Validation of Commercially Available InfraredThermometers for Measuring Skin SurfaceTemperature