VASCULAR/INTERVENTIONALDr. Jeff Jaskolka
University of Toronto
Disclosure:
Have acted as consultant for:SiemensBraccoLantheusNo bearing on the contents of this lecture
Some uses of devices shown are “off-label”

DISCLAIMER:VIR not the same as diagnosticWe are simple folkFocus on management, diagnoses straightforward

CASES
CASE 148 year old woman with hypertension
11

Diagnosis?
Best treatment?
Would you use a stent?
11
CASE 255 year old woman with hypertension
22

Diagnosis?
Best treatment?
Would you use a stent?
22
CASE 375 year old male with right leg claudication
33
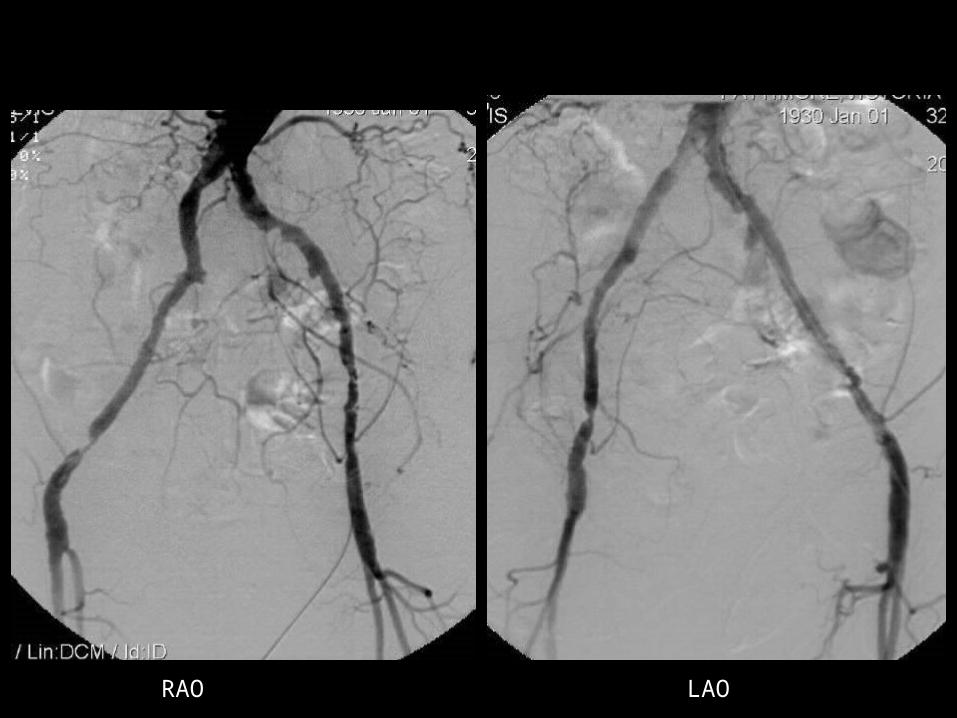
RAO LAO

Diagnosis?
Best treatment?
If endovascular treatment, would you use a stent?
33
CASE 477 year old male, left leg claudication
44
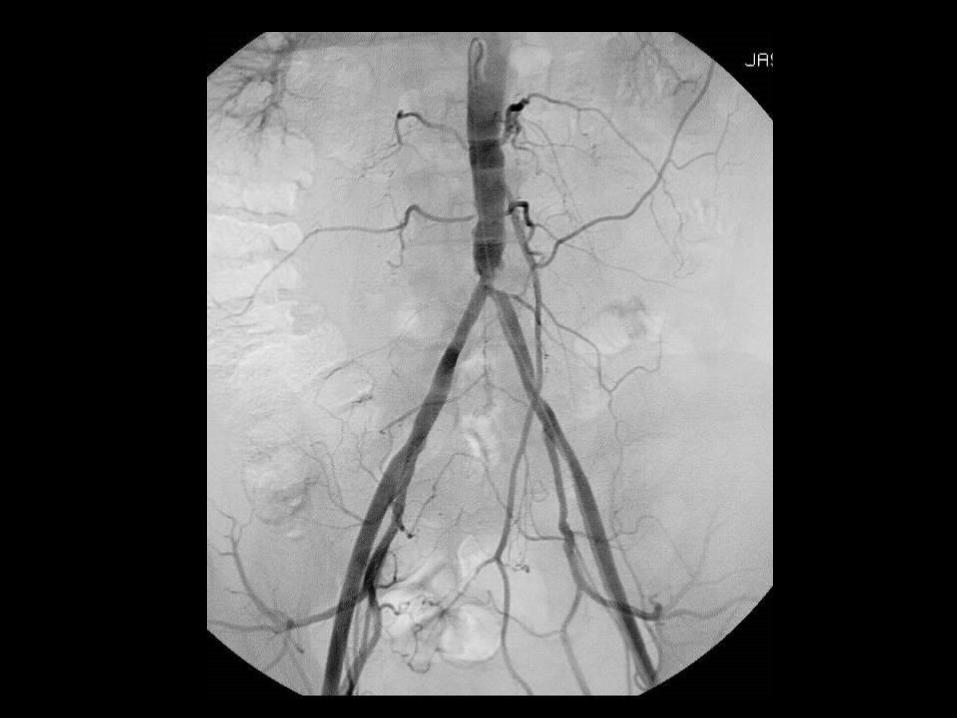
Diagnosis?
Best treatment?
What would you use for endovascular treatment?
44
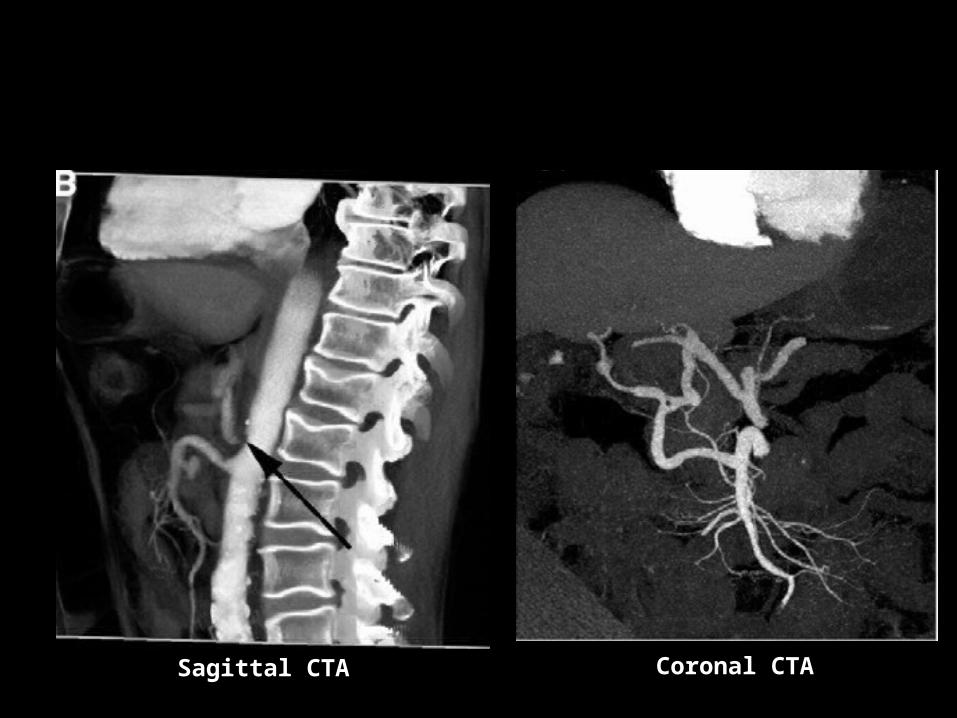
CASE 535 year old female, pain after eating
55
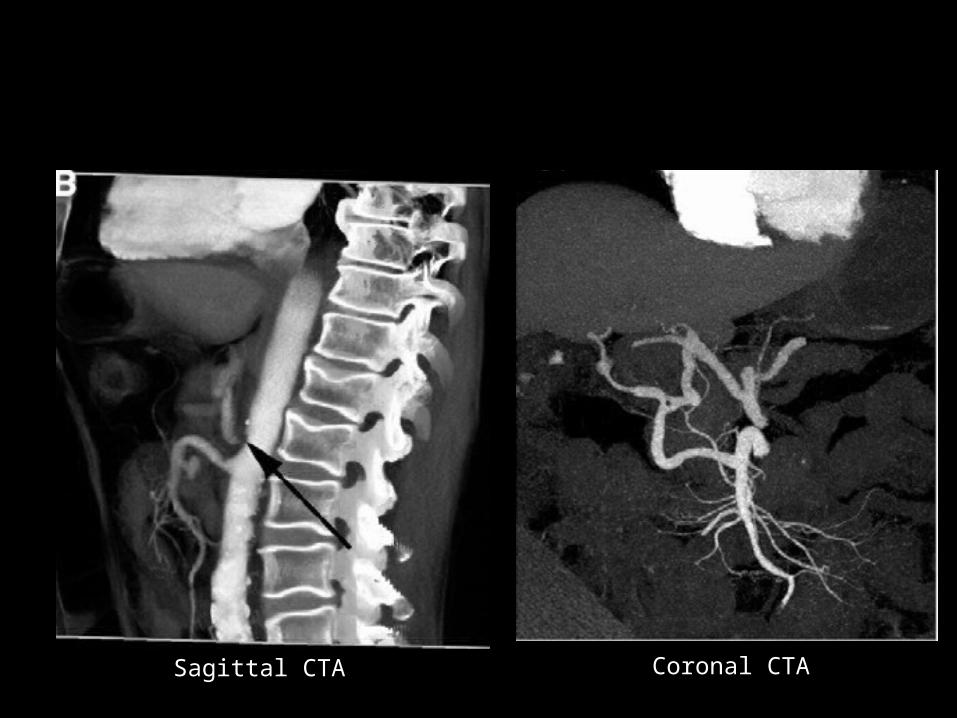
Sagittal CTA Coronal CTA
Diagnosis?
Provocative manouver?
Best treatment?
55

