Venous thrombosis, Manifestations, Diagnosis and
TherapySam Schulman, MD
Incidence of VTE
• Estimated to affect 350,000 to 600,000 Americans annually
• Contributing to at least 100,000 deaths per year
• Will increase with ageing population

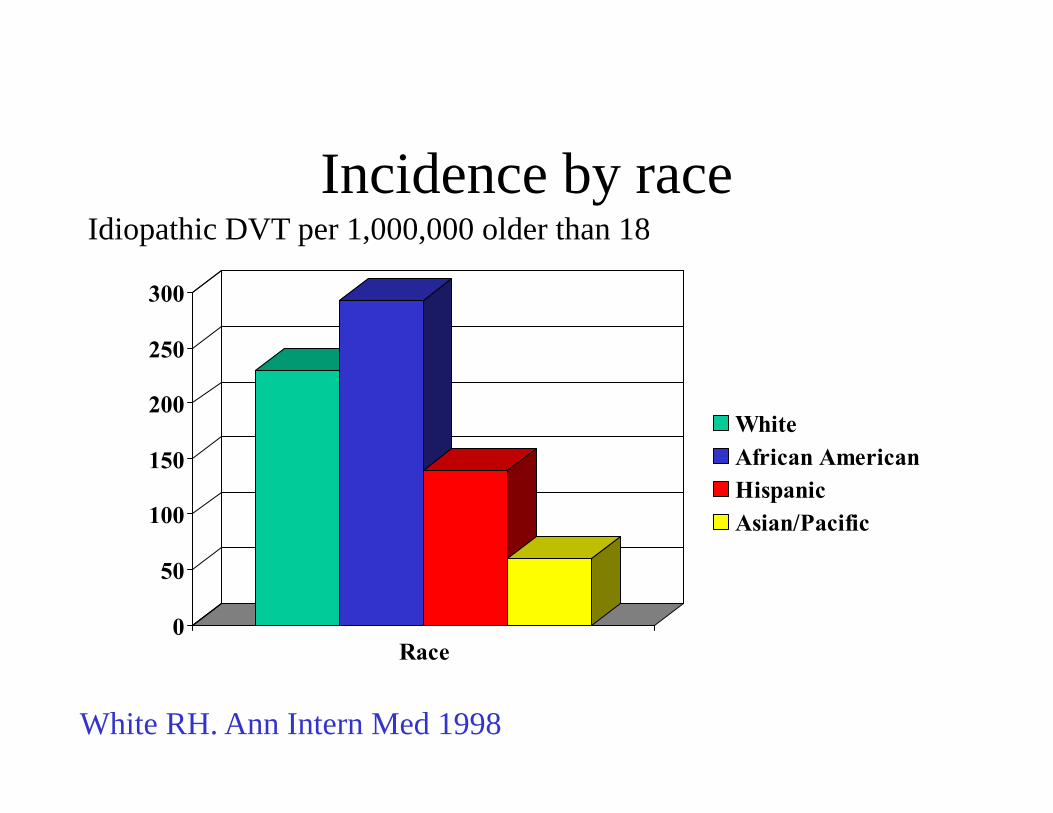
Incidence by race
0
50
100
150
200
250
300
Race
WhiteAfrican AmericanHispanicAsian/Pacific
Idiopathic DVT per 1,000,000 older than 18
White RH. Ann Intern Med 1998
Copyright ©2003 American Heart Association
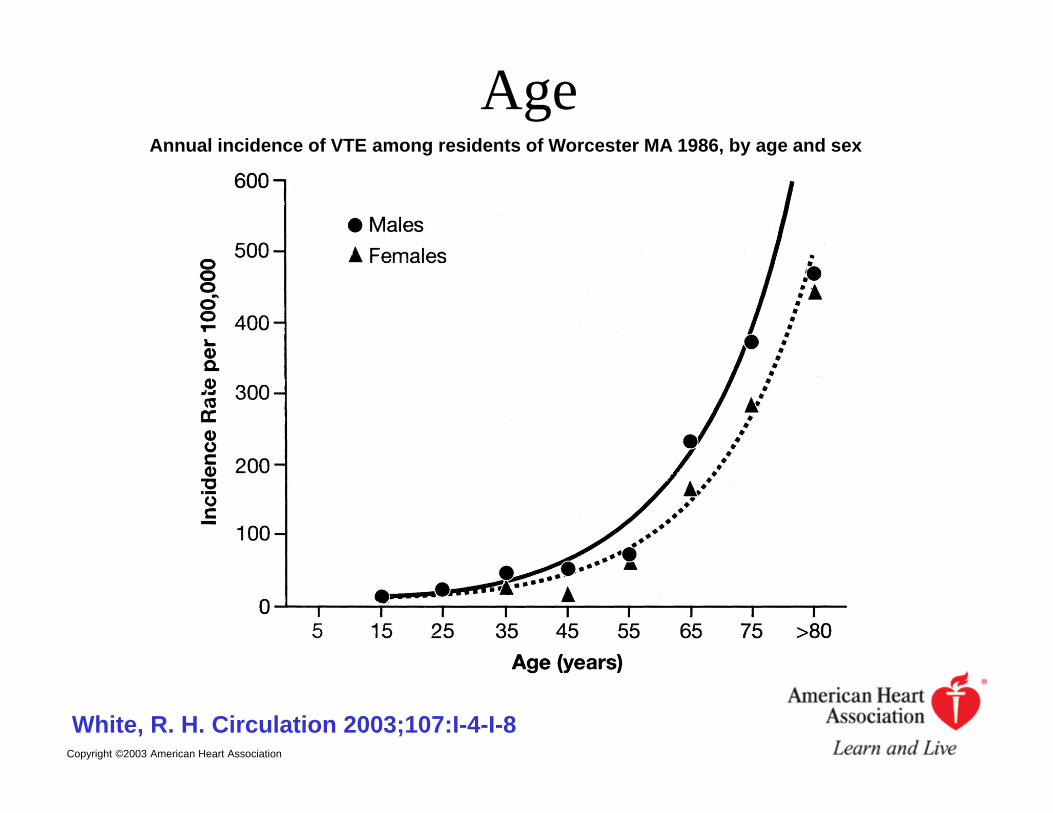
White, R. H. Circulation 2003;107:I-4-I-8
Annual incidence of VTE among residents of Worcester MA 1986, by age and sex
Age
Sex
• Worcester: No signif difference• Young age: more women; old age: more
men (Silverstein and others)
• California database: women 78 and men 63 per 100,000
Copyright ©2001 BMJ Publishing Group Ltd.
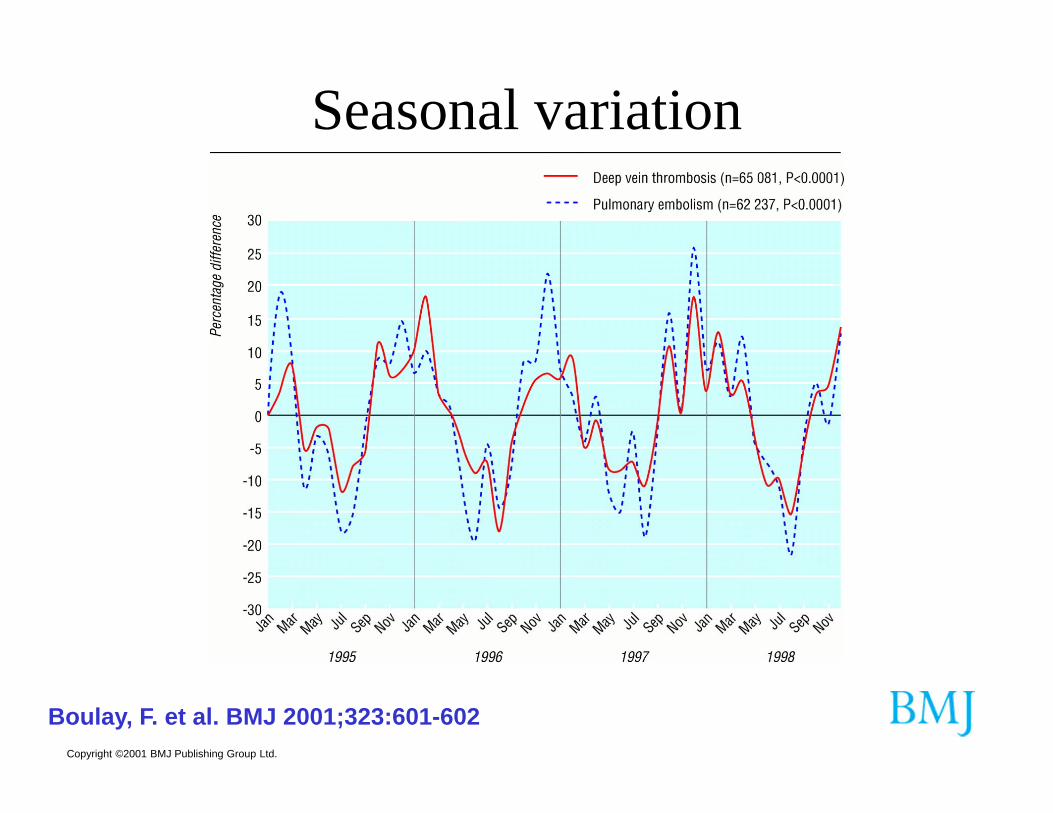
Boulay, F. et al. BMJ 2001;323:601-602
Seasonal variation
Metabolic syndrome• Of all components in the metabolic
syndrome abdominal obesity is the only component significantly associated with VTE (LITE-study and Tromsø Study)
Steffen LM et al. J Thromb Haemost 2009;7:746-51. Borch KH et al. J Thromb Haemost 2009;7:739-45.
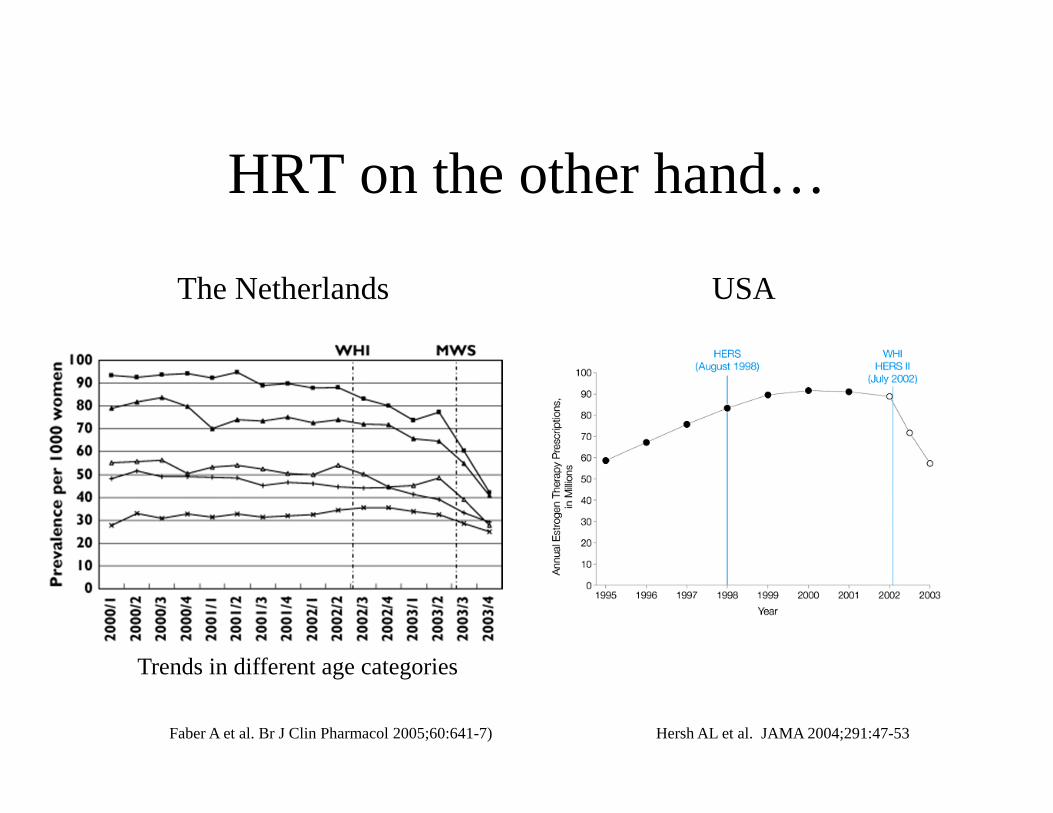
HRT on the other hand…
The Netherlands
Trends in different age categories
USA
Hersh AL et al. JAMA 2004;291:47-53Faber A et al. Br J Clin Pharmacol 2005;60:641-7)
And smoking
• Danish registry study 1993-97 (n=57,000) with adjustments for sex, alcohol, BMI, physical activity and HRT.
