What’s new in emergency care? Dr Sally McCarthy Medical Director ECI
ECI Emergency Care Symposium Friday 8 November 2013

Stakeholder survey 2013

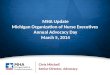
Rural metropolitan split (responses compared to presentations)
63% 60% 64%
30% 34% 36%
7% 6%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2013 2012 2012/13 patient volume
Unknown
Rural
Met

ED delineation level (responses compared to presentations)
0.4% 3% 3% 9%
15% 9%
15%
12% 22%
12%
21% 23% 21%
14%
19%
36% 30%
25%
7% 6%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
2013 2012 2012/13 patientvolume
Unknown
6
5
4
3
2
1

What are the ‘top’ challenges for your Emergency Department today? 39%
29% 27%
26% 23%
20% 18%
16% 13% 13%
12% 10% 10%
9% 9%
7% 6% 6% 6%
Access blockIncreased demand for services
Inefficient hospital systems/poor…Introduction of NEAT
Lack of staffOvercrowding
Lack of senior cliniciansTransfer of patients
Mental healthHealth bureaucracy
Ageing populationLack of resources
Recruitment and retentionLack of education / professional…Patient and public expectations
Waiting timesVariations in care
OthereMR

Top challenges – comparison of 2013 to previous

Top challenges – Metro and Rural

Top challenges – emergency service role delineation

How much do you know about the NSW ECI (2012 compared to previous)?
6% 14%
34%
7%
12%
21%
38%
36%
33% 40%
31%
10% 10% 7% 2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2013 2012 2011
A lot
A fair amount
Not very much
Heard of butknow nothing atall

41%
40%
39%
37%
31%
22%
33%
37%
37%
34%
25%
17%
Standardised reporting of information accessibleto the whole of the hospital
Patient focus
Strong and visible leadership
Quality improvement focus on care
Use of diagnostic and project managementmethodology
Support structures for sites and executives
2013
2012
% of respondents
Implementation of NEAT – activities that were evident

Implementation of NEAT – activities that were evident by staff group 49%
45%
40%
47%
33%
30%
33%
31%
33%
25%
28%
13%
Standardised reporting of information accessible to the whole of the hospital
Patient focus
Strong and visible leadership
Quality improvement focus on care
Use of diagnostic and project management methodology
Support structures for sites and executivesNursing Medical
% of respondents

Implementation of NEAT/WOHP – initiatives introduced
37%
29%
25%
16%
14%
13%
13%
12%
8%
ED right to admit policy implementation
ED navigator role
Team-based ED care
Length Of Stay outlier management
Patient journey boards
Diagnostic mapping
Overcensus on wards
Ward reconfiguration
Weekend discharge management
% of respondents

Where do staff go for information about emergency care
51%
50%
41%
40%
33%
33%
6%
5%
37%
48%
38%
31%
23%
20%
6%
7%
84%
50%
29%
14%
17%
11%
0%
Emergency Care Institute (ECI)
NSW Ministry of Health
College or ProfessionalAssociation
Clinical Excellence Commission(CEC)
Agency for Clinical Innovation(ACI)
Health Education and TrainingInstitute (HETI)
Interstate emergency networks(e.g. Victoria)
Bureau of Health Information(BHI)
2013
2012
2011
% of respondents

What’s happened in 2013?


Education • ECI skills workshops: Orange, Albury • ECI moodle site: dental, NDEC suite, radiology, EZI IO,
procedures • The Best from the Best

Review and change • PECC review implementation in early stages • Surgery for children: referral arrangements; designated
hospitals. Await release. • Advance Planning for Quality Care at End of Life
Framework, NSW Health released: implementation has commenced

Whole of Hospital Program Activity at 23 sites

Work in progress Firstnet remediation program All the committee work

15%
35%
46%
48%
51%
51%
73%
0% 20% 40% 60% 80%
Other
Needing to log out…
Volume of other…
Poor/no wireless…
Slow…
Lack of…
Blocking…
Percentage of respondents
Gap assessment Q20 Barriers to internet access
ECI Survey of Internet Use in Emergency Departments 2013

Research • Evidence into practice research prizes ACEM and CENA 2032 annual
congress
• ECI presentations and posters at CENA, ACEM, RCC and other conferences

Projects Roll out of ACE project completed (*ECI symposium innovation
presentation 2011)
Implementation of ACEM quality framework: 23/ 24 sites • Appropriate test ordering • Morbidity and mortality review • Many other projects Commencing advocacy to support QSO position retention

Nurse Delegated Emergency Care
• Based on “The Walcha Model”
• Framework offering standardised, delegated care by nurses for low risk / low acuity, unscheduled care, patients
• Delineated and robust patient inclusion and exclusion criteria
• Episodic care by accredited RNs through: • Nursing Management Guidelines • Standing Orders • Documentation templates • Discharge and follow-up procedures
• Scheduled follow-up with GP
• Follow-up phone call from RN within 24 hours of presentation

Nurse Management Guidelines •Burns (minor) •Ear ache •Eye problems •Foreign bodies •Head injuries •Insect bites •Limb injuries •Pain (any cause) •Rash •Respiratory type illness •Tick bite •Urinary Symptoms •Vomiting and diarrhoea •Wounds •Marine Creatures

July August September October June Nov - Dec
Steering Committee formed
NDEC Suite Review & Site Expression
of Interest received
NDEC Suite finalised. First tranche sites
notified
First tranche site implementation
commences
NDEC commences at implementation sites
NDEC suite further reviewed
& finalised

Look out for… Workforce literature review and directions
document

Will this change your practice? Limm EL et al. Ann Emerg Med. 2013 Nov;62(5):521-5. doi: 10.1016/j.annemergmed.2013.02.022.
Epub 2013 Apr 23.
Half of all peripheral intravenous lines in an Australian
tertiary emergency department are unused: pain with no gain?
STUDY OBJECTIVE: Our study aims to determine the incidence of unused peripheral intravenous cannulas inserted in the
emergency department (ED). METHODS: A retrospective cohort study using a structured electronic medical record review was performed in a
640-bed tertiary care hospital in Melbourne, Australia. RESULTS: Fifty percent of peripheral intravenous cannulas inserted in the ED were unused. Forty-three percent
of patients admitted to the hospital with unused peripheral intravenous cannulas in the ED continued to have them unused 72 hours later.

Will this change your practice? First do no harm: In fact, first do nothing, at least not a cannula Diana Egerton-Warburton1,2, Sue Ieraci3 Article first published online: 1 AUG 2013 DOI: 10.1111/1742-6723.12109 Emergency Medicine Australasia

Level 4, Sage Building, 67 Albert Avenue, PO Box 699 T 02 9464 4675 www.ecinsw.com.au
Chatswood NSW 2067 Chatswood NSW 2057 F 02 9464 4728 ABN 89 809 648 636
www.ecinsw.com.au
Recommended