CASE REVIEW

Case 1: FIBROMUSCULAR DYSPLASIA (BILATERAL)
11
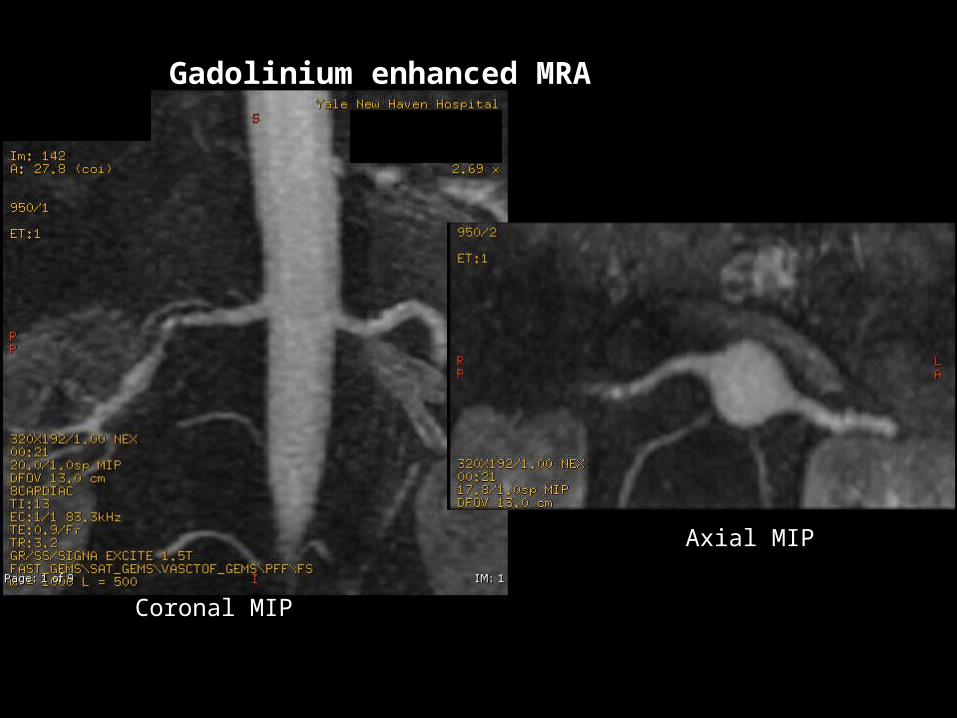
Gadolinium enhanced MRA
Coronal MIP
Axial MIP
Differential Diagnosis
Atherosclerosis
Standing waves
Vasculitis
1
Presentation Title - Subtitle
Key Points
NOTABLE:
more common in women, 65% bilateral
CLASSIC DESCRIPTOR:
“String of beads” appearance of renal artery
+/- webs
+/- stenosis
PEARL:
mid/distal renal artery vs. ostial/proximal 1/3
5 types, medial fibroplasia (type II) most common
1
Presentation Title - Subtitle
Key Points
TREATMENT:
endovascular preferred
angioplasty alone, no stent
1
Presentation Title - Subtitle
22
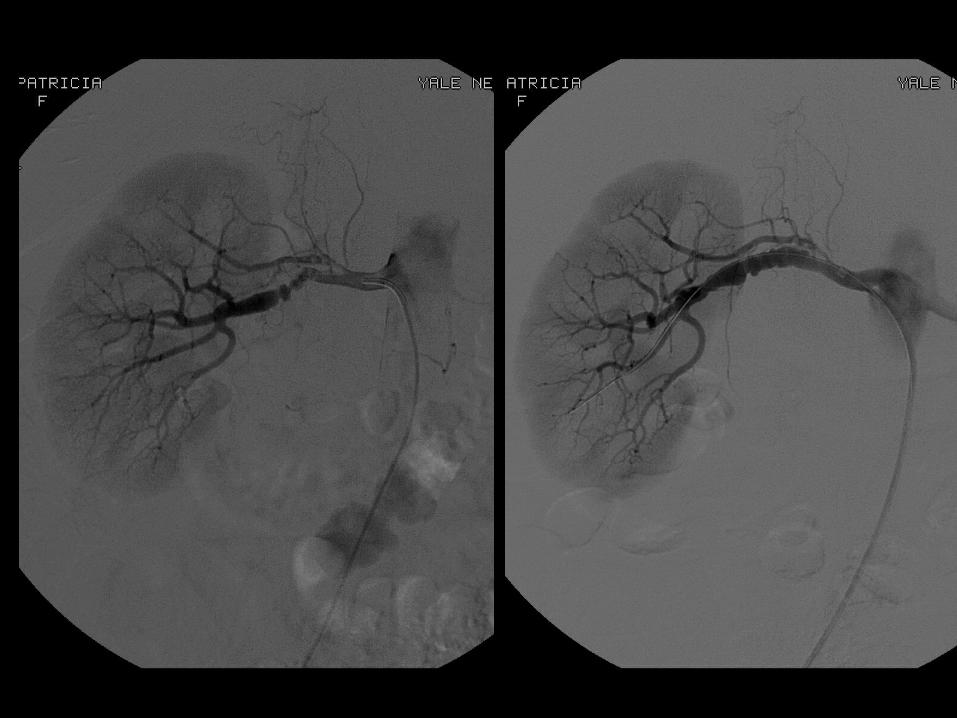
Case 2: RENAL ARTERY STENOSIS(ATHEROSCLEROTIC)

Frontal aortogram Left renal arteriogram post treatment

Differential Diagnosis
Vasculitis
Fibromuscular dysplasia
Congenital
2
Presentation Title - Subtitle
Atherosclerosis
Atherosclerosis
Atherosclerosis
Key Points2
Presentation Title - Subtitle
NOTABLE:
<10% cases of hypertension due to RAS
CLASSIC DESCRIPTOR:
Eccentric, ostial narrowing of renal artery with associated atherosclerotic aorta
PEARL:
>50% stenosis or >10% systolic pressure drop across lesion considered hemodynamically significant
Key Points
TREATMENT:
MEDICAL
endovascular treatment for:
failed medical therapy
renal salvage (ie. renal failure)
flash pulmonary edema
endovascular treatment is primary stent
balloon expandable for high radial force and accuracy of placement
2
Presentation Title - Subtitle
33
Case 3: EXTERNAL ILIAC ARTERY STENOSIS

Differential Diagnosis
Atherosclerosis
Atherosclerosis
Atheroscelrosis(trauma/iatrogenic, vasculitis)
3
Presentation Title - Subtitle

RAO arteriogram LAO arteriogram

Key Points3
Presentation Title - Subtitle
NOTABLE:
common cause of unilateral claudication
CLASSIC DESCRIPTOR:
focal, short, eccentric stenosis
PEARL:
best, most durable treatment for all iliac lesions is surgical bypass

Key Points
TREATMENT:
best treatment is surgical bypass
many patients not candidates
multiple comorbidities
best lesions for angioplasty
concentric
short
non-calcified
stenting in external iliac artery optional
self expanding stent best
3
Presentation Title - Subtitle
44
Case 4: AORTOILIAC STENOSIS
Differential Diagnosis
No differential
4
Presentation Title - Subtitle


Key Points4
Presentation Title - Subtitle
NOTABLE:
iliac bifurcation lesions extension of aortic disease
CLASSIC DESCRIPTOR:
bilateral calcified narrowing of iliac bifurcation
PEARL:
Treatment is with “kissing” balloons or stents
Key Points
TREATMENT:Aortobiiliac or aortobifemoral bypass graft
most durableEndovascular
kissing stents/balloons for simultaneous treatment of both sides or to protect unaffected side from
occlusion/dissectionballoon vs. self expanding stents
higher radial force, precise position
4
Presentation Title - Subtitle
55
Case 5: MEDIAN ARCUATE LIGAMENT SYNDROME
Sagittal CTA Coronal CTA
Differential Diagnosis
Atherosclerosis
Vasculitis
Extrinsic compression (not truly median arcuate ligament “syndrome”)
5
Presentation Title - Subtitle
Key Points5
Presentation Title - Subtitle
NOTABLE:
extrinsic compression of celiac axis by median arcuate ligament
CLASSIC DESCRIPTOR:
J-shaped appearance of proximal celiac artery
PEARL:
stenosis gets worse with expiration
treatment is conservative or surgical. Endovascular treatment not appropriate