• HR females: 1.52 (95% CI, 1.15-2.00)• HR males: 1.32 (95% CI, 1.00-1.74)
Severinsen MT et al. J Thromb Haemost 2009;7:1297-1303
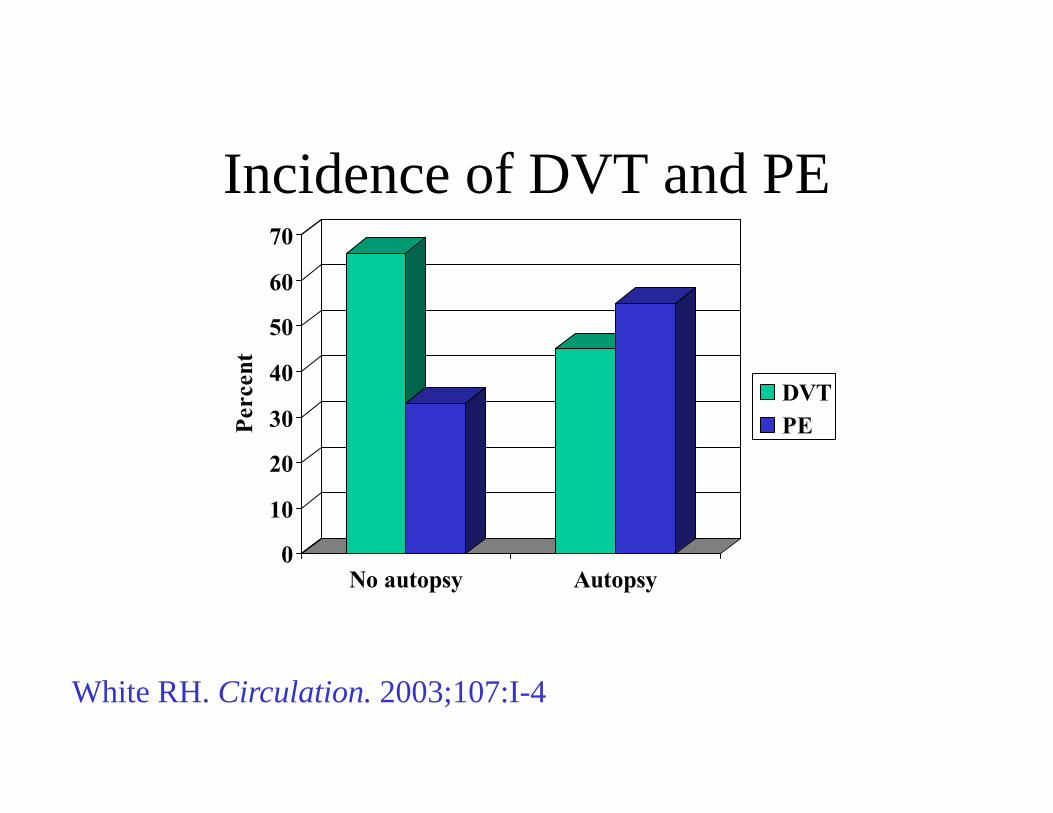
Incidence of DVT and PE
0
10
20
30
40
50
60
70Pe
rcen
t
No autopsy Autopsy
DVTPE
White RH. Circulation. 2003;107:I-4
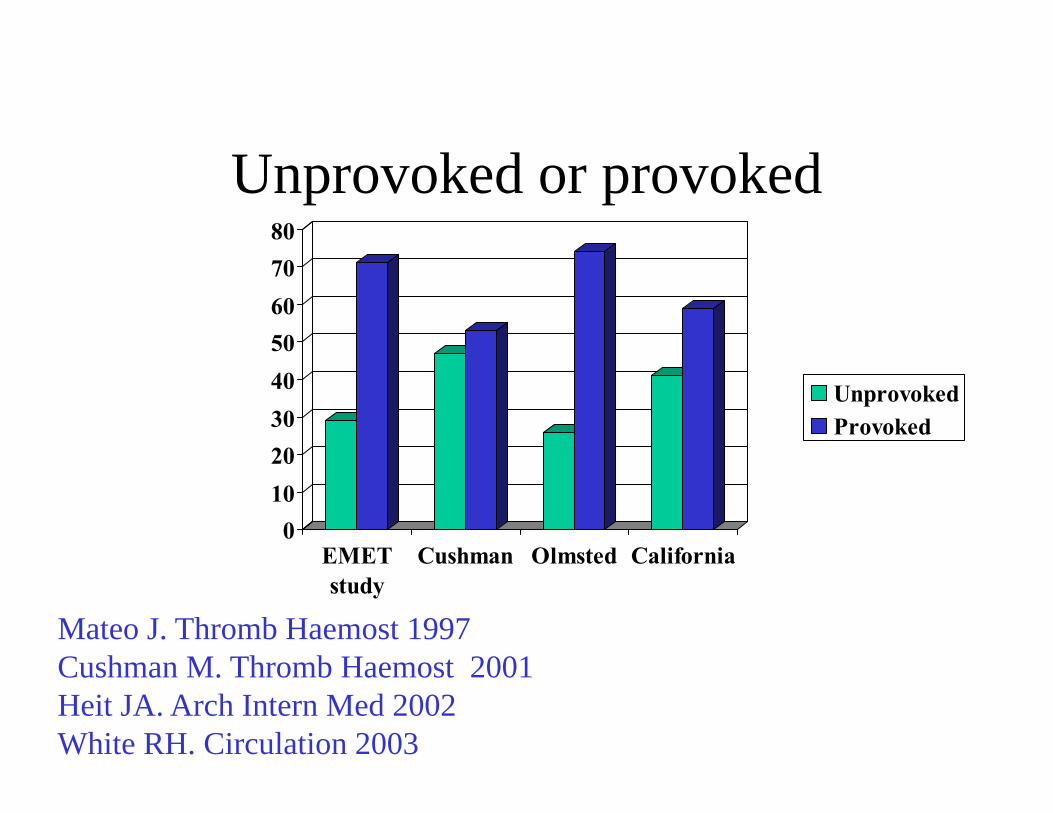
Unprovoked or provoked
Mateo J. Thromb Haemost 1997Cushman M. Thromb Haemost 2001Heit JA. Arch Intern Med 2002White RH. Circulation 2003
01020304050607080
EMETstudy
Cushman Olmsted California
UnprovokedProvoked
Hospitalized vs outpatient
• Worcester community-based study: 1,897 with validated VTE.
• 73.7% developed VTE as outpatients.• 27% occurred in patients already hospitalized for
other disease.
Spencer FA. Thromb Haemost 2008 & 2009.
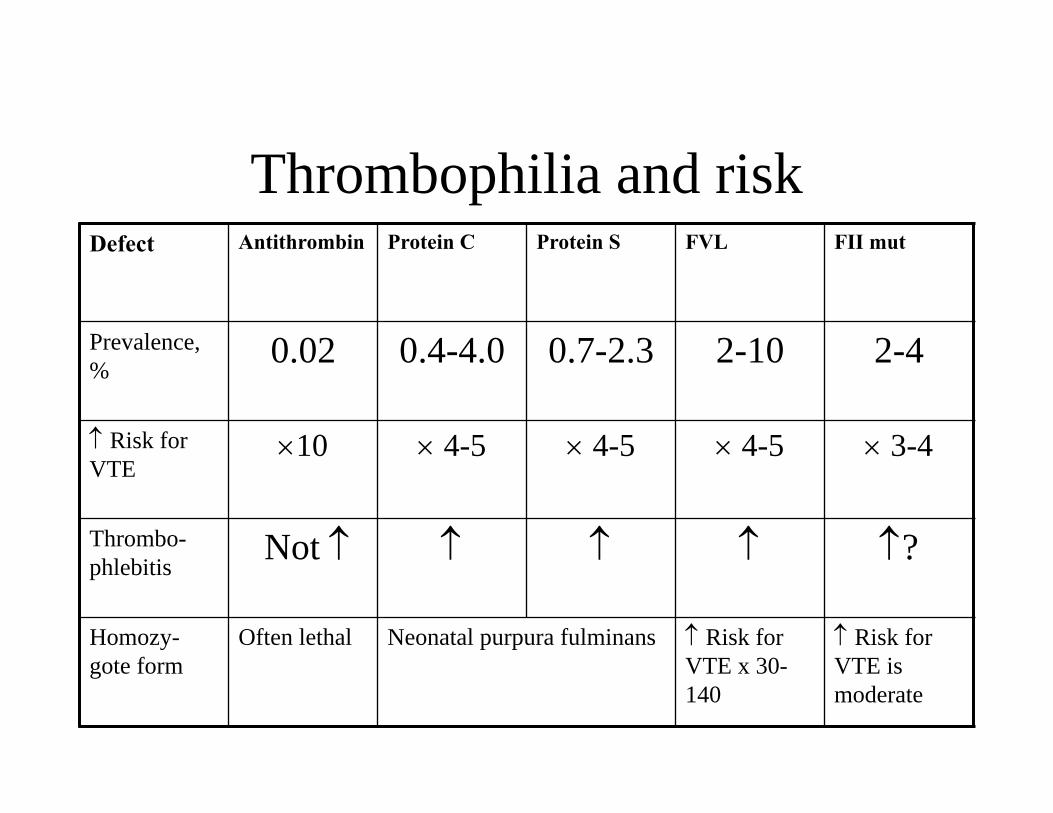
Thrombophilia and riskDefect Antithrombin Protein C Protein S FVL FII mut
Prevalence, %
0.02 0.4-4.0 0.7-2.3 2-10 2-4
Risk for VTE
10 4-5 4-5 4-5 3-4
Thrombo-phlebitis
Not ?
