9/29/2017
1
Bethany Sarosiek, RN, MSN, MPH, CNLUniversity of Virginia Health SystemCharlottesville, [email protected]
Enhanced Recovery After Surgery at the University of Virginia Medical Center
• None
Disclosures
• Provide background and rationale behind implementing an ERAS program
• Describe the key steps for implementation of an interdisciplinary ERAS program
• Identify potential barriers to ERAS program implementation and ways to overcome them
Objectives

9/29/2017
2
2012 NSQIP data revealed discouraging trends starting in 2008 when outcomes at UVA were better than average:
– Morbidity: 1.35 (from 0.99)– LOS: 0.79 (from 0.99)– UTI: 1.95 (not tracked in 2008)– SSI: 1.37 (from 0.99)
Why ERAS in Colorectal Surgery?
A multimodal approach to perioperative care designed to decrease the time required to recover from surgery
Major components include:• Not starving patients before surgery• Intraoperative “goal-directed therapy” (GDT) – using
advanced hemodynamic monitors to only give IV fluids when they are needed
• Adequate pain control with minimal opioid use• Early ambulation• Patients take ownership of their care
What is ERAS?
• Recognizing the need for improvement, we implemented an Enhanced Recovery After Surgery (ERAS) protocol for all patients undergoing elective colorectal surgery at an academic institution.
• Provide quality care at reduced costs
• Inter-disciplinary effort to standardize care
Our Objective

9/29/2017
3
• Perioperative teaching• Surgery Handbook• Setting realistic goals and expectations
The Preoperative Phase
• “Goal-directed fluid therapy” (GDT) • Vasopressors for hypotension• Long acting intrathecal opioid • Ketamine and lidocaine infusion• Standardized protocol
The Intraoperative Phase
“Pleth Variability Index” monitors “fluid responsiveness” continuously based on the pulse oximeter waveform
• Clears and OOB in PACU• Elimination of IV opioids from
order set• Lidocaine drip for 48 hours• IVF at 40 cc/hr for 24 hours only• Checklists for nursing staff to
complete WITH patient• Discharge criteria IDENTICAL• Discharge goal POD 3
Ordersets and checklists help to drive care!
The Postoperative Phase

9/29/2017
4
Inter-disciplinary Partnership
• Core Team• Surgeon• Anesthesia • RN champion
• Partners• Pharmacy/Pain Management • Registered Dieticians• Participating staff from Clinic, Preop, OR, PACU, Postop• Informatics
• Widespread systems changes (EPIC, OR, checklists, pathway)
• Ongoing education prior to implementation
• ERAS implemented August 1, 2013
• All patients undergoing elective abdominal surgery on colorectal service enrolled in protocol regardless of procedure or medical comorbidities
• Compared pre/post data– pre ERAS (08/2012 – 02/2013) – post ERAS (08/2013 – 08/2014)
Colorectal Data Comparison

9/29/2017
5
LOS relative to Medical Center

9/29/2017
6

9/29/2017
7
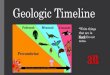
Financial Impact of ERAS
Mean Total Cost Mean Direct Cost
Pre‐ERAS 25,344 20,435
Post‐ERAS 18,777 13,306
$0.00
$5,000.00
$10,000.00
$15,000.00
$20,000.00
$25,000.00
$30,000.00$6,567/pt
$7,129/pt
Financial Impact of ERAS
Pre‐ERAS Post‐ERAS
Expected Direct Costs 13,599 14204
Actual Direct Costs 20435 13306
0
5,000
10,000
15,000
20,000
25,000
+ $6,836/pt
‐$898/pt$746,231 in cost savings
Decision pack in 2014 (>$700,000 investment):
• Clinicians• RN champion to lead effort• 2 LIPs for outpatient and inpatient support• Medical directors - salary support
• Data analyst
• Equipment (OR and post-op monitoring)
The Business Case for Expansion

9/29/2017
8
Expansion Timeline to Date
GYN ERAS March 2015
Thoracic ERAS March 2016
Whipple ERAS Jan 2017
Colorectal ERAS Aug 2013
• Changing deep-rooted, traditional practices
• Electronic Medical Record Process
• Additional (unforeseen) costs
• Academic medical center w/ rotating staff
• Ongoing iterative process
Barriers
• Comprehensive patient educational materials• Checklists for staff AND patients• EPIC (EMR) support• ERAS indication in ALL phases of care• Frequent compliance audits/data collection• Frequent feedback to providers• Ongoing protocol revisions to ensure application of latest
evidence
From a Systems Perspective:Communication is key!
…Make it as easy as possible to do the right
thing!