Key Points – OPENING
Presentation Title - Subtitle
Not all lesions require treatment
Angioplasty is not the only treatment
Best lesions for angioplasty:
- short, concentric, non-calcified
Stenting for bailout, ostial lesions
Balloon expanding stents - ostial lesions
Self expanding stents – flexible/mobile anatomy
CASES
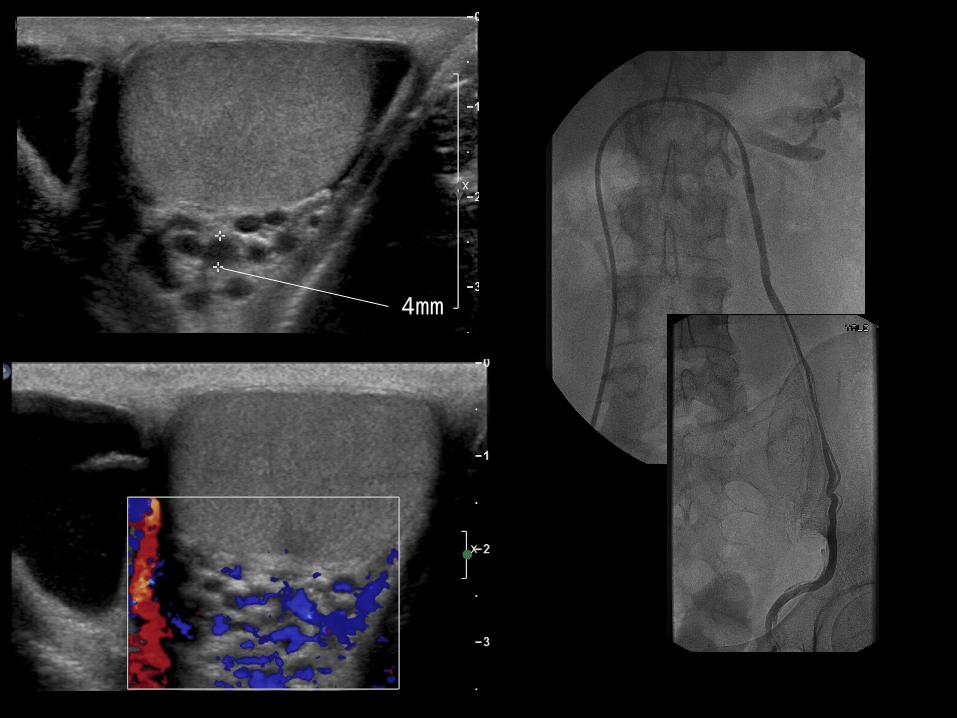
CASE 665 year old female, bruising 4 days post cardiac catheterization
66
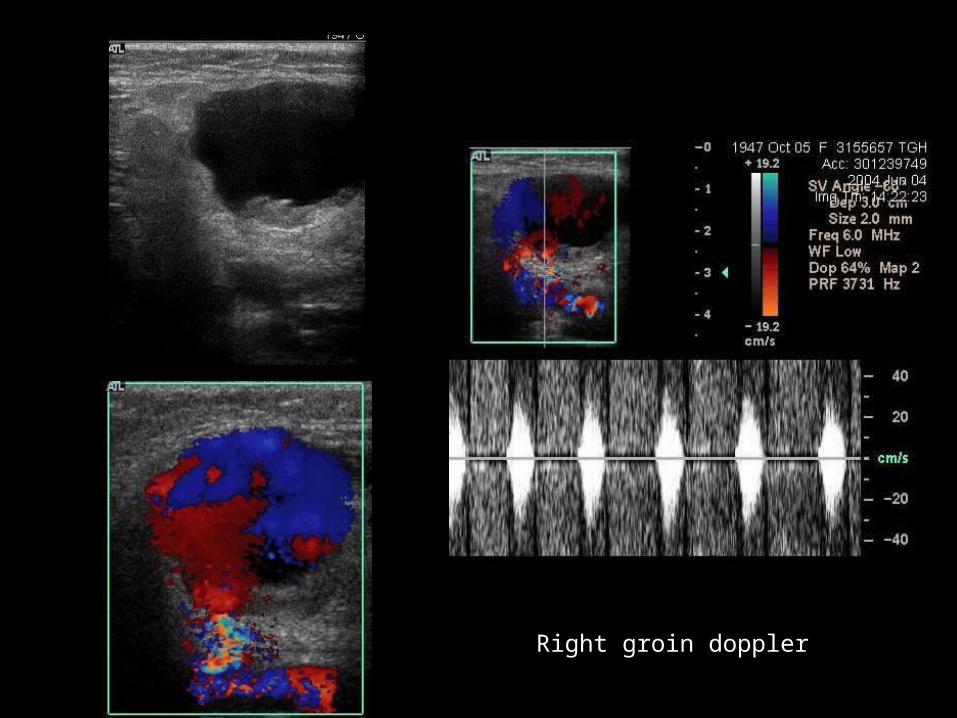
Right groin doppler
Diagnosis?
Best treatment?
What would you use for endovascular treatment?
33
CASE 750 year old male found unconscious with hematochezia
77

Diagnosis?
Best treatment?
What would you use for endovascular treatment?
77

CASE 880 year old male, routine f/u post EVAR
88
Diagnosis?
Does this need treatment?
If so, what would treatment be?
33
CASE 970 year old female with massive hemoptysis
99
Diagnosis?
Treatment options?
What is the most devastating potential complication of endovascular treatment?
99
CASE 1034 year old man with scrotal mass
1010
4mm
Diagnosis?
Treatment options?
What would you use for endovascular treatment?
1010

CASE REVIEW
66
Case 6: COMMON FEMORAL ARTERY PSEUDOANEURYSM
Differential Diagnosis
True aneurysm
Mycotic aneurysm
Arteriovenous fistula
6
Presentation Title - Subtitle
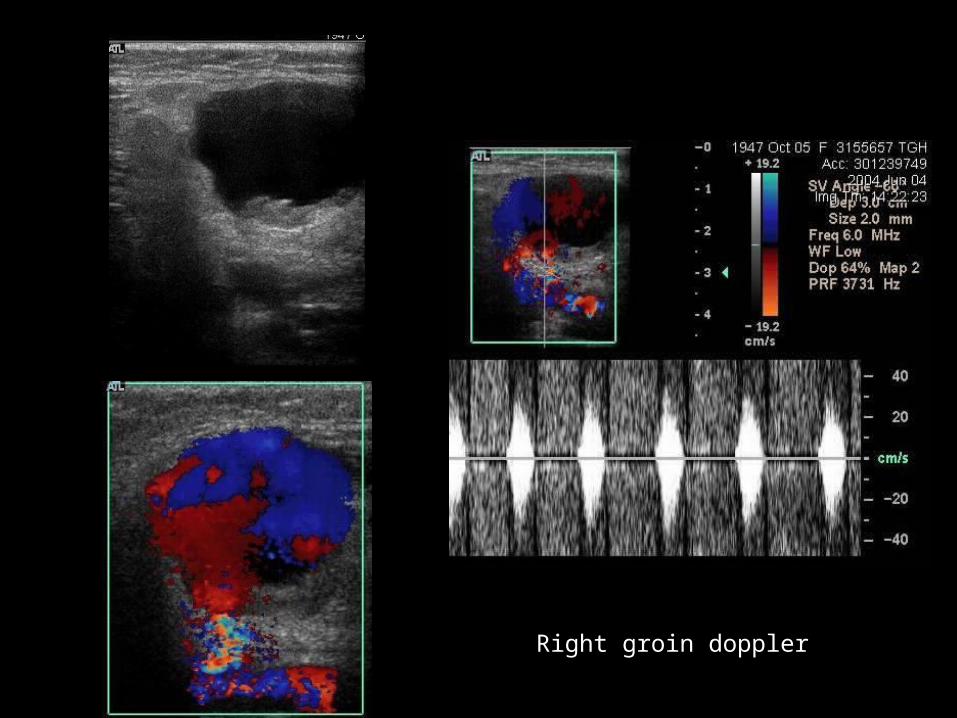
Right groin doppler

Needle tip
Key Points6
Presentation Title - Subtitle
NOTABLE:
Common complication of femoral artery complication.
Presents with bruising, palpable lump
CLASSIC DESCRIPTOR:
Yin-yang appearance. To-and-fro flow in neck.
PEARL:
Small (<2cm) pseudoaneurysms may resolve spontaneously
Key Points
TREATMENT:
expectant (for small lesions)
ultrasound graded compression
percutaneous thrombin injection
small needle
500-1000U thrombin
must have short neck, no AVF
surgical repair
stent graft
6
Presentation Title - Subtitle
77
Case 7: LOWER GI HEMORRHAGE (DIVERTICULAR)
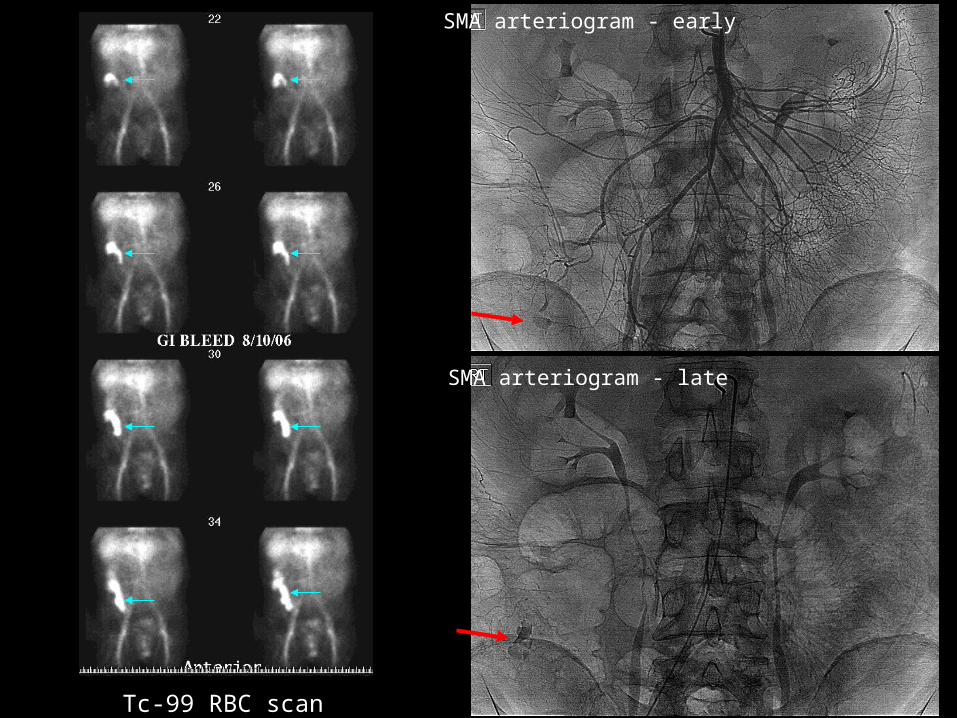
Tc-99 RBC scan
SMA arteriogram - early
SMA arteriogram - late