Homozy-gote form
Often lethal Neonatal purpura fulminans Risk for VTE x 30-140
Risk for VTE is moderate
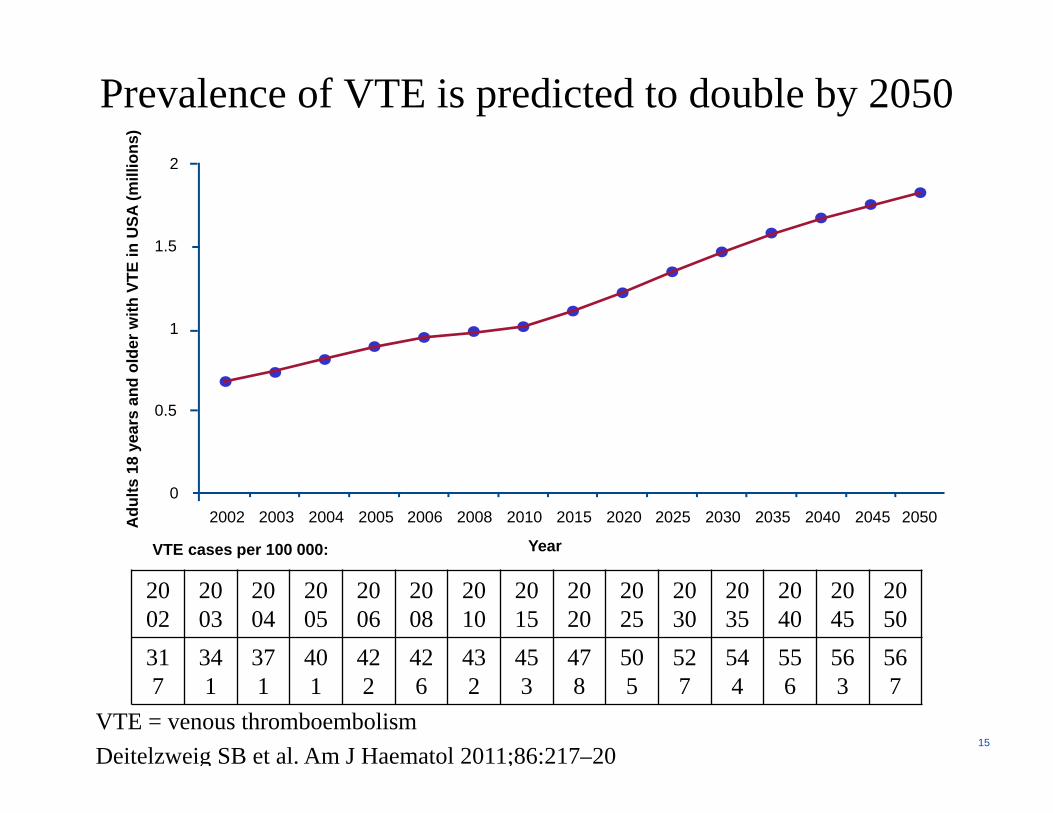
Prevalence of VTE is predicted to double by 2050
VTE = venous thromboembolismDeitelzweig SB et al. Am J Haematol 2011;86:217–20
15
YearVTE cases per 100 000:
2002
2003
2004
2005
2006
2008
2010
2015
2020
2025
2030
2035
2040
2045
2050
317
341
371
401
422
426
432
453
478
505
527
544
556
563
567
Adu
lts 1
8 ye
ars
and
olde
r with
VTE
in U
SA (m
illio
ns)
0
0.5
1
1.5
2
2002 2003 2004 2005 2006 2008 2010 2015 2020 2025 2030 2035 2040 2045 2050
Typical case
• 36 y.o. lady with pain in the R calf x 3d• Previously healthy• Went for a long walk last weekend• Was on COC for 10 years, stopped at age
28, restarted 3 months ago.• Physical: Tender calf, no edema or SOB
DVT – most common symptoms
• Deep leg pain• Unilateral swelling• Increased temperature, tenderness, redness• Phlegmasia cerulea dolens
– Severe pain, cyanosis• Phlegmasia alba dolens
– Severe pain, edema, pallor

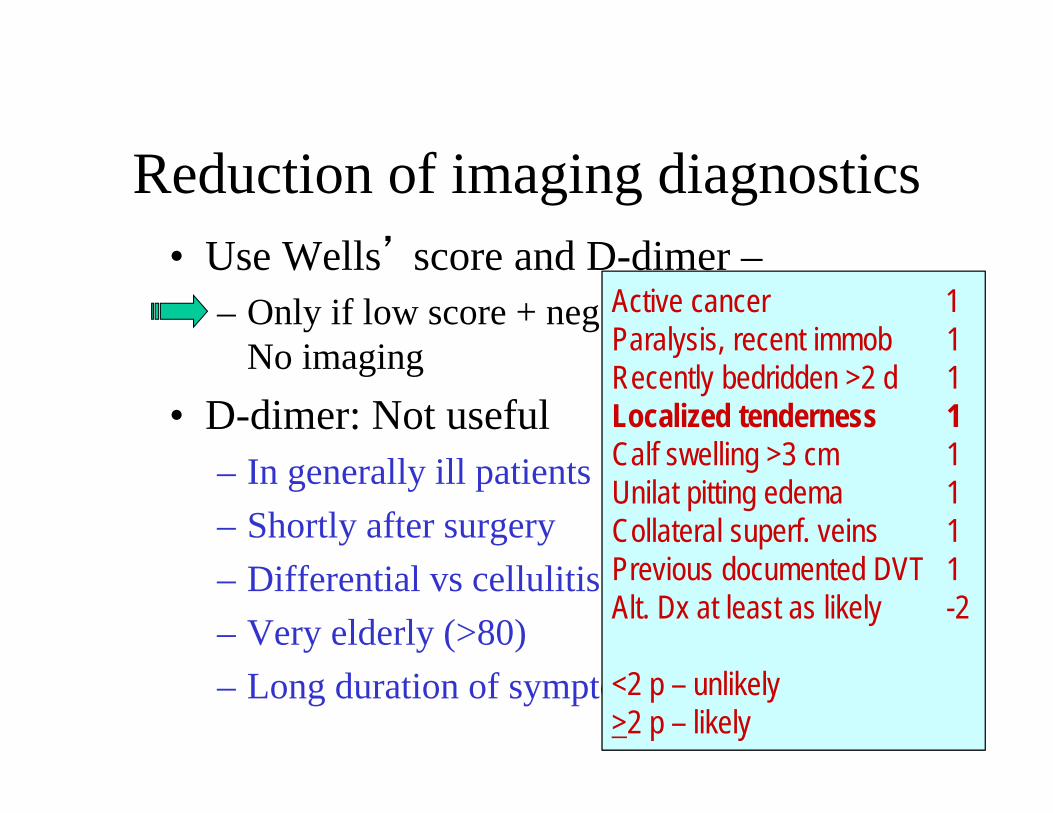
Reduction of imaging diagnostics• Use Wells’ score and D-dimer –
– Only if low score + neg D-dimer will result in No imaging
• D-dimer: Not useful– In generally ill patients– Shortly after surgery– Differential vs cellulitis– Very elderly (>80)– Long duration of symptoms
Reduction of imaging diagnostics• Use Wells’ score and D-dimer –
– Only if low score + neg D-dimer will result in No imaging
• D-dimer: Not useful– In generally ill patients– Shortly after surgery– Differential vs cellulitis– Very elderly (>80)– Long duration of symptoms
Active cancer 1Paralysis, recent immob 1Recently bedridden >2 d 1Localized tenderness 1Calf swelling >3 cm 1Unilat pitting edema 1Collateral superf. veins 1Previous documented DVT 1Alt. Dx at least as likely -2
<2 p – unlikely>2 p – likely
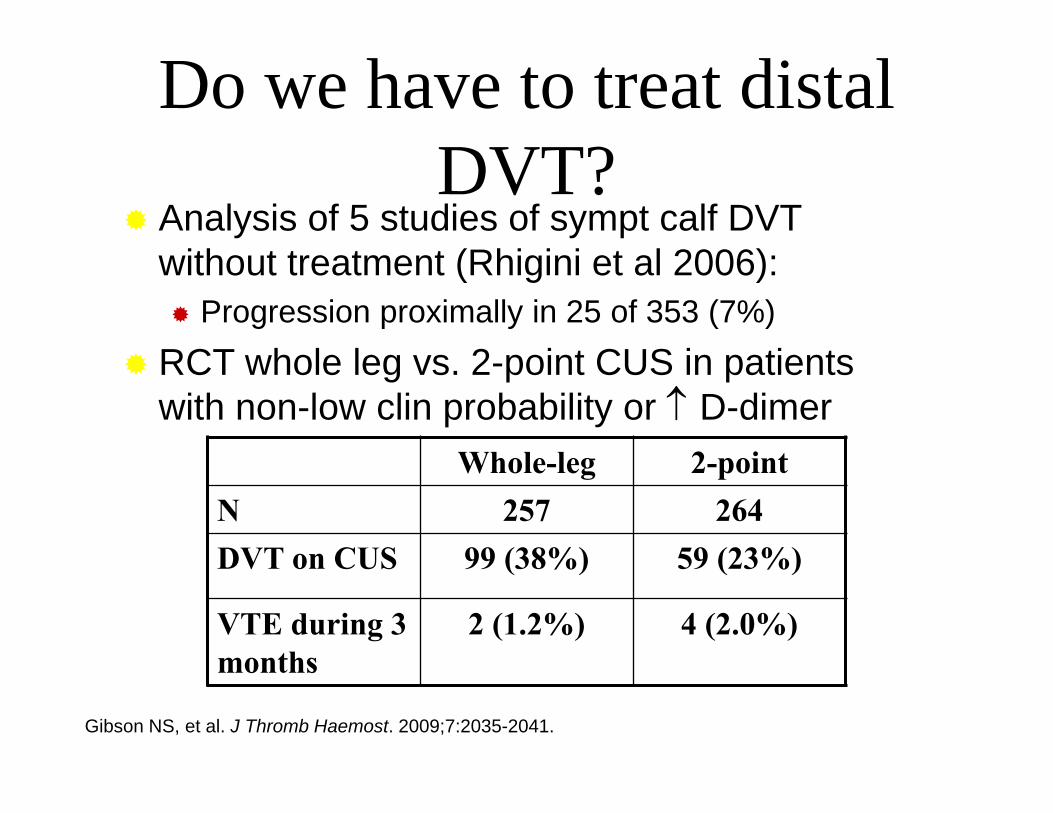
Analysis of 5 studies of sympt calf DVT without treatment (Rhigini et al 2006): Progression proximally in 25 of 353 (7%)
RCT whole leg vs. 2-point CUS in patients with non-low clin probability or D-dimer
Whole-leg 2-pointN 257 264DVT on CUS 99 (38%) 59 (23%)
VTE during 3 months
2 (1.2%) 4 (2.0%)
Gibson NS, et al. J Thromb Haemost. 2009;7:2035-2041.
Do we have to treat distal DVT?
