfortunate situation are, perhaps, typicalof many emerging conditions that exist in medicallyunderdeveloped (and frequently rural and isolated) popu-lations and can be traced to a lack of integrated researchon the syndrome. The recent discussions of this serious,central nervous system (CNS) condition by two authorswith different perspectives [1,2] have underscored theinadequate status of knowledge regarding the pathogen-esis of this encephalopathy and also underline the lack ofknowledge about the actions of IVM and its use in treat-ment of filariases (to say nothing of other antifilarial andanthelmintic drugs).
Keeping an open mind regarding the pathogenesis ofL. loa encephalopathy is the only approach that is judi-cious at present, given that few data are available, especi-ally at the tissue level – there are data from only onelimited autopsy on an individual who died almost eightweeks after treatment (J. Kamgno et al., unpublished).Many unanswered questions remain about this condition,including the reason for the apparent clustering of casesin Africa, which might be because of the intensity of L. loamicrofilaremia. The seriousness of encephalopathy inclinical terms is supported by the fact that this para-site-related condition seems not to be simply an acutephenomenon; instead, some of the sufferers remain per-manently compromised in terms of CNS function.
At the programmatic level, the risk of developingencephalopathy is a major impediment to the expansionand completion of mass drug administration (MDA)
Corresponding author: Mackenzie, C. ([email protected]).Available online 24 April 2007.
www.sciencedirect.com
programs in loiasis-endemic areas and sensible, ethicaland effective managerial policies for introducing IVM tothese areas are urgently needed.
The ideas put forward in the original article [1], theresponse to it [2] and in other review articles (see, forexample, Ref. [3]), cover, by virtue of the current paucity ofdata, a wide range of opinions and ideas from scientistswith different experiences. Sorting out these opinions anddetermining the actual pathogenesis and necessary stepsto ensure the maintenance of antifilarial programmesurgently needs attention, as does the collection ofmaterialand more-detailed clinical data from new cases. Specialattention should be devoted to making sure that data aresystematically collected on possible coinfections or otherconcomitant conditions. Activities such as core needleCNS biopsies that leave the body free of external damage(and are, thus, more acceptable to relatives), along withquicker transition to tertiary medical observation andcare for affected individuals, are important pathways toenhance the collection of much needed data and tissuesamples.
Scientists and physicians from both clinical and basicresearch backgrounds must collaborate to address thisclinically and programmatically important phenomenon.To begin the analysis of the possible roles of host-genomefactors to the development of post-IVM SAEs, research-ers have agreed to collaborate to characterize thesequence integrity and expression of multidrug resist-ance (MDR)-1 proteins in affected and unaffected indi-viduals. This project should be able to rule out (or in) thegenetically determined contribution of IVM access tothe brain in this syndrome. If the findings indicate thatthe mdr-1 genotype might predict sensitivity to IVM,researchers will then need to explore possible appli-cations to field-based medical management, whichinvolve genome-level testing (which will not be easilyaccomplished in situ). Indeed, it could be that theapproaches to managing this condition will require theinstigation of further premass treatment (MDA) pro-cedures. This would, of course, increase the cost ofMDA for filarial infections but is likely to be a worth-while cost for the continuance of such antifilarial pro-grams. Interpretations and decisions need to be based ondata. The collaboration of researchers to obtain data onthe interaction of IVM and the host in encephalopathycases is intended to clarify the underlying causes for thiscondition.