Differential Diagnosis
Angiodysplasia
Neoplasia (polyp/carcinoma)
Colitis
7
Presentation Title - Subtitle
Key Points7
Presentation Title - Subtitle
NOTABLE:
divericulosis accounts for 65% of LGI hemorrhage
CLASSIC DESCRIPTOR:
extravasation of contrast, pooling on delayed phase, shape of diverticulum
PEARL:
do not image an unstable patient with lower GI hemorrage – take them straight to angio suite
Key Points
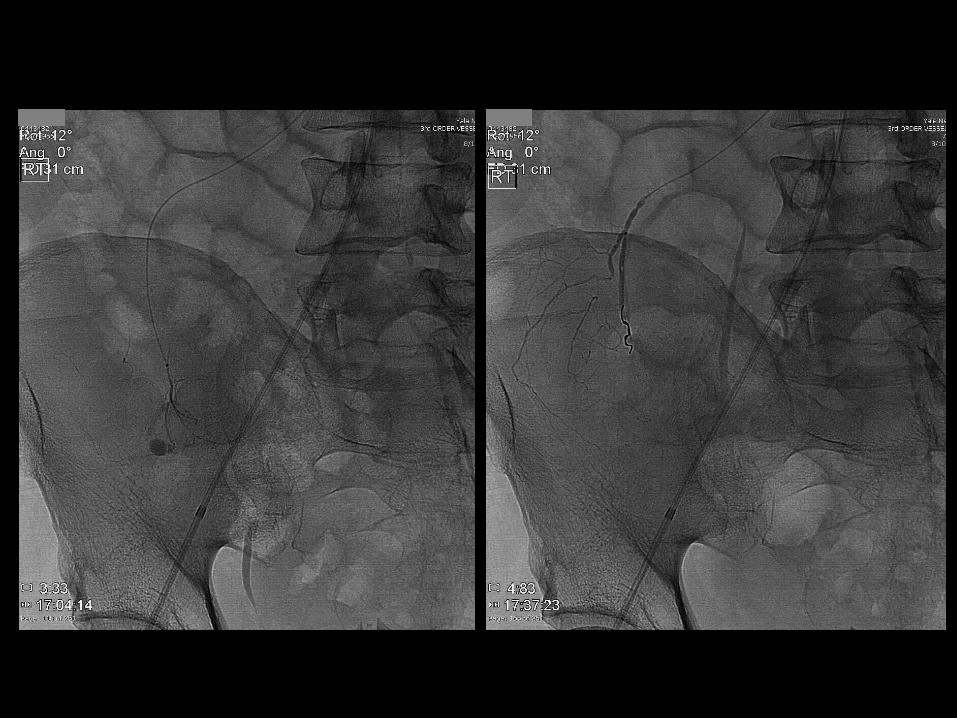
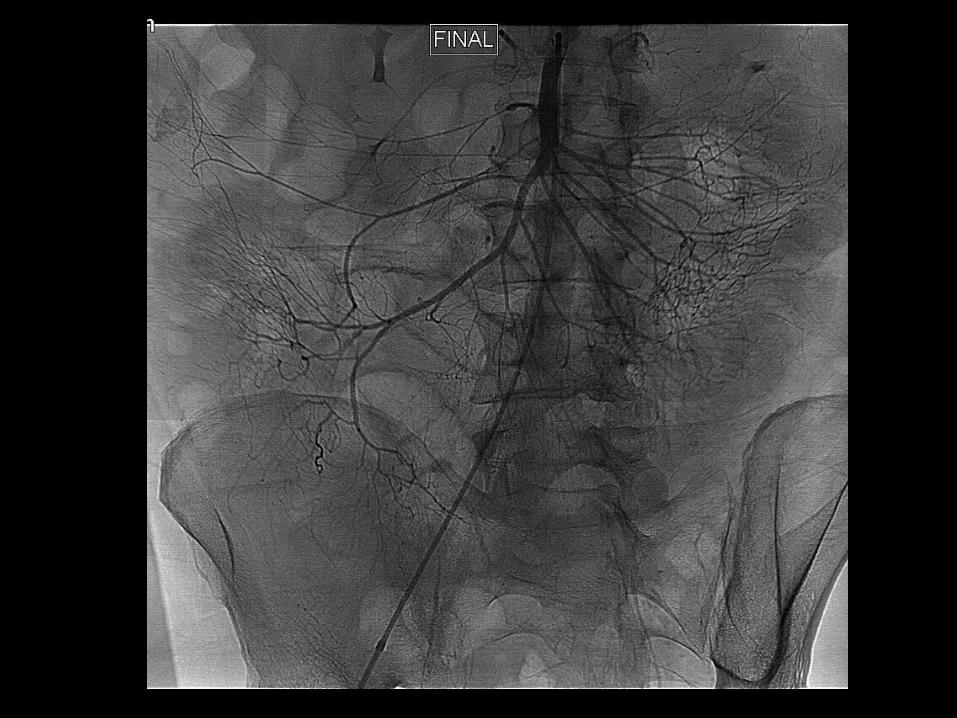
MANAGEMENT:
stabilize patient
if stable – image (CTA, Tc99 RBC scan)
if actively bleeding – to angio for diagnosis/treatment
treatment is embolization
superselective coil embolization
particles risk of ischemia
7
Presentation Title - Subtitle
88
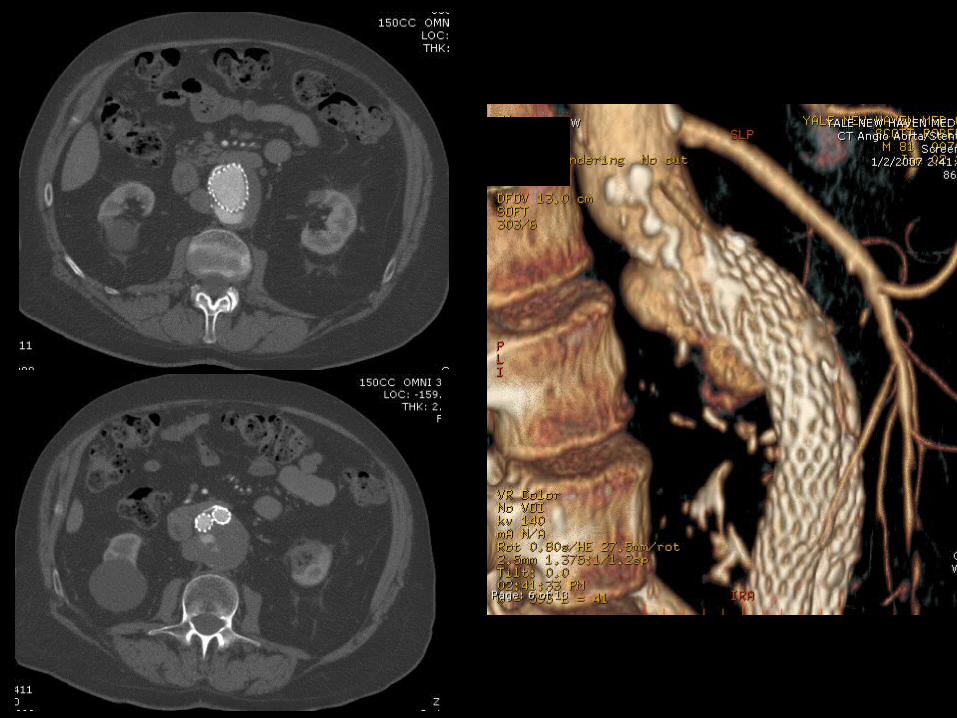
Case 8: TYPE I ENDOLEAK POST EVAR

Differential Diagnosis
Endoleak classification
Type I – inadequate seal proximally or distally
Type II – retrograde flow via collateral
Type III – graft failure, component separation
Type IV – porosity of graft
Type V - endotension
8
Presentation Title - Subtitle
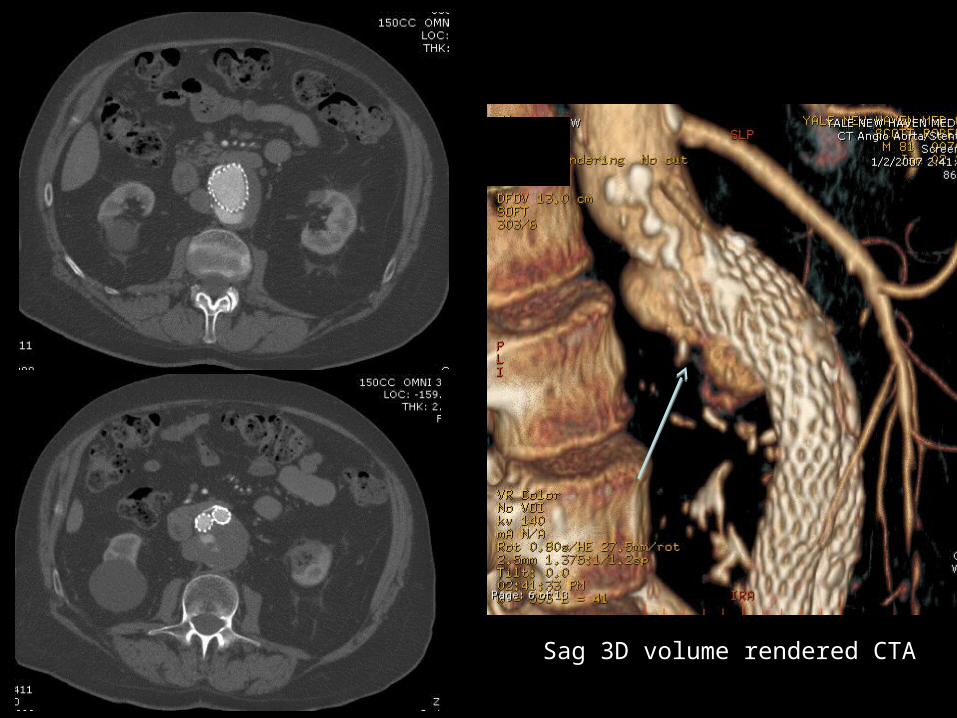
Sag 3D volume rendered CTA
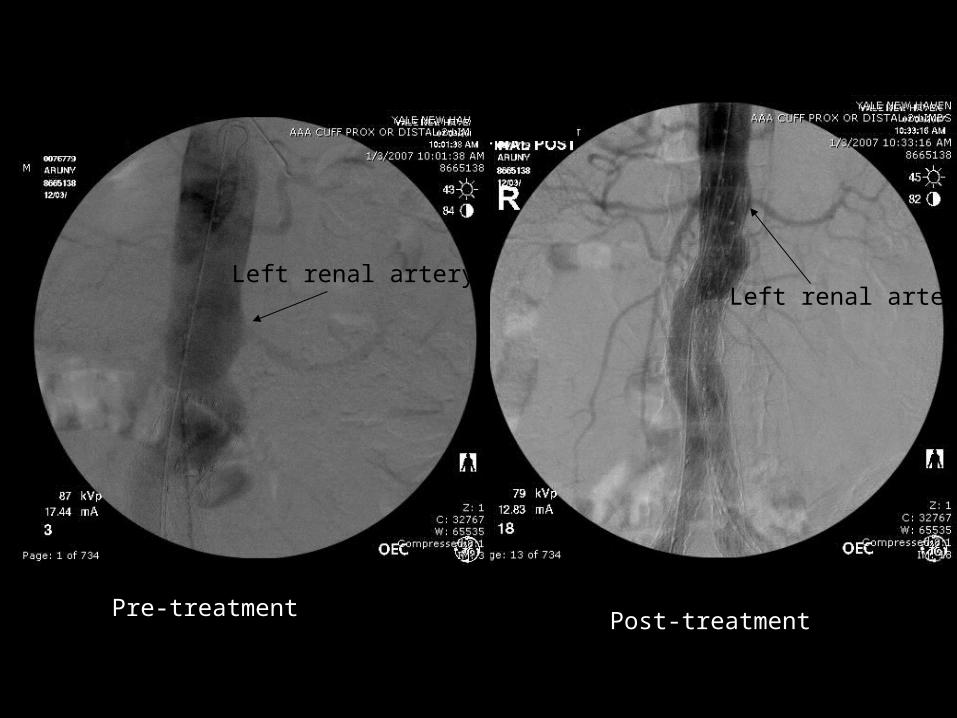
Left renal arteryLeft renal artery
Pre-treatment Post-treatment
Key Points8
Presentation Title - Subtitle
NOTABLE:
Type II endoleaks post EVAR are common and usually managed expectantly
Type I endoleaks more common in grafts without suprarenal fixation or in large/short necks
CLASSIC DESCRIPTOR:
contrast outside endograft, within aneurysm sac
PEARL:
Delayed imaging improves sensitivity for detection of endoleak
Key Points
TREATMENT:Type 1 endoleak
treated by extension of graft or buttress with balloon expandable stent
Type 2 endoleaktreated by embolizationdirect sac puncture vs. transarterial
Type 3 endoleaknew graft within old graft
Type 4 endoleak, usually intraoperative and resolve spontaneously
Type 5 endoleak – no treatment
8
Presentation Title - Subtitle
99
Case 9:LEFT UNILATERAL VARICOCELE
Differential Diagnosis
Secondary varicocele
- retroperitoneal mass
- renal vein/IVC occlusion
9
Presentation Title - Subtitle
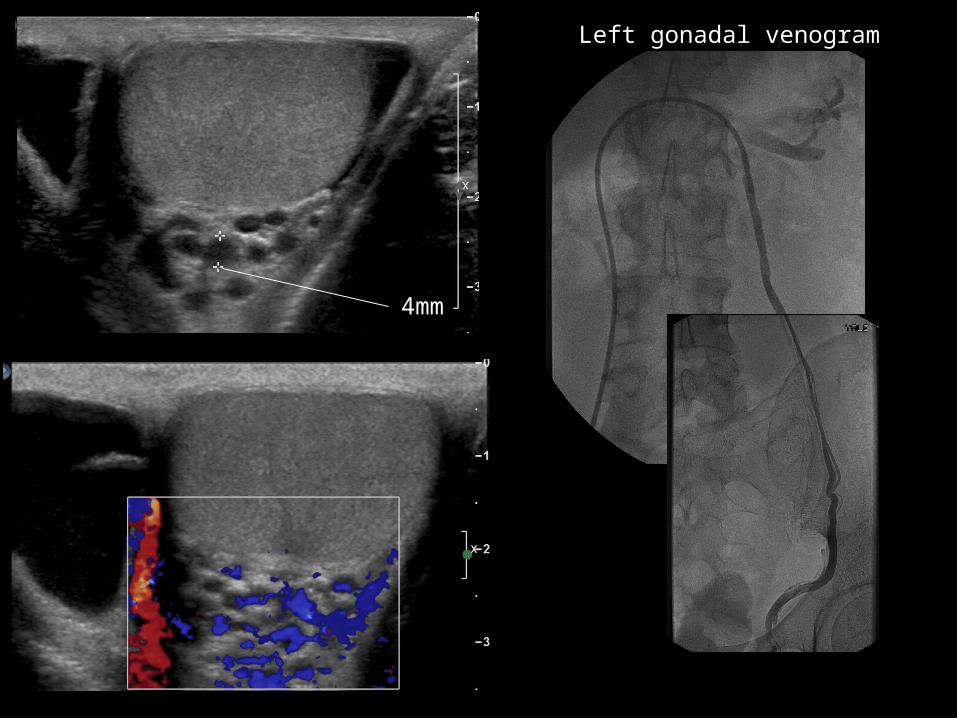
4mm
Left gonadal venogram