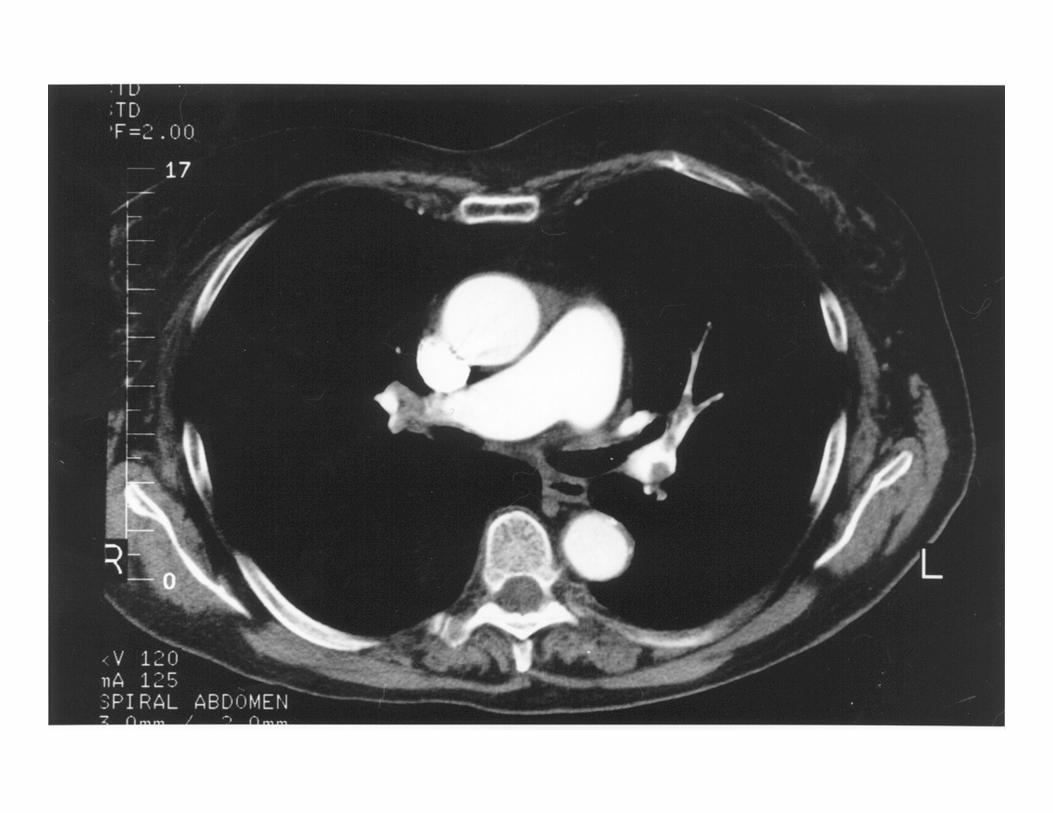
PE – most common symptoms
• Pleuritic pain 65%• Dyspnea 20%• Syncope 10%• Hemoptysis – fewDifferentialsRTI, MI, pericarditis, musculoskeletal
disorders …
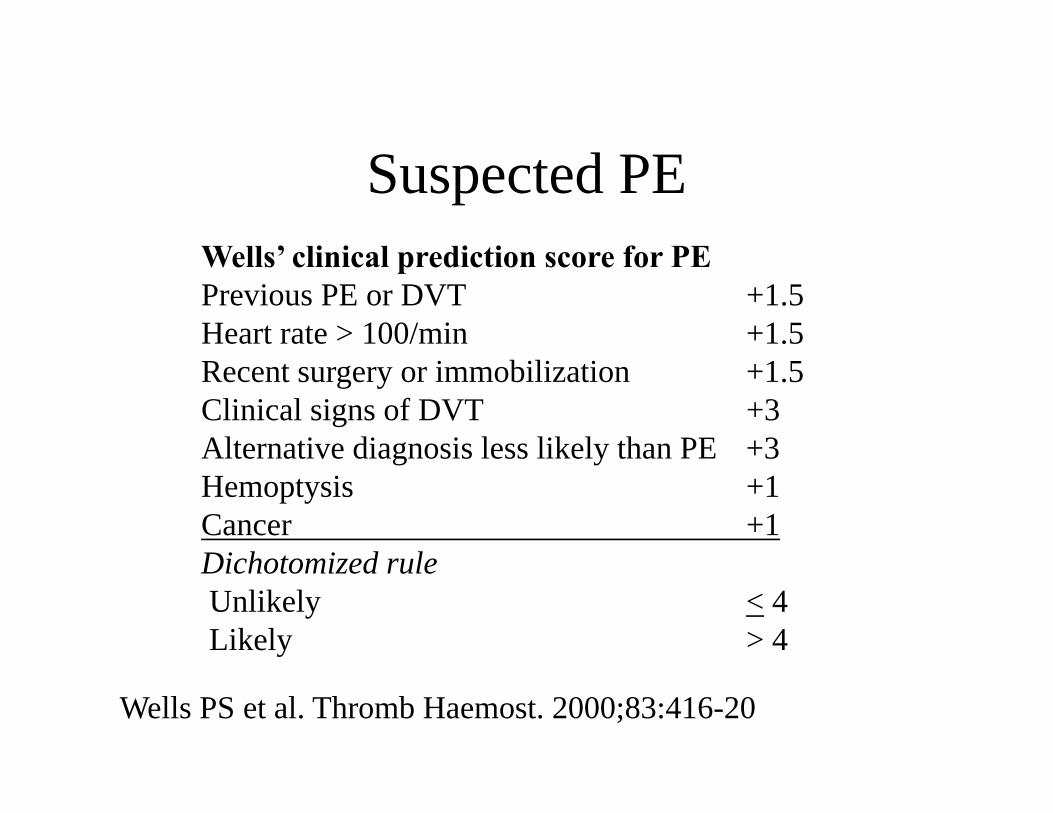
Suspected PEWells’ clinical prediction score for PEPrevious PE or DVT +1.5Heart rate > 100/min +1.5Recent surgery or immobilization +1.5Clinical signs of DVT +3Alternative diagnosis less likely than PE +3Hemoptysis +1Cancer +1Dichotomized ruleUnlikely < 4Likely > 4
Wells PS et al. Thromb Haemost. 2000;83:416-20
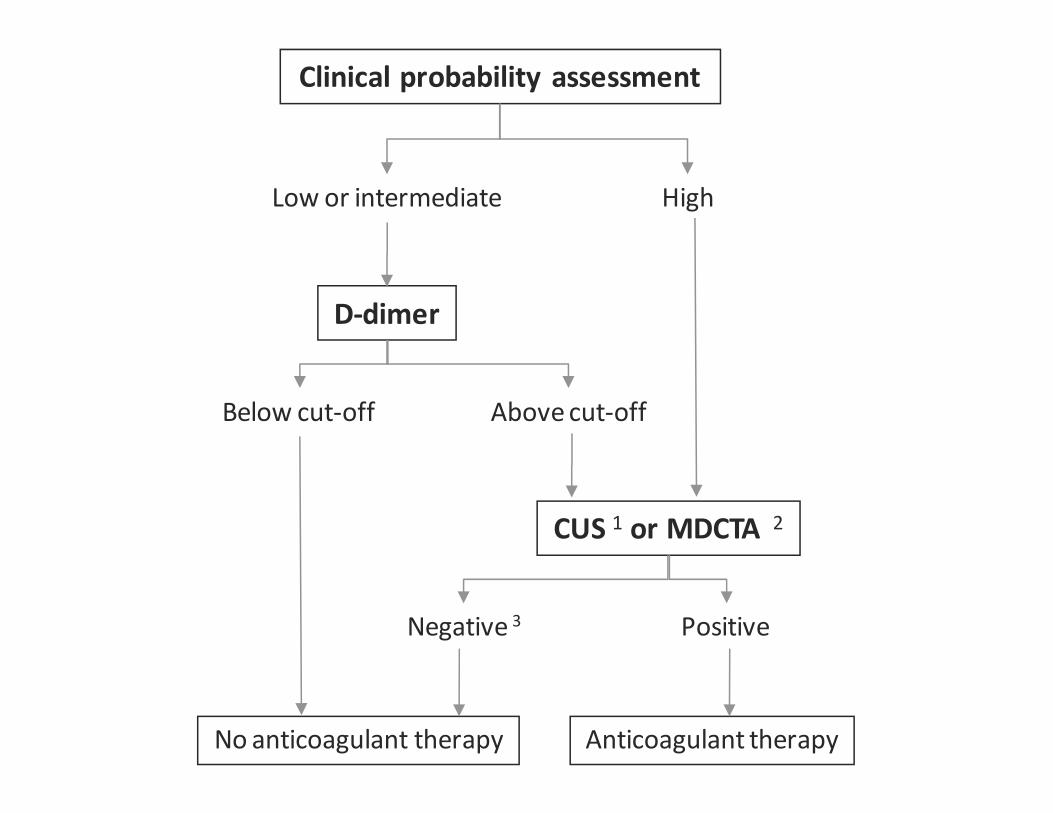
Clinical probability assessment
Low or intermediate High
D‐dimer
Below cut‐off Abovecut‐off
CUS 1 or MDCTA 2
Negative 3 Positive
No anticoagulant therapy Anticoagulant therapy
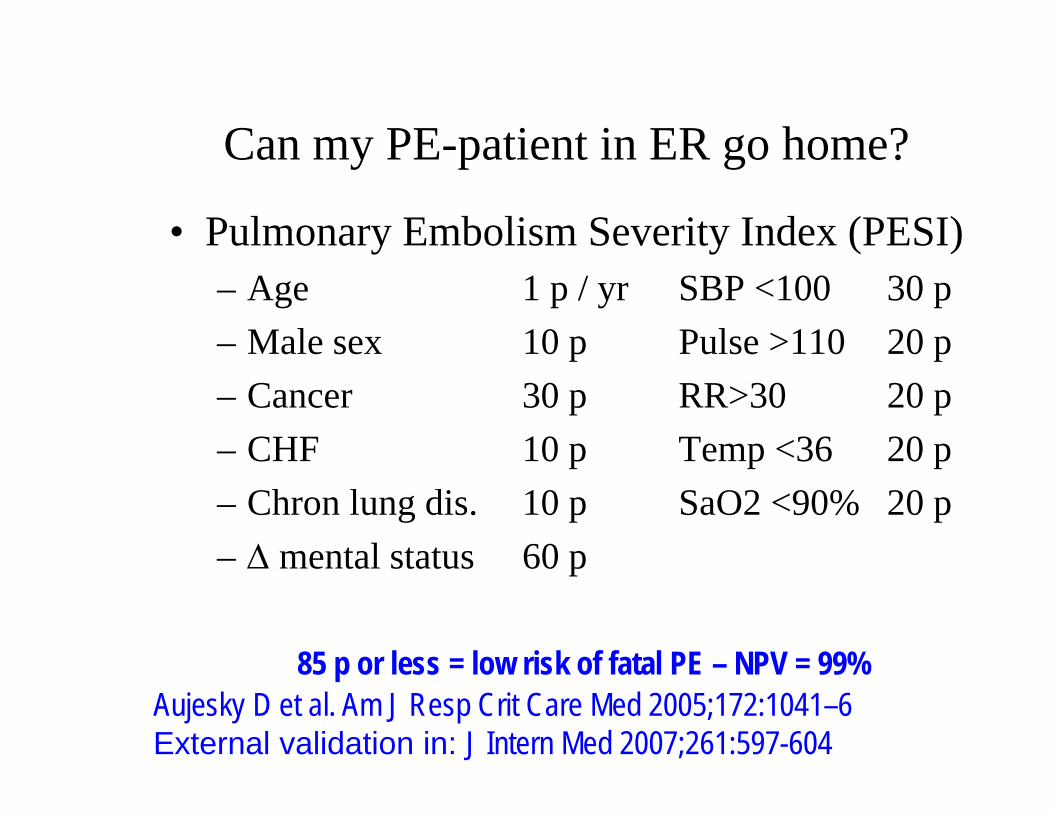
Can my PE-patient in ER go home?