238 Update TRENDS in Parasitology Vol.23 No.6
References1 Geary, T.G. (2005) Ivermectin 20 years on: maturation of a wonder
drug. Trends Parasitol. 21, 530–5322 Boussinesq, M. et al. (2006) What are the mechanisms associated
with post-ivermectin serious adverse events? Trends Parasitol. 22,244–246
Corresponding author: Parkinson, M. ([email protected]).Available online 11 April 2007.
www.sciencedirect.com
3 Mackenzie, C.D. et al. (2003) Possible pathogenic pathways in theadverse clinical events seen following administration of ivermectinto onchocerciasis patients. Filaria J. 2, S5
1471-4922/$ – see front matter � 2007 Elsevier Ltd. All rights reserved.
doi:10.1016/j.pt.2007.04.007
Controlling fasciolosis in the Bolivian Altiplano
Michael Parkinson1, Sandra M. O’Neill2 and John P. Dalton3
1 School of Biotechnology, Dublin City University, Glasnevin, Dublin 9, Ireland2 School of Nursing, Dublin City University, Glasnevin, Dublin 9, Ireland3 Institute for the Biotechnology of Infectious Diseases, University of Technology Sydney, Ultimo, Sydney, NSW 2071, Australia
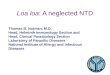
Figure 1. Infection rates of fasciolosis in the Bolivian Altiplano. Infection rate is
Liver fluke disease, or fasciolosis, is a global problem oflivestock and causes losses of US$3 billion annually [1].Recently, it has emerged as a major health problem inmany countries, including Iran, Peru, Cuba, Bolivia andEgypt. Every year an estimated 2.4 million people areinfected worldwide and a further 180 million people areat risk of infection [1]. The highest prevalence of fasciolosisin humans is found in the Altiplano region of northernBolivia [2,3]; this article highlights the need for a controlstrategy in this region. The disease causes serious illhealth with extensive haemorrhaging and inflammationof the liver, and thickening and dilation of the bile ductsand gallbladder.
In the Bolivian Altiplano, the zone of high infection inhumans stretches >30 km along the narrow corridor ofBatallas from Lake Titicaca to La Paz [2] (Figure 1). Theareas with the highest prevalence of fasciolosis in humans(reaching 60%) are also those with high animal (25% cattleand 70% sheep) infection [4,5]. In most regions of the Alti-plano, animal pasturing is free and this leads to infectedanimals contaminating pastures andwater sources that areused by humans. Fluke eggs released by infected mammalshatch and then formmiracidia, which invade the snail hostand subsequently develop to erupt as free-swimming cer-cariae. These cercariae settle and encyst on vegetation orremain on the water surface to form metacercaria that areinfectious to mammals when ingested.
The Altiplano consists of poor rural communities ofsubsistence farmers who rely on the land and their live-stock to survive and have somewhat primitive farm-man-agement practices, which are unlikely to change inthe near future. Although the use of molluscicides andthe elimination of snail habitats have been successful insome trematode control programs, such as the control ofschistosomiasis in China [6], they would be too costly,labour intensive and logistically difficult to use in theBolivian Altiplano, where precipitation is high and snailslive over a broad area. A fasciolosis-control programmemust, therefore, focus on flukicide drug treatment andeducation.
Infection is highly age related, with the highestprevalence in children between eight and eleven yearsold [2,4]. Children of this age commonly work in the fieldsminding livestock and are more likely than adults toacquire infection through habitually eating aquatic plantsand by drinking water from sources that are contaminatedwith metacercariae [1,4]. Accordingly, drug treatmentshould be particularly focused towards children inhigh-risk areas (local schools being a focal point). Thiscould be effective alongside a health-education programmethat delivers the correct message on how fasciolosis isspread from animal to human and that links the diseaseand the resulting illness [7]. Treatment with the flukicidetriclabendazole is the most effective means for clearingliver fluke infection in cattle, sheep and humans (althoughit is not yet registered for human use in Bolivia) [4]. Se-lective chemotherapy of humans with triclabendazole overa four-year period has been effective in reducing the preva-lence of fasciolosis in humans in the Nile delta, Egypt [8].With the support from government and local health
related to the size of the circle: black circles indicate an infection rate of 10–61.5%
and red circles indicate an infection rate of <10%. Green shading indicates level
areas of the Altiplano and brown shading indicates elevated regions. Scale
bar = 10 km.
Recommended