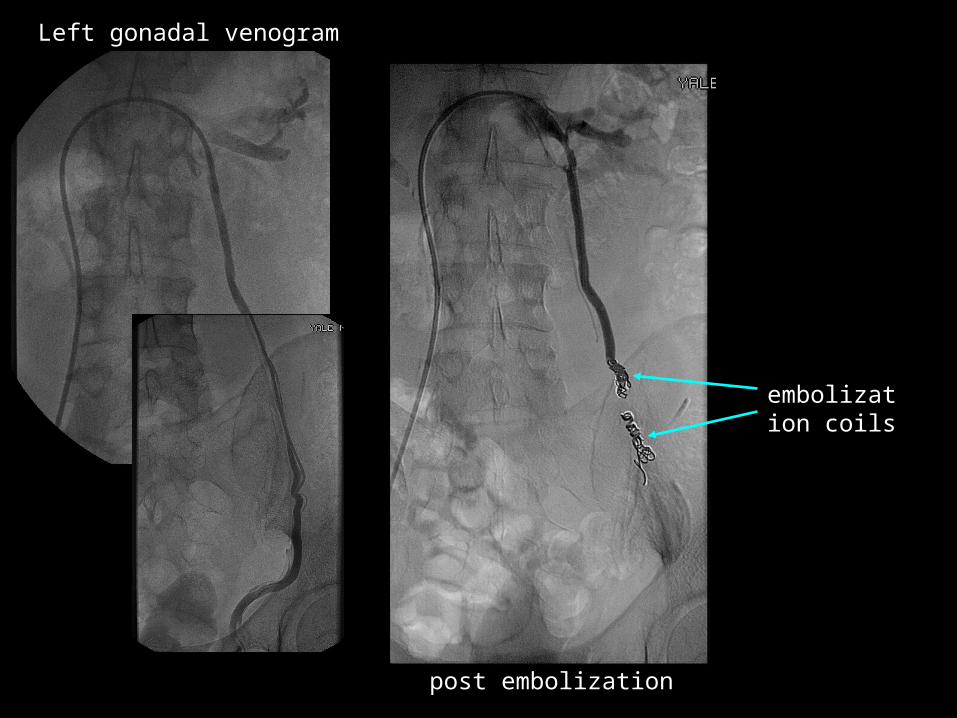
post embolization
embolization coils
Left gonadal venogram

Key Points9
Presentation Title - Subtitle
NOTABLE:
common cause of palpable scrotal mass
veins > 3mm on ultrasound are diagnostic
CLASSIC DESCRIPTOR:
“bag of worms” on ultrasound
PEARL:
most often “idiopathic”, look for a cause in cases of isolated right-side varicocele

Key Points
TREATMENT:
endovascular (embolization) vs. surgical (ligation)
both are “minimally invasive”
both have comparable outcomes
embolic material of choice is coils for large vessel occlusion
9
Presentation Title - Subtitle
1010
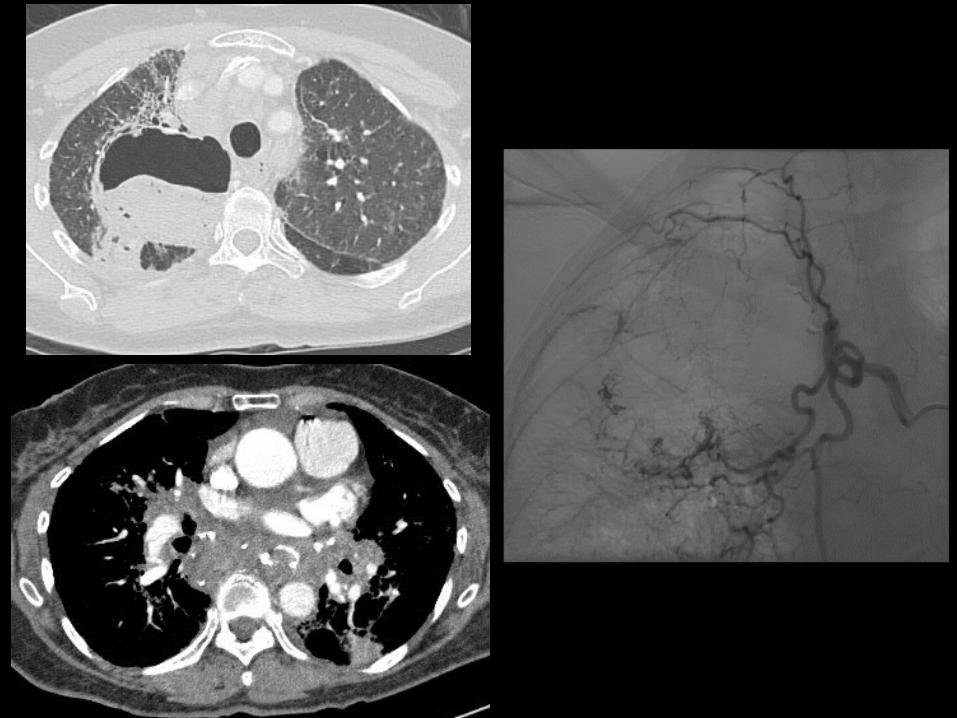
Case 10: MASSIVE HEMOPTYSIS (ASPERGILLOMA)
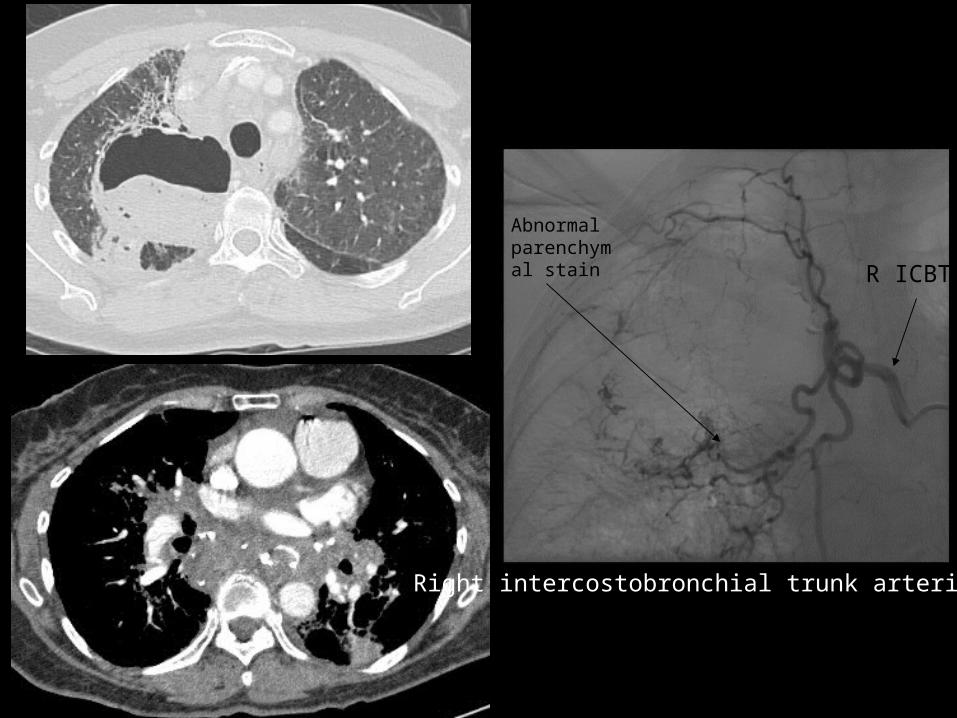
Right intercostobronchial trunk arteriogram
R ICBT
Abnormal parenchymal stain