• Pulmonary Embolism Severity Index (PESI)– Age 1 p / yr SBP <100 30 p– Male sex 10 p Pulse >110 20 p– Cancer 30 p RR>30 20 p– CHF 10 p Temp <36 20 p– Chron lung dis. 10 p SaO2 <90% 20 p– mental status 60 p
Aujesky D et al. Am J Resp Crit Care Med 2005;172:1041–6External validation in: J Intern Med 2007;261:597-604
85 p or less = low risk of fatal PE – NPV = 99%
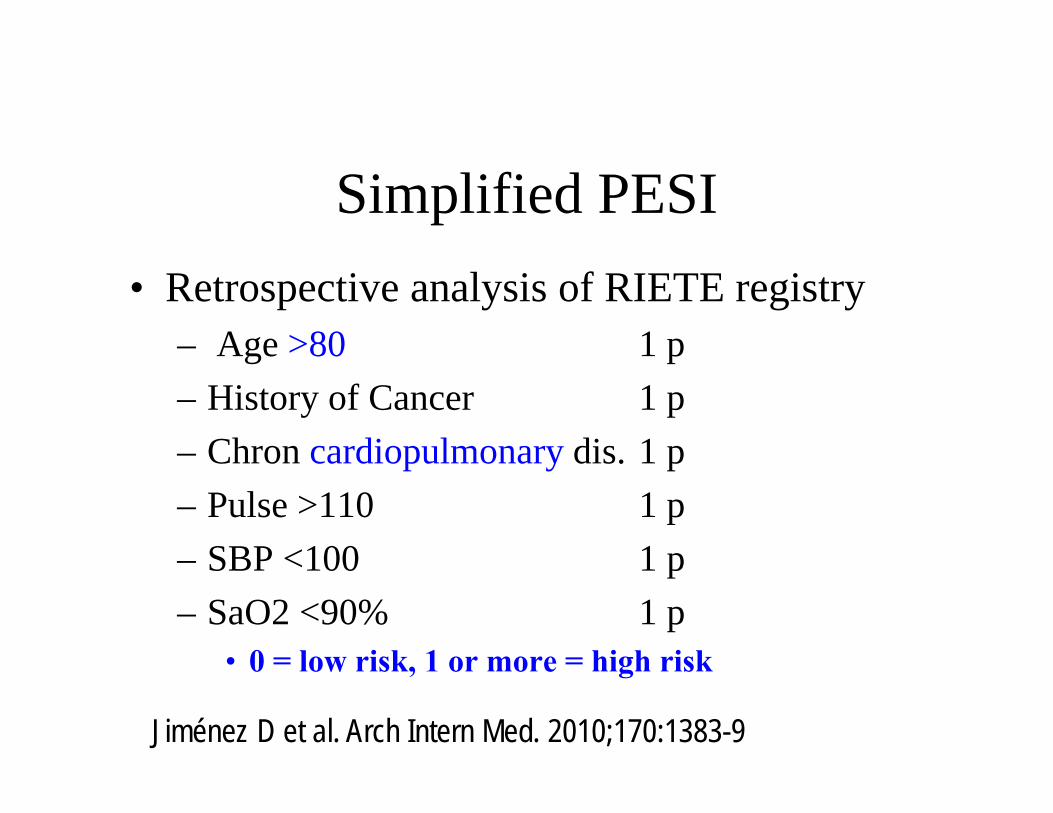
Simplified PESI• Retrospective analysis of RIETE registry
– Age >80 1 p– History of Cancer 1 p– Chron cardiopulmonary dis. 1 p– Pulse >110 1 p– SBP <100 1 p– SaO2 <90% 1 p
• 0 = low risk, 1 or more = high risk
Jiménez D et al. Arch Intern Med. 2010;170:1383-9
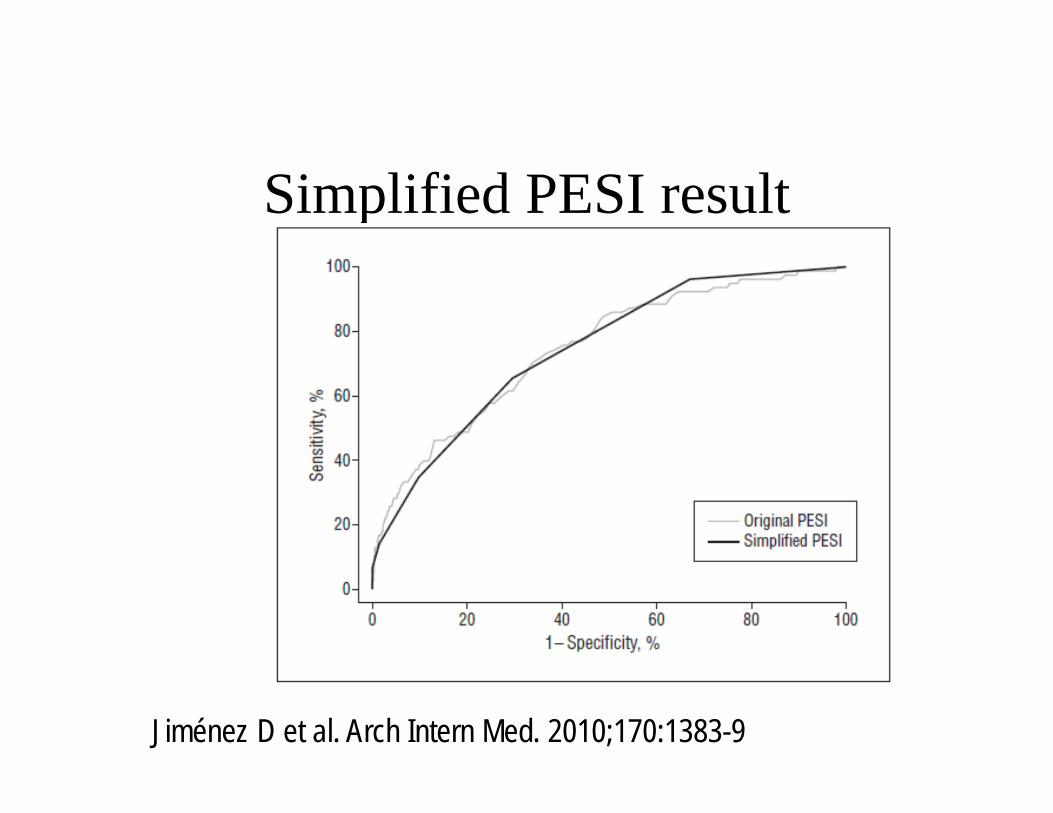
Simplified PESI result
Jiménez D et al. Arch Intern Med. 2010;170:1383-9
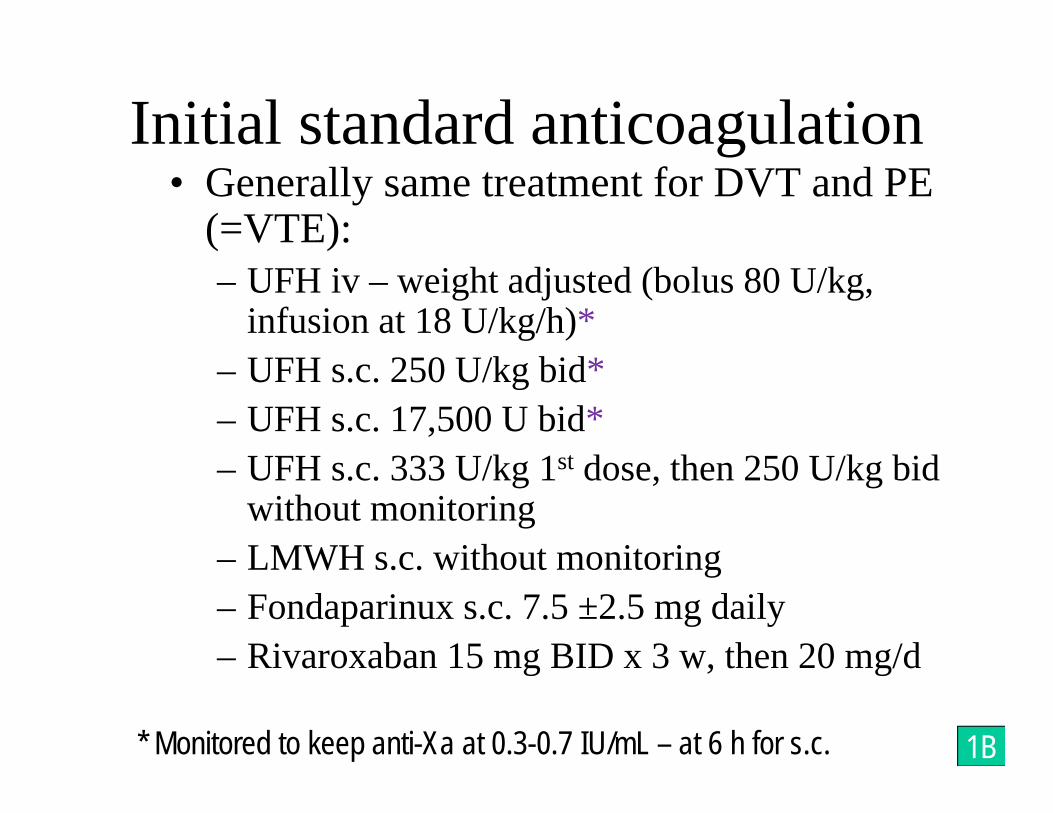
• Generally same treatment for DVT and PE (=VTE):– UFH iv – weight adjusted (bolus 80 U/kg,
infusion at 18 U/kg/h)*– UFH s.c. 250 U/kg bid*– UFH s.c. 17,500 U bid*– UFH s.c. 333 U/kg 1st dose, then 250 U/kg bid
without monitoring– LMWH s.c. without monitoring– Fondaparinux s.c. 7.5 ±2.5 mg daily– Rivaroxaban 15 mg BID x 3 w, then 20 mg/d
* Monitored to keep anti-Xa at 0.3-0.7 IU/mL – at 6 h for s.c. 1B
Initial standard anticoagulation
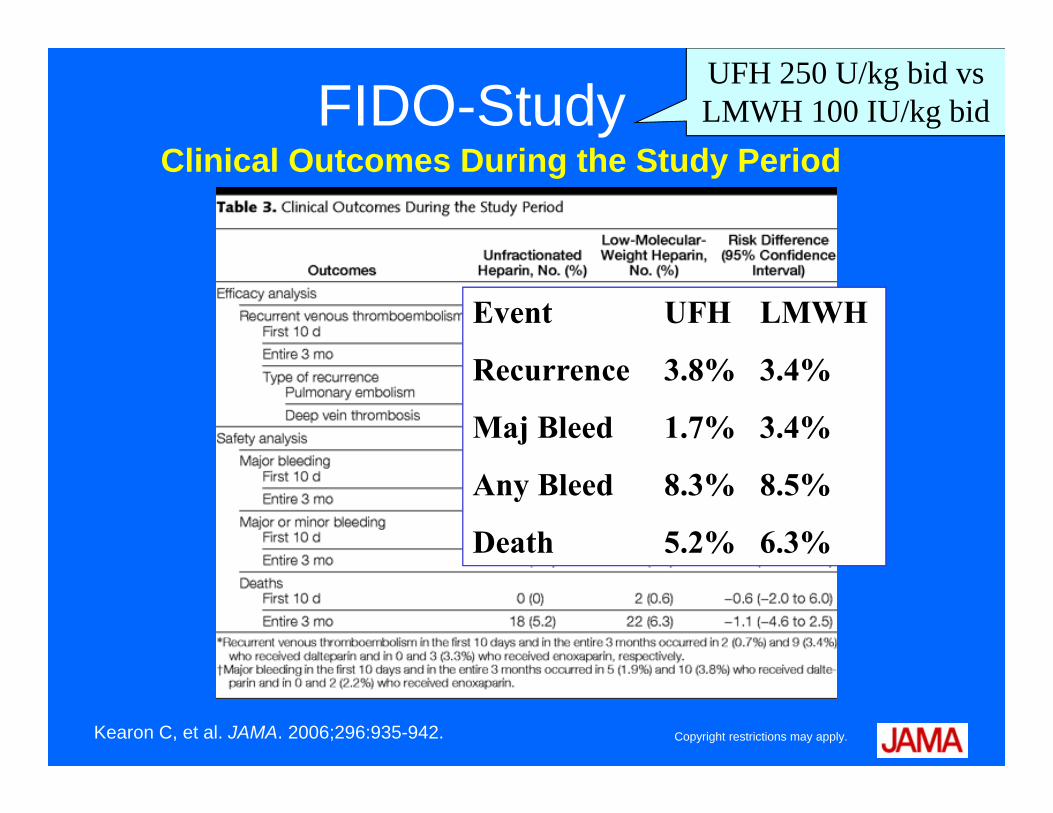
FIDO-Study
Copyright restrictions may apply.Kearon C, et al. JAMA. 2006;296:935-942.