9/29/2017
9
• Ever-growing interest from add’l surgical services
• Successful implementation of electronic checklist
• ERAS app
• Expanded institutional support
Success Stories
• Multidisciplinary effort
• Buy-in from everyone to standardize care– Will be different at each institution, individual elements not as
important as adhering to 5 main ERAS concepts
• Dedicated surgeon, anesthesiologist, nurse champions
• Strict monitoring of compliance
• Constant feedback and iteration
What does ERAS implementation require?
• Ortho Joint• Spine (Ortho and Neurosurgery)• General Surgery• Thoracic (Esophagectomy)• Hepatic Resection• Breast Surgery• Neurosurgery• Vascular Surgery• Pediatric Surgery• Donor Kidney (Transplant)• Urology
Plans for Expansion
Bottom Line:
• Our GOAL is to expand these principles to every patient undergoing surgery at UVA
• ERAS should be the standard of care - providing quality surgical care at reduced cost with a focus on improving patient outcomes
30

9/29/2017
10
Expanded ERAS Program Organizational Chart
Which of the following is not a key concept of an ERAS program:
1. Early ambulation
2. Opioid-sparing multimodal pain management
3. Preoperative fasting
4. Patient education and expectation management
Self Assessment Question 1
Name three key members of a inter-disciplinary ERAS team.
Self Assessment Question 2

9/29/2017
11
Which of the following could be considered a barrier to ERAS implementation:
1. Remarkable change from traditional practices
2. Cost
3. Continuous change in staff
4. All of the above
Self Assessment Question 3
E R A S =
1) Protocolized care
2) Opioid minimization
3) Focus on mobilization
4) Patient empowerment
5) Reduced healthcare costs
6) More efficient use of scarce resources
33
Thank you!

9/29/2017
12
1. Kehlet, H. Multimodal Approach to Control Postoperative Pathophysiology and Rehabilitation. Br J Anaesth 1997;78:606-617
2. Zhuang, CL et al. Enhanced Recovery After Surgery Programs versus Traditional Care for Colorectal Surgery: A Meta-analysis of Randomized Control Trials. Dis Colon Rectum 2013;56:667-678.
3. Brandstrup, B et al. Effects of Intravenous Fluid Restriction on Postoperative Complications: Comparison of Two Perioperative Fluid Regimens: A Randomized Assessor-Blinded Multicenter Trial. Ann Surg 2003; 238:641-648.
4. Gan, TJ et al. Goal-directed Intraoperative Fluid Administration Reduces Length of Hospital Stay After Major Surgery. Anesthesiology 2002;97:820-826.
5. Barreveld, A et al. Preventive Analgesia by Local Anesthetics: the Reduction of Postoperative Pain by Peripheral Nerve Blocks and Intravenous Drugs. Anesth Analg 2013;116:1141-1161.
6. Thiele, R et al. Standardization of Care: Impact of an Enhanced Recovery Protocol on Length of Stay, Complications, and Direct Costs after Colorectal Surgery. J Amer Coll Surg 2015; 220(4):430-443.
7. Modesitt, S et al. Enhanced Recovery Implementation in Major Gynecologic Surgeries: Effect of Care Standardization. Ob & Gyn 2016;128(3):457-466.
8. Roulin, D et al. Cost-effectiveness of the Implementation of an Enhanced Recovery Protocol for Colorectal Surgery. Br J Surg 2013;100:1108-1114.
References
Recommended