Differential Diagnosis
Sarcoid/TB
Neoplasm
Airway trauma
Vasculitis
10
Presentation Title - Subtitle
Key Points10
Presentation Title - Subtitle
NOTABLE:
defined as >500cc hemoptysis in 24 hours
multiple causes, usually blood supply is by hypertrophied bronchial artery
CLASSIC DESCRIPTOR:
hypertrophied bronchial artery with abnormal parenchymal stain +/- shunting to pulmonary artery/vein
NB - active extravasation not commonly seen
PEARL:
mainstay of therapy is bronchial embolization – BEWARE THE ANTERIOR SPINAL ARTERY
Key Points
TREATMENT:
particle embolization of bronchial artery
no coils – won’t be able to treat recurrence
BEWARE THE ANTERIOR SPINAL ARTERYvariable bronchial artery anatomy
most commonly right intercostobronchial trunk, left bronchial artery
10
Presentation Title - Subtitle
Key Points - CLOSING
Sometimes surgery is the answer
Interventional options:
Embolization, covered stent, thrombin
Types of embolic agents:
permanent (PVA, glue, coils) vs temporary (gelfoam)
Coils are akin to surgical ligation
- “proximal” occlusion
- potential for collateral formation
Particles/glue
- “distal” occlusion, capillary/arteriolar level
- no collaterals, risk for ischemia
Presentation Title - Subtitle

CASES
CASE 1155 year old male, hepatoma screen
1111

Arterial phase Venous phase
Diagnosis?
Potential treatment options?
1111

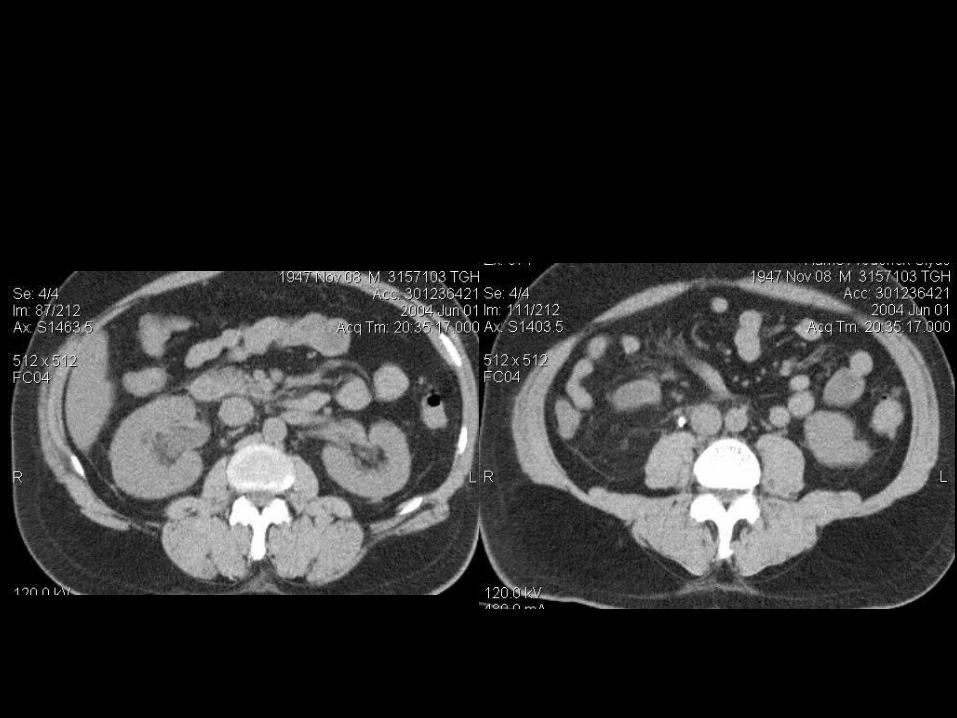
CASE 12:60 year old male with abdominal pain
1212
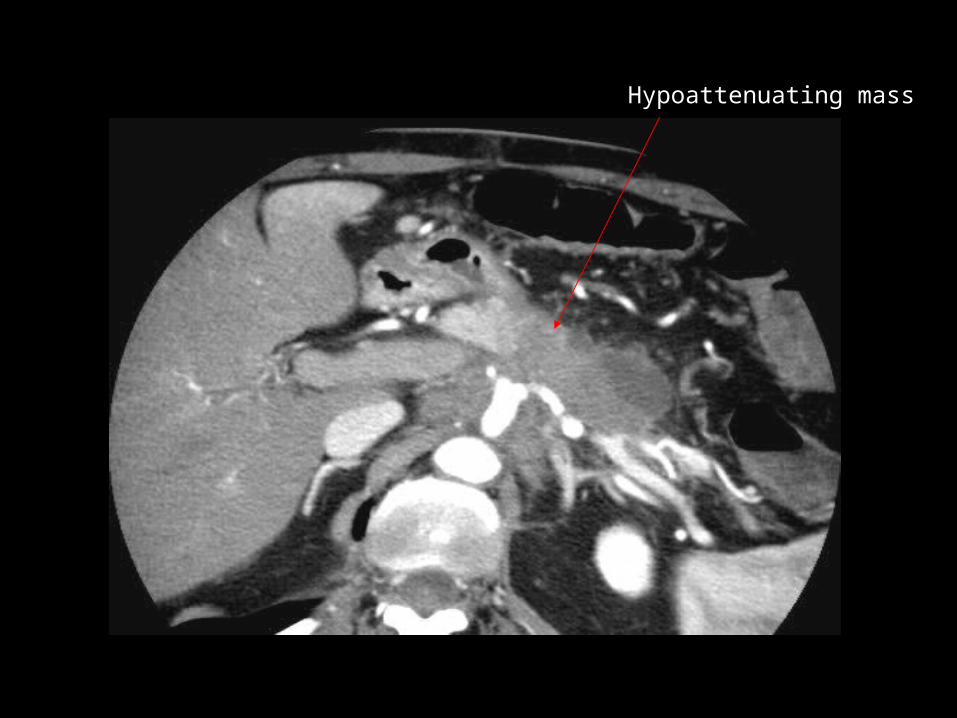
Hypoattenuating mass
Probable diagnosis?
What would be your approach to biopsy?
What are the risks of biopsy?
1212
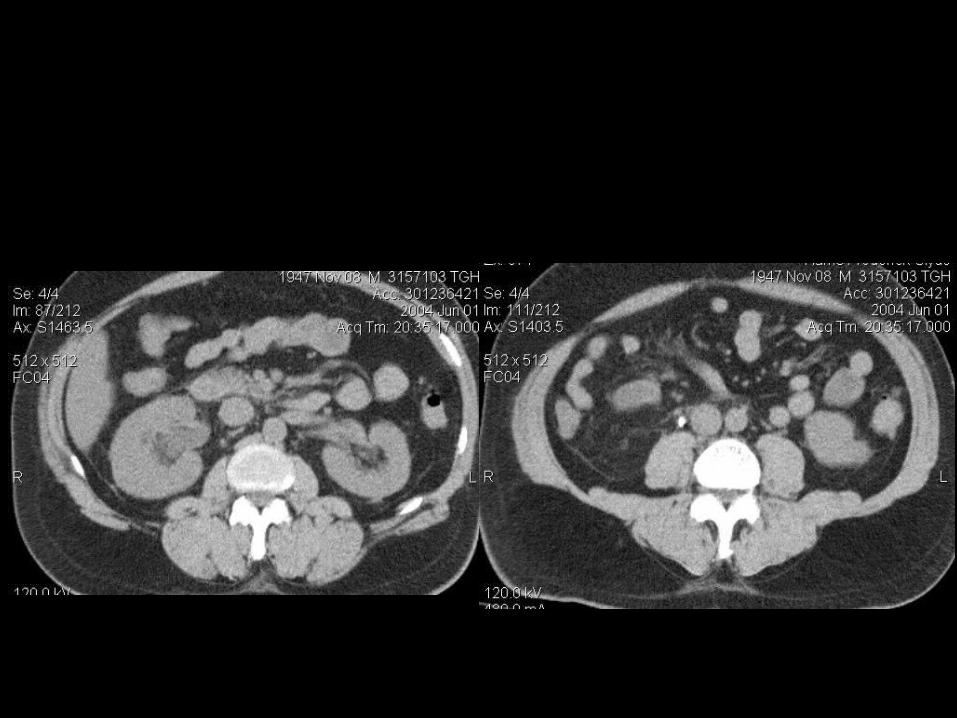
CASE 1357 year old male, right flank pain and fever
1313
Diagnosis?
How can a radiologist help?
What are the risks of percutaneous intervention?
1212
CASE 1460 year old male, left lower quadrant pain and fever
1414

Is this drainable?
Probable diagnosis?
Is this collection drainable?
What route/guidance method would you choose?
1212