Clinical Outcomes During the Study Period
UFH 250 U/kg bid vs LMWH 100 IU/kg bid
Event UFH LMWH
Recurrence 3.8% 3.4%
Maj Bleed 1.7% 3.4%
Any Bleed 8.3% 8.5%
Death 5.2% 6.3%
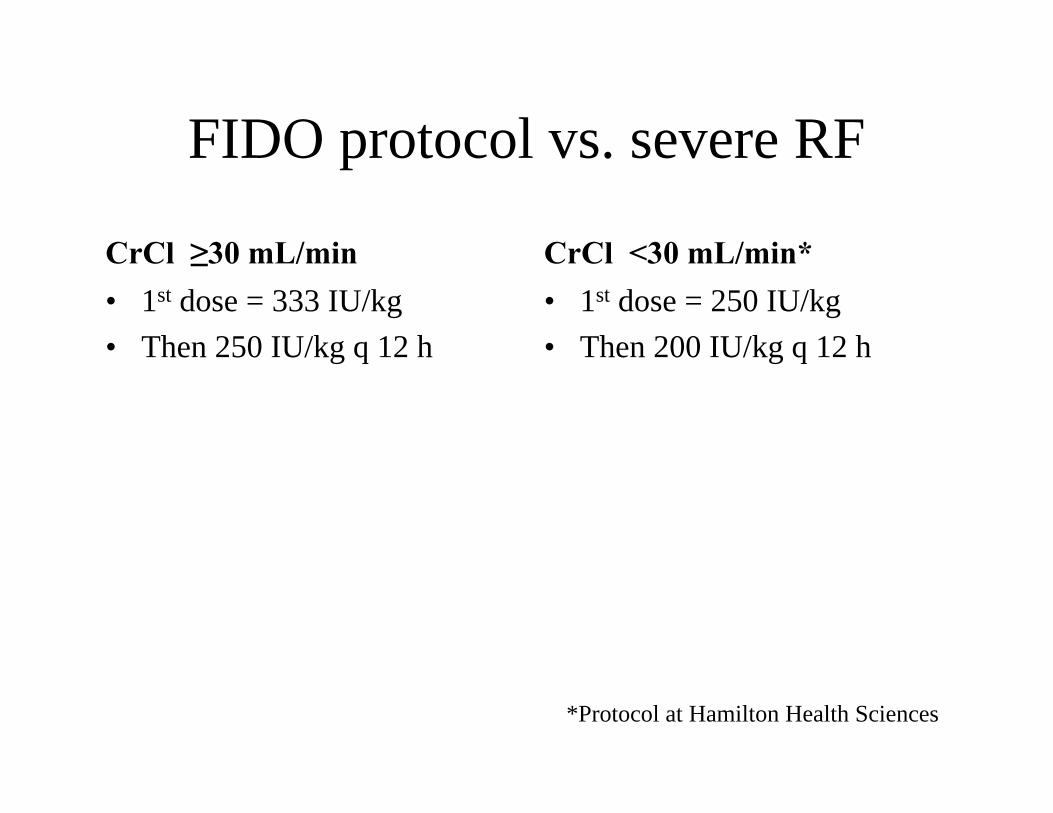
FIDO protocol vs. severe RF
CrCl ≥30 mL/min• 1st dose = 333 IU/kg• Then 250 IU/kg q 12 h
CrCl <30 mL/min*• 1st dose = 250 IU/kg• Then 200 IU/kg q 12 h
*Protocol at Hamilton Health Sciences
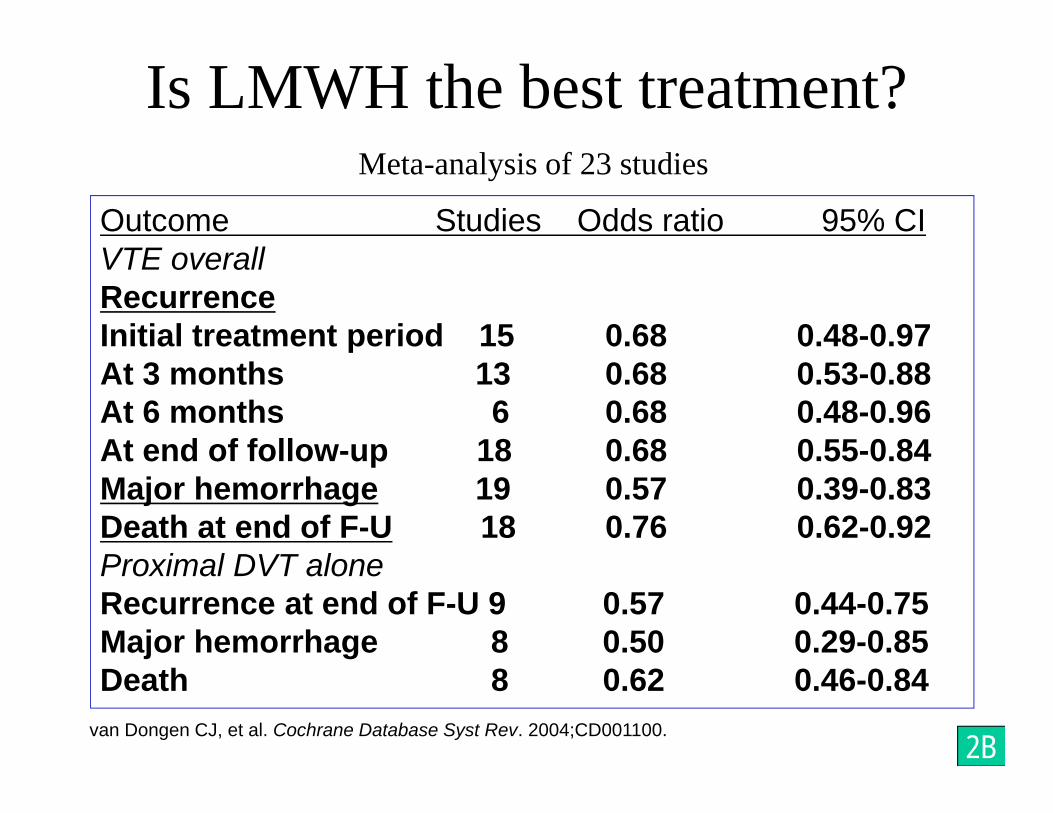
Is LMWH the best treatment?Meta-analysis of 23 studies
Outcome Studies Odds ratio 95% CIVTE overallRecurrenceInitial treatment period 15 0.68 0.48-0.97At 3 months 13 0.68 0.53-0.88At 6 months 6 0.68 0.48-0.96At end of follow-up 18 0.68 0.55-0.84Major hemorrhage 19 0.57 0.39-0.83Death at end of F-U 18 0.76 0.62-0.92Proximal DVT aloneRecurrence at end of F-U 9 0.57 0.44-0.75Major hemorrhage 8 0.50 0.29-0.85Death 8 0.62 0.46-0.84
van Dongen CJ, et al. Cochrane Database Syst Rev. 2004;CD001100. 2B
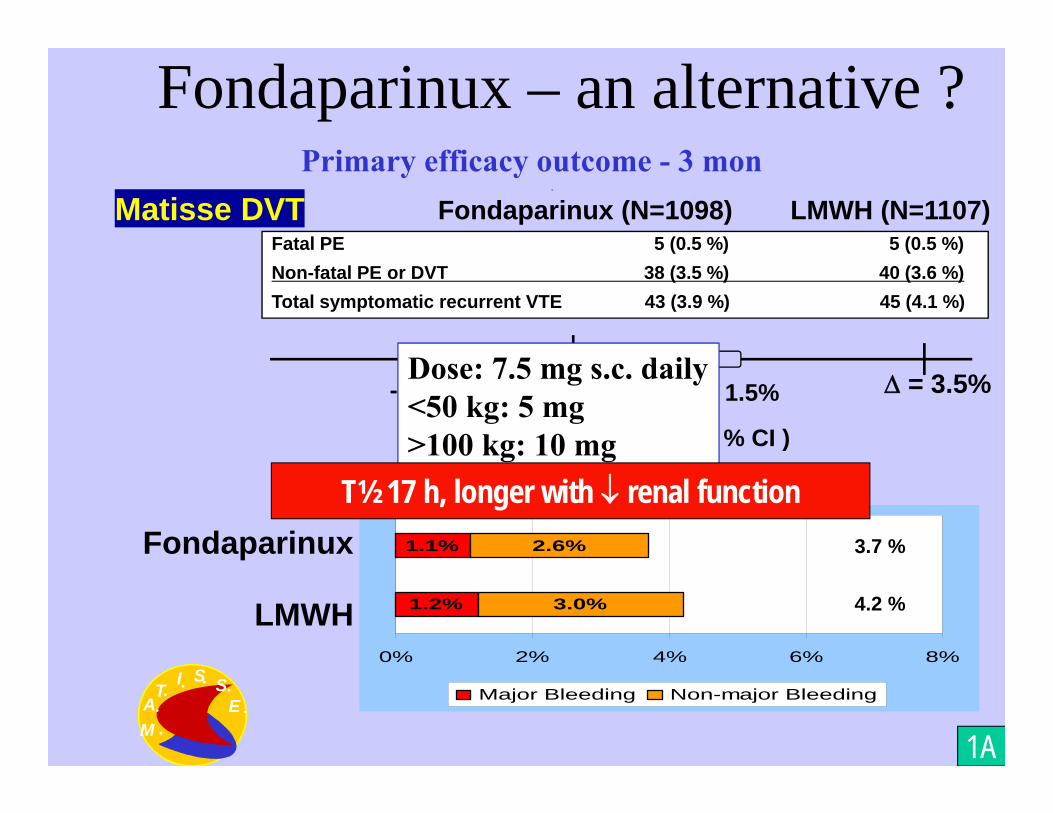
Fondaparinux – an alternative ?Primary efficacy outcome - 3 mon
Fondaparinux (N=1098) LMWH (N=1107)Matisse DVTFatal PE 5 (0.5 %) 5 (0.5 %) Non-fatal PE or DVT 38 (3.5 %) 40 (3.6 %)Total symptomatic recurrent VTE 43 (3.9 %) 45 (4.1 %)
-0.15 % = 3.5%0 1.5%-1.8%
Fondaparinux - LMWH (95 % CI )
AT
I S SE
M ... . . .
.
Dose: 7.5 mg s.c. daily<50 kg: 5 mg>100 kg: 10 mg
Fondaparinux
LMWH 1.2%
1.1%
3.0%
2.6%
0% 2% 4% 6% 8%
Major Bleeding Non-major Bleeding
3.7 %
4.2 %
Primary safety outcome - initially
1A
T½ 17 h, longer with renal function
• Extensive acute proximal DVT– Symptoms <14 d– Good functional status– Life expectancy >1 year
• Low risk of bleeding• Expertise and resources available• Can reduce acute symptoms• and risk of post-thrombotic syndrome
2C
Catheter-directed thrombolysis
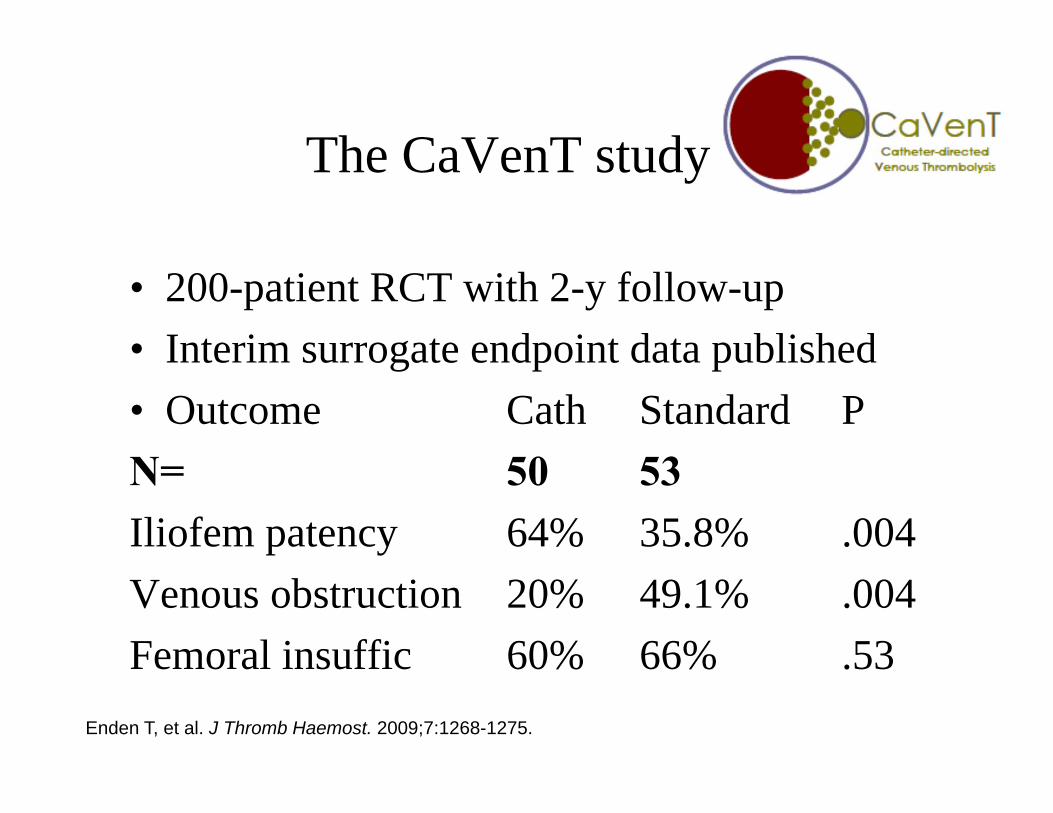
The CaVenT study
• 200-patient RCT with 2-y follow-up• Interim surrogate endpoint data published• Outcome Cath Standard PN= 50 53Iliofem patency 64% 35.8% .004Venous obstruction 20% 49.1% .004Femoral insuffic 60% 66% .53
Enden T, et al. J Thromb Haemost. 2009;7:1268-1275.
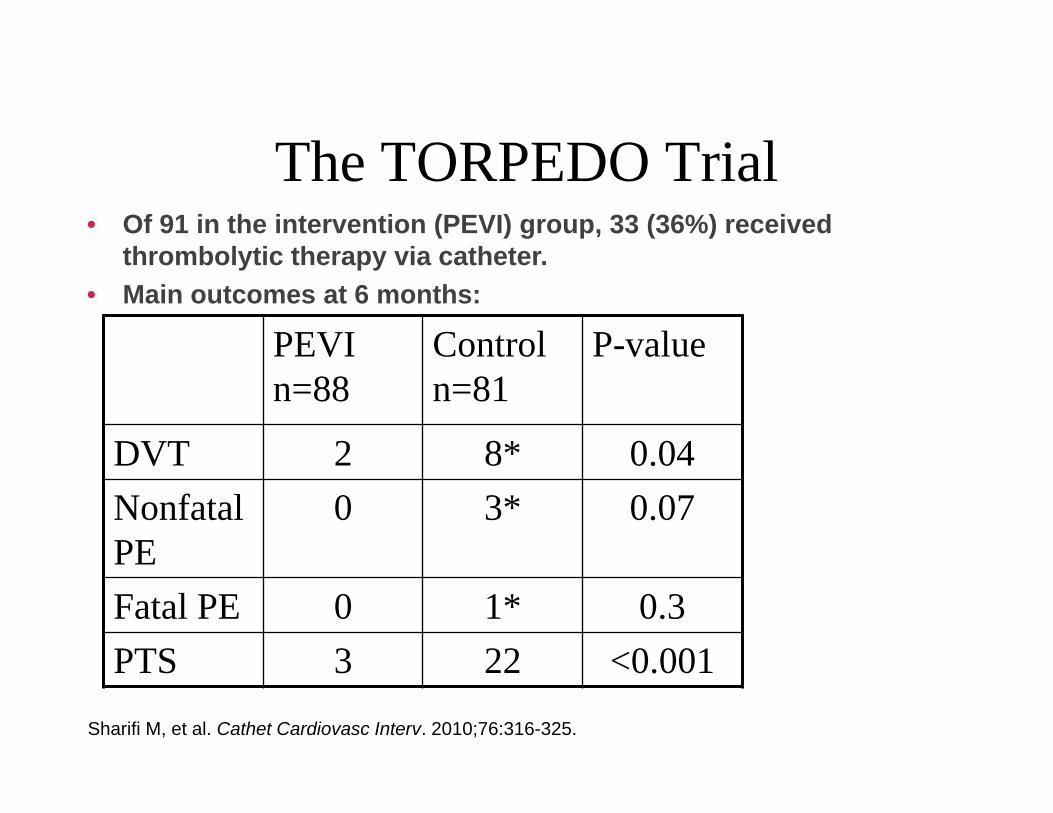
• Of 91 in the intervention (PEVI) group, 33 (36%) received thrombolytic therapy via catheter.
• Main outcomes at 6 months:
PEVIn=88
Controln=81
P-value
DVT 2 8* 0.04Nonfatal PE
0 3* 0.07
Fatal PE 0 1* 0.3PTS 3 22 <0.001
Sharifi M, et al. Cathet Cardiovasc Interv. 2010;76:316-325.
The TORPEDO Trial
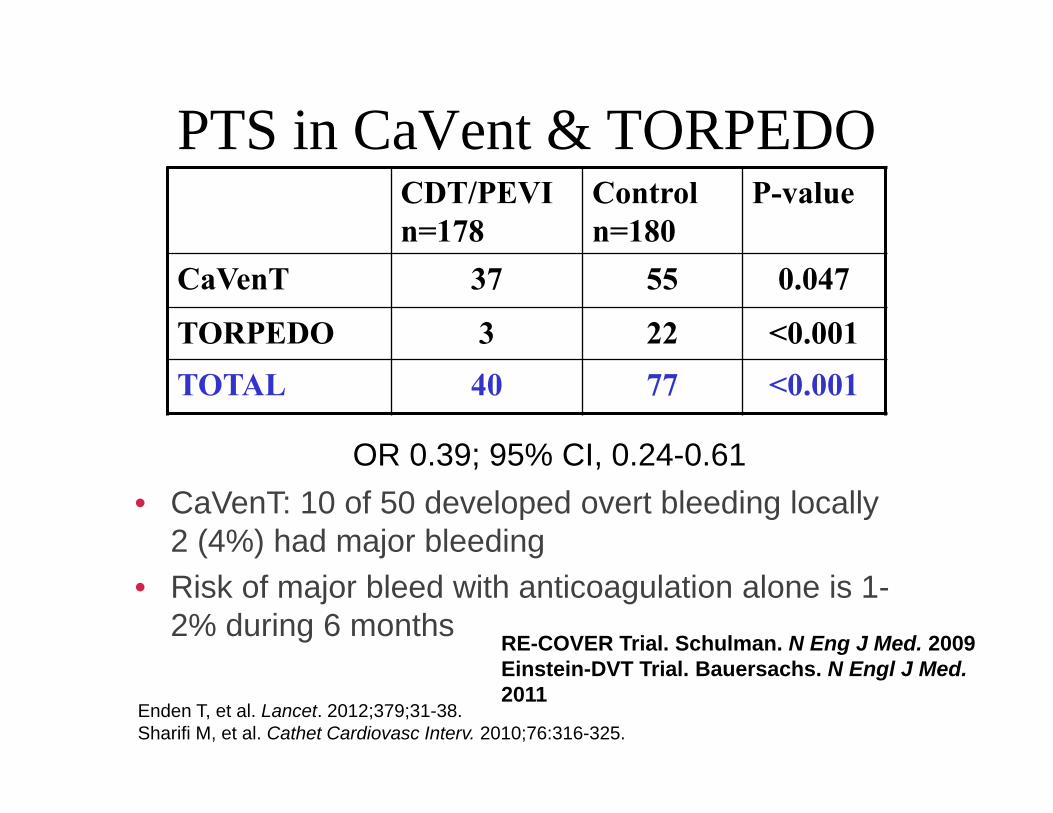
CDT/PEVIn=178
Controln=180
P-value
CaVenT 37 55 0.047
TORPEDO 3 22 <0.001TOTAL 40 77 <0.001
OR 0.39; 95% CI, 0.24-0.61
Enden T, et al. Lancet. 2012;379;31-38.Sharifi M, et al. Cathet Cardiovasc Interv. 2010;76:316-325.
• CaVenT: 10 of 50 developed overt bleeding locally2 (4%) had major bleeding
• Risk of major bleed with anticoagulation alone is 1-2% during 6 months RE-COVER Trial. Schulman. N Eng J Med. 2009
Einstein-DVT Trial. Bauersachs. N Engl J Med.2011
PTS in CaVent & TORPEDO
Follow-up after CDT• Balloon-angioplasty and stent for
underlying lesion• Alternative to CDT is Pharmacomechanical
Thrombolysis– Shortens treatment time
2C
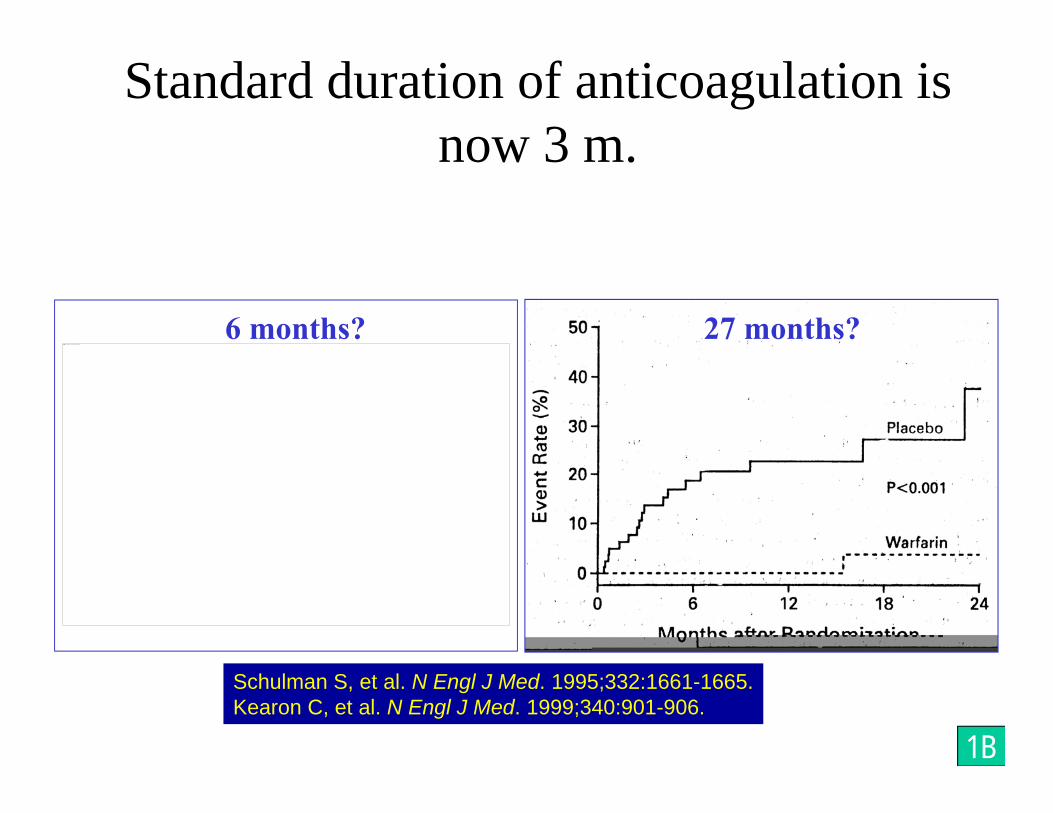
Standard duration of anticoagulation is now 3 m.
Schulman S, et al. N Engl J Med. 1995;332:1661-1665.Kearon C, et al. N Engl J Med. 1999;340:901-906.
6 months? 27 months?
1B
This image cannot currently be displayed.
WODITThis image cannot currently be displayed.
Agnelli, G et al. N Engl J Med. 2001;345:165-169.