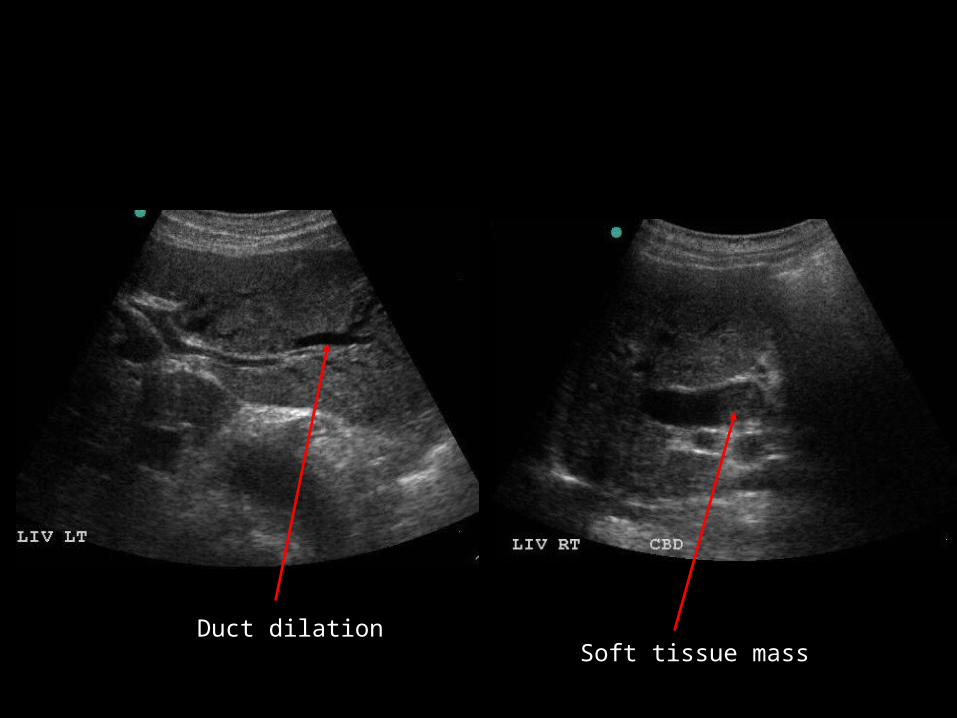
CASE 15: 70 year old female, fever and right upper quadrant pain
1515
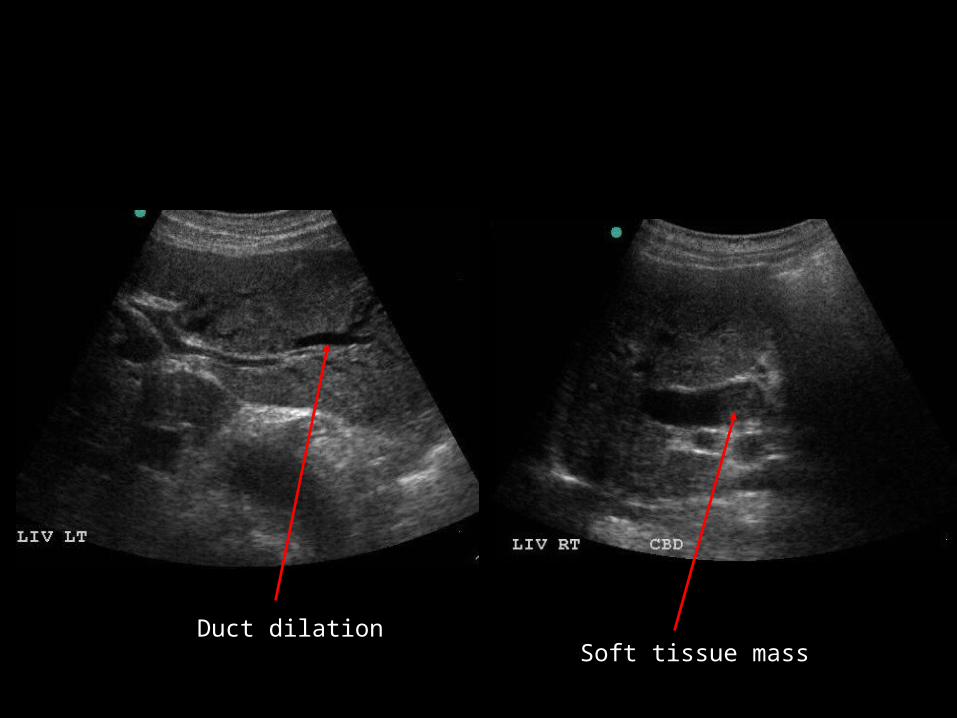
Soft tissue massDuct dilation
Probable diagnosis?
Treatment options?
What kind of tube would you use for percutaneous intervention?
1212

CASE REVIEW

1111
Case 11: HEPATOCELLULAR CARCINOMA

Differential Diagnosis
Dysplastic nodule
Hemangioma
FNH-like lesion
11
Presentation Title - Subtitle

Arterial phase Venous phase
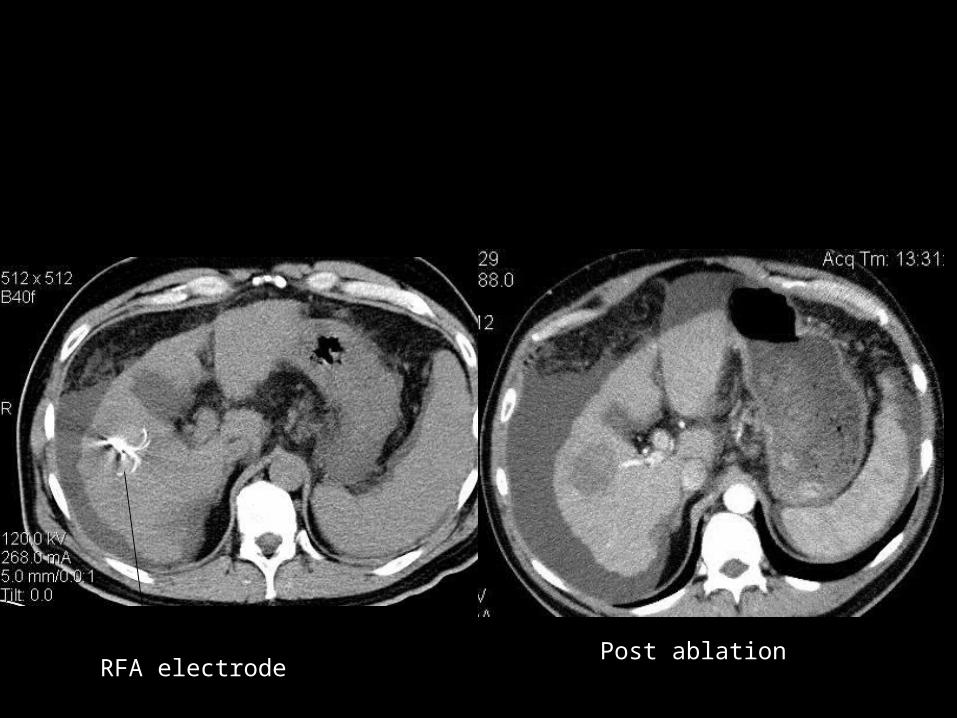
RFA electrodePost ablation
Key Points11
Presentation Title - Subtitle
NOTABLE:
Very common in far east, increased incidence in north america
CLASSIC DESCRIPTOR:
Arterially enhancing nodule with washout in cirrhotic liver
PEARL:
Any arterially enhancing lesion >2cm in a cirrhotic liver is HCC until proven otherwise
Only cure is liver transplantation
Key Points11
Presentation Title - Subtitle
TREATMENT:
Only curative treatment for HCC is transplant
Surgical resection for surgical candidates
RFA for non-surgical candidates
+/- lesions ≤ 2.5cm
chemoembolization
radiotherapy
sorafenib
Risks of RFA: hemorrage, infection, bile duct injury, needle tract seeding, colon/GB injury
1212
Case 12: PANCREATIC ADENOCARCINOMA
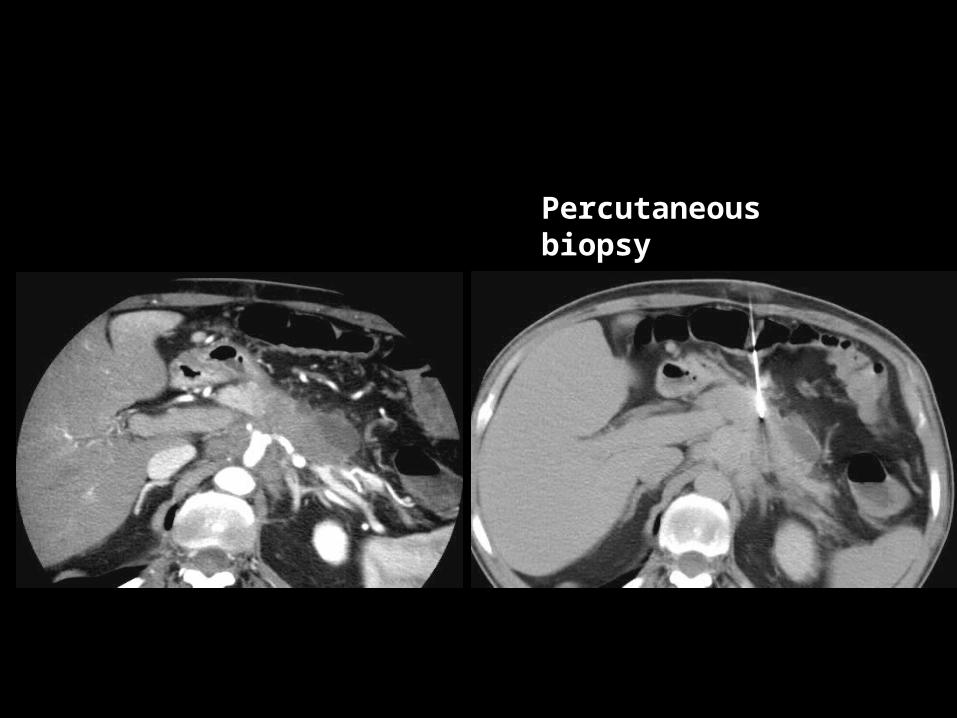
Percutaneous biopsy
Differential Diagnosis
Pancreatic adenoCa
Focal pancreatitis
Metastasis
12
Presentation Title - Subtitle

Key Points12
Presentation Title - Subtitle
NOTABLE:
most commonly present in pancreatic head.
CLASSIC DESCRIPTOR:
ill-defined hypoattenuating pass pancreatic head
PEARL:
Most unresectable
Key Points12
Presentation Title - Subtitle
PERCUTANEOUS BIOPSY:
ultrasound vs. CT guided
may go transgastric if needed
risks:
hemorrage
infection
tumour seeding very rare
bowel injury
coaxial technique
core biopsy preferred
1313
Case 13: PYELONEPHRITIS, OBSTRUCTING CALCULUS
Differential Diagnosis
Non-infected hydronephrosis
Pre-existing UPJ obstruction
13
Presentation Title - Subtitle