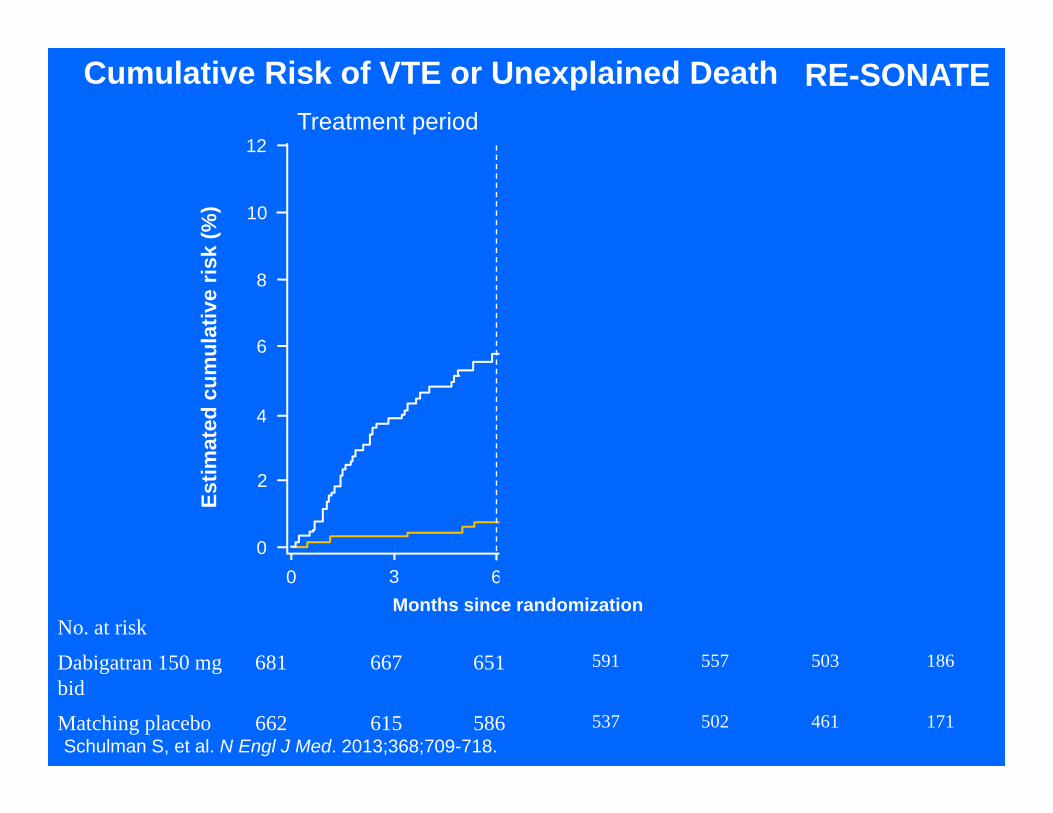
No. at risk
Dabigatran 150 mg bid
681 667 651 591 557 503 186
Matching placebo 662 615 586 537 502 461 171
Cumulative Risk of VTE or Unexplained Death
0
2
4
6
8
10
12
0 3 6 9 12 15 18Months since randomization
Estim
ated
cum
ulat
ive
risk
(%)
Treatment period Post-treatment follow-up
Dabigatran 150mg bidMatching placebo
RE-SONATE
Schulman S, et al. N Engl J Med. 2013;368;709-718.
Recurrent DVT after stopping
• Patients with unprovoked DVT– 3 months Rx – 10% first year after (WODIT)
– 6 months Rx – 10% first year after (DURAC)
– 12 months Rx – 10% first year after (WODIT)
– 24 months Rx – 10% first year after (LAFIT)
• No difference 3 vs 6 months in patients with proximal DVT or PE in DOTAVK
Pinede L, et al. Circulation. 2001;103:2453-2460.
Decision on long-term at 3 m• Long-term treatment for
–Unprovoked VTE–Second episode–Cancer
• Unless bleeding risk or adequate monitoring unavailable
2B
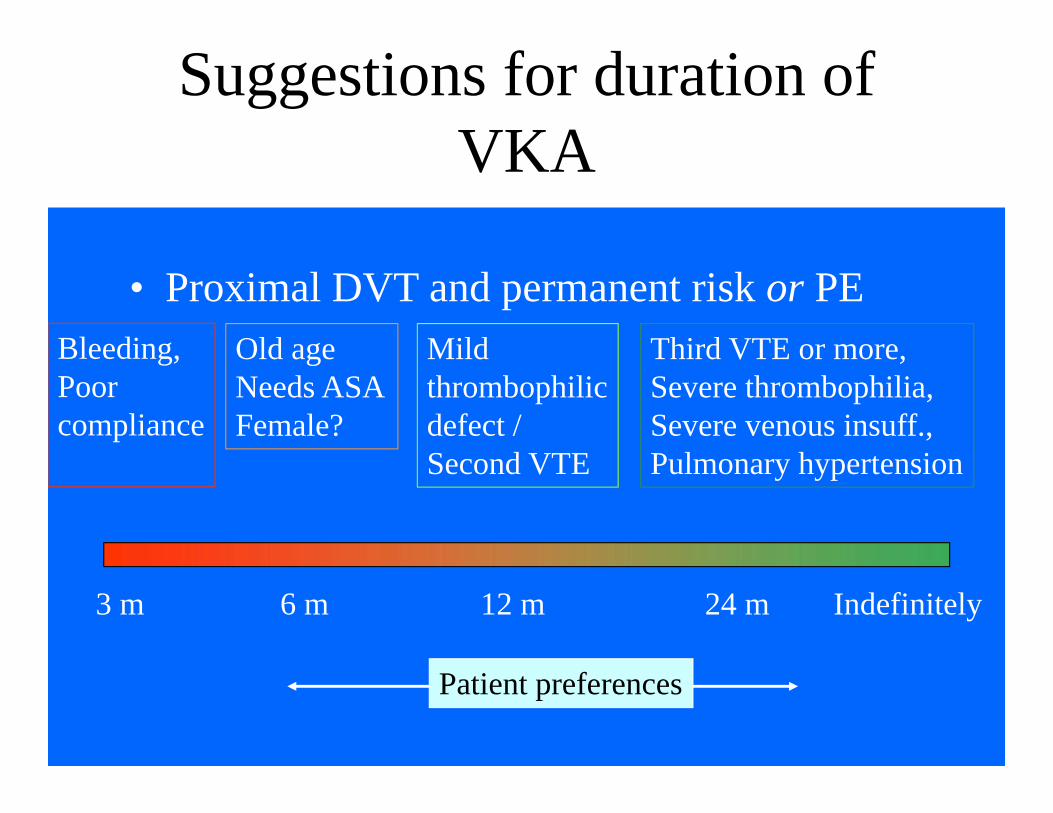
Suggestions for duration of VKA
• Proximal DVT and permanent risk or PE
3 m 6 m 12 m 24 m Indefinitely
Bleeding, Poorcompliance
Old ageNeeds ASAFemale?
Mildthrombophilicdefect /Second VTE
Third VTE or more,Severe thrombophilia,Severe venous insuff.,Pulmonary hypertension
Patient preferences
This image cannot currently be displayed.This image cannot currently be displayed.
Elevated D-dimer
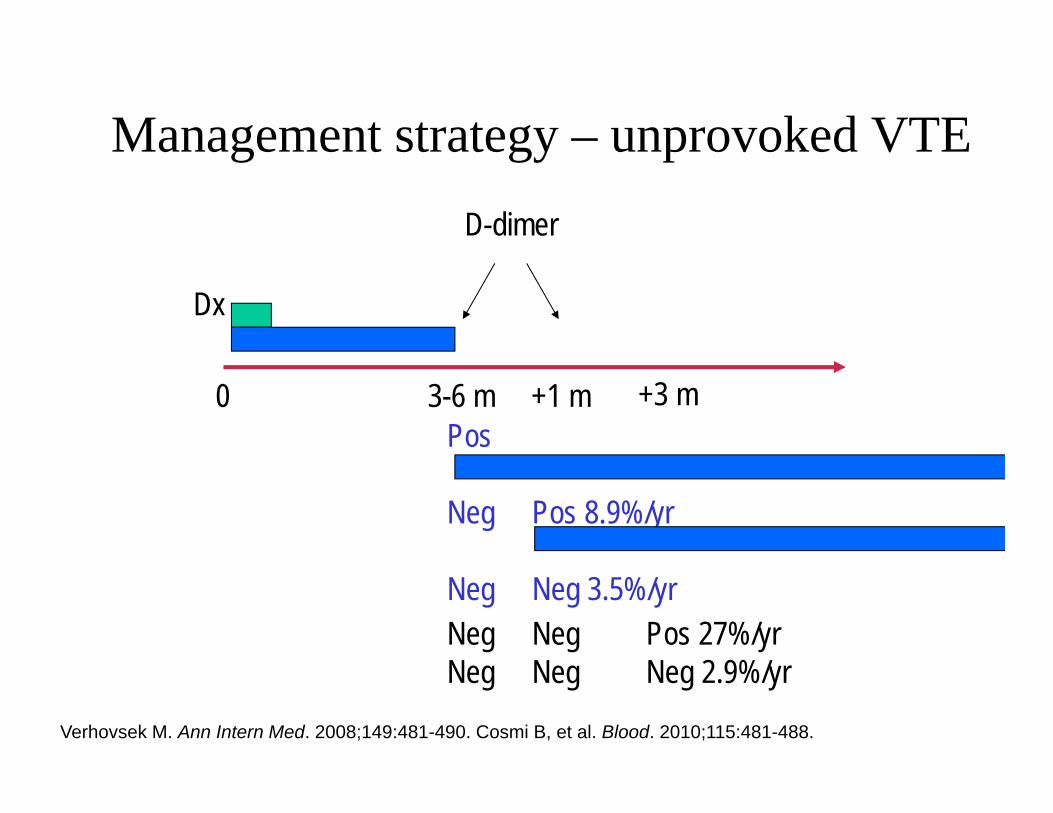
Management strategy – unprovoked VTE
Dx
0 3-6 m +1 m
D-dimer
Pos
Neg Pos 8.9%/yr
Neg Neg 3.5%/yr
Verhovsek M. Ann Intern Med. 2008;149:481-490. Cosmi B, et al. Blood. 2010;115:481-488.
+3 m
Neg Neg Pos 27%/yrNeg Neg Neg 2.9%/yr
D-dimer not in males?
• Several studies indicate that males have despite normalization of D-dimer a higher risk of recurrence.
• Recurrent VTE after neg-neg D-dimer– Men 9.7%– Women & no estrogen 5.4%– Women with estrogen Rx 0.0%
McRae S et al. Lancet 2006;368:371-8Kearon C et al. ISTH 2013
Recurrences• Recurrence rate adds up to about 30% after
8-10 years (Prandoni et al, Heit et al, Schulman et al.)
Prandoni P. Ann Intern Med 1996.Heit JA. Arch Intern Med 2000Schulman S. J Thromb Haemost 2005.
This image cannot currently be displayed.
This image cannot currently be displayed.
This image cannot currently be displayed.
Index event = DVTN=790
Index event = PEN=107
The DURAC I trial, Sweden 1988-2001Schulman et al. J Thromb Haemost 2006;4:734-42.Murin S. Thromb Haemost 2002.Douketis JD. JAMA 1998
Site of recurrent VTE
Case-fatality
• During short-term follow-up 50-100% higher if initial PE.
• After discontinuation of Rx: case fatality 3.8 – 9% (definite-probable vs any fatal PE) or 0.2-0.5 events/100 person-years.
• Rates depend on autopsy routines.
Douketis J. Ann Intern Med 2007;147:766-74.
Duration of follow-up and PTSThis image cannot currently be displayed.This image cannot currently be displayed.
Severe PTS 6-week gr 6-mo gr OR (95% CI)Class 5-6 17 (4.2) 16 (3.8) 1.12 (0.57-2.22)
Conclusions
• VTE is an increasing problem• Several risk scores and risk stratification tools are
available and should be used• Diagnostic algorithm for DVT/PE is helpful• Many options for treatment of VTE exist• Decide at 3-6 months regarding stopping or
indefinite anticoagulation
This image cannot currently be displayed.
Recommended