Key Points13
Presentation Title - Subtitle
NOTABLE:
99% of renal calculi depicted on non-contrast CT
Most calculi impacted at UVJ, UPJ or pelvic brim
CLASSIC DESCRIPTOR:
radioopaque calculus with associated renal enlargement, perinephric stranding, hydronephrosis/hydroureter
PEARL:
Infected calculi, hydronephrosis in solitary kidney or electrolyte disturbances are indications for urgent management

Key Points13
Presentation Title - Subtitle
TREATMENT:
renal decompression
urgently for sepsis, solitary kidney, electrolyte disturbance
options:
percutaneous nephrostomy/ nephroureterostomy
percutaneous JJ stent
cystoscopic JJ stent
risks of percutaneous therapy
worsening sepsis, hemorrhage/AVF, other organ injury
1414
Case 14: DIVERTICULAR ABSCESS
Differential Diagnosis
Perforated colon cancer
Abscess from inflammatory bowel disease
14
Presentation Title - Subtitle

Is this drainable?
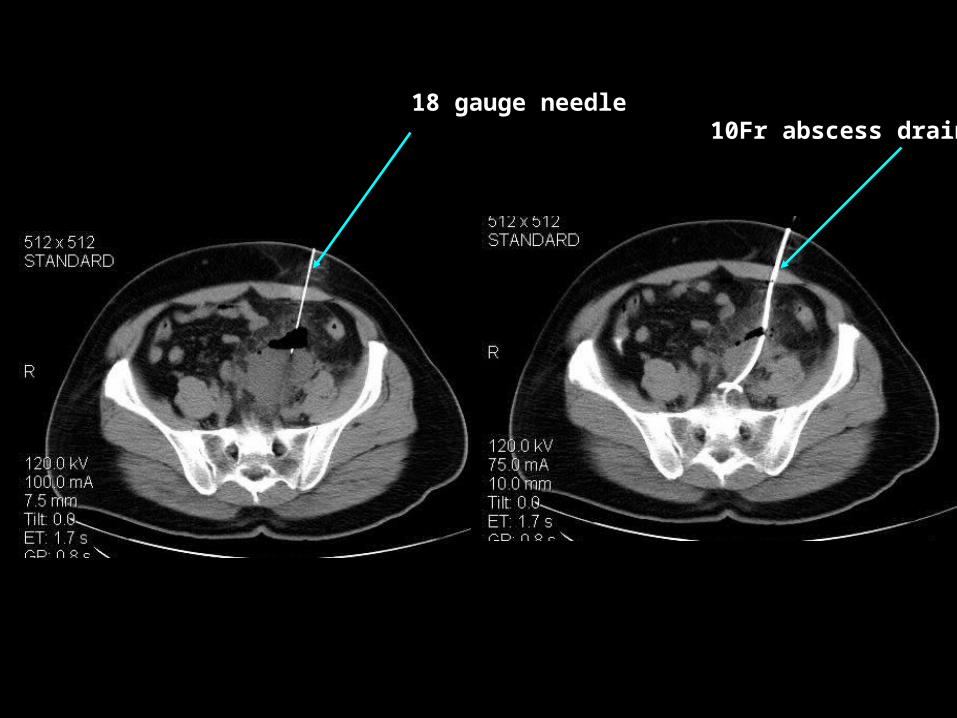
18 gauge needle10Fr abscess drain
Key Points14
Presentation Title - Subtitle
NOTABLE:
prevalence of diverticulosis @ 50% after age 70
complications include diverticulitis, fistula, muscular hypertrophy, lower GI bleed
CLASSIC DESCRIPTOR:
rim enahancing fluid collection in sigmoid mesentary, adjacent to inflamed diverticulum
PEARL:
always do elective sigmoidoscopy/colonoscopy to rule out underlying malignancy
Key Points14
Presentation Title - Subtitle
TREATMENT:
medical
antibiotics, often successful for small collections
surgery
two stage – hartman’s with colostomy, then reversal
percutaneous
definitive management
delay surgery to elective, 1-stage procedure

Key Points14
Presentation Title - Subtitle
PERCUTANEOUS TREATMENT:
US guidance – faster, safer
CT guidance – not all lesions can be seen by ultrasound
deep
gas obscuring view
Seldinger vs. Trochar
safer vs. faster, less painful
Tube size – 10 French or bigger for pus, thick bile, pleural fluid
Key Points14
Presentation Title - Subtitle
WHAT IS FRENCH SIZE?!?!?!:
Circumference of tube in mm
French size/3 = diameter
Eg. 8Fr tube is ~ 2.7mm
- suitable for simple fluid
1515
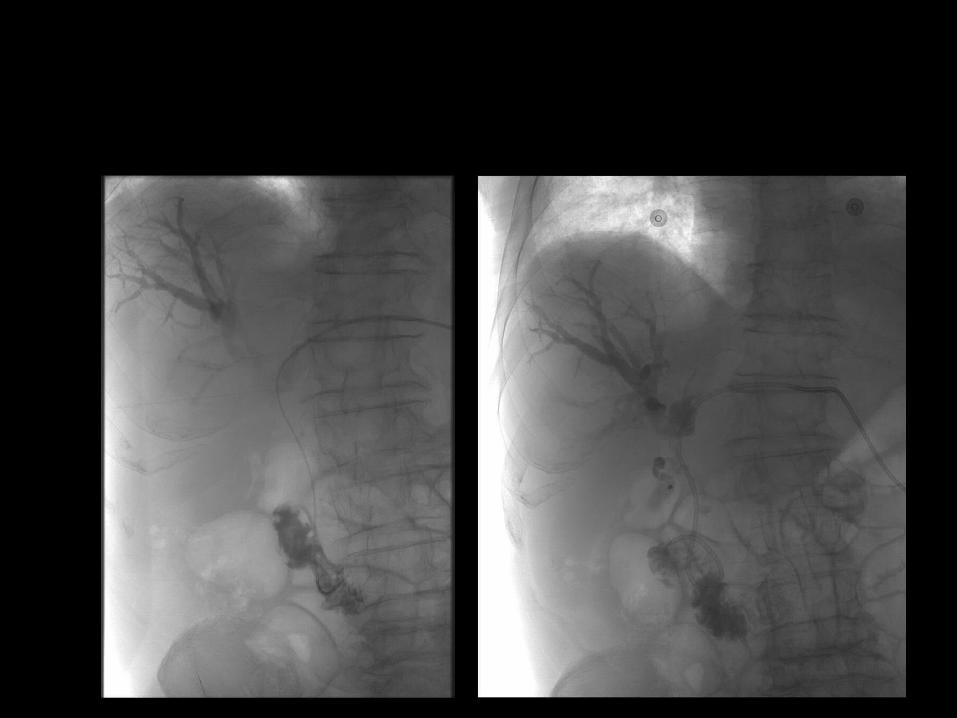
Case 15: KLATSKIN TUMOUR, BILE DUCT OBSTRUCTION
Soft tissue massDuct dilation
Differential Diagnosis
Cholangiocarcinoma
Biliary calculus
15
Presentation Title - Subtitle
Key Points15
Presentation Title - Subtitle
NOTABLE:
Hilar cholangiocarcinoma, known as klatskin tumour
Often unresectable
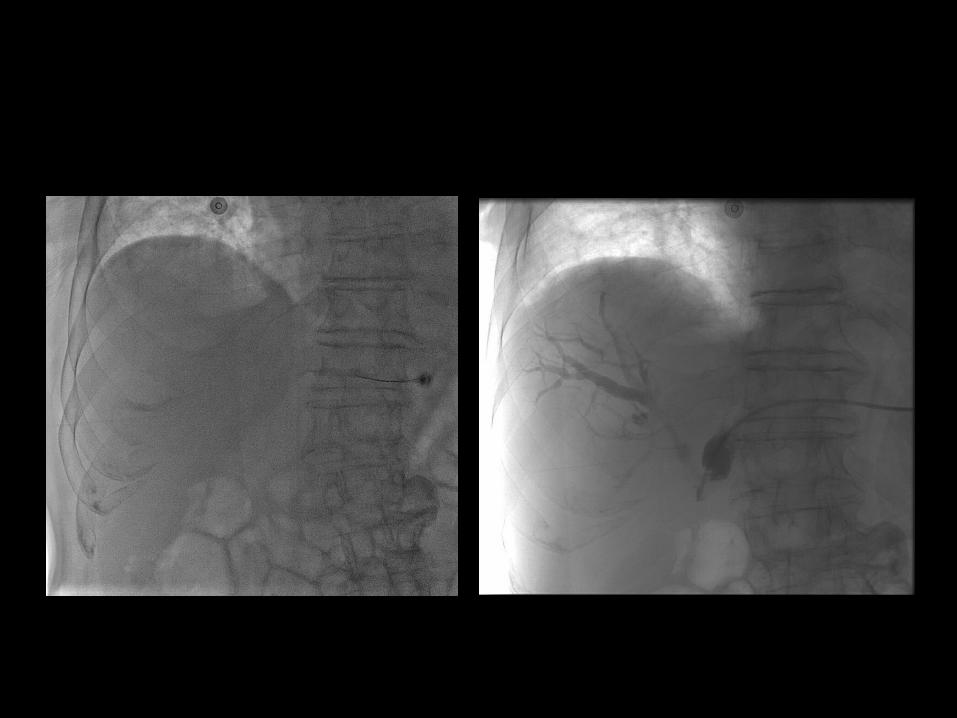
CLASSIC DESCRIPTOR:
Hilar soft tissue mass with bilateral biliary obstruction. Lack of communication of left and right sided ducts
PEARL:
Often require biliary drainage to restore bilirubin and allow safe administration of chemotherapy
Key Points15
Presentation Title - Subtitle
TREATMENT:
Medical
Surgical
Endoscopic
plastic stents
can’t be removed without endoscopy
limited access
more appropriate for low lesions
if the GB is distended – ERCP
Percutaneous

Key Points15
Presentation Title - Subtitle
PERCUTANEOUS TREATMENT:
Goal is to decompress as much liver as possible
Goal is internal drainage if possible
Internal/external biliary drainage catheter
minimize manipulation if cholangitis
Either side if right and left side communicate
Right side first vs. bilateral tubes if not
Key Points – NEEDLES/DRAINS
Presentation Title - Subtitle
Procedures are not without risk
Bleeding, infection, other organ injury
Internal drainage always desirable
US faster, safer when possible
Seldinger vs. trochar
- safer, slower, more painful
THANK YOU
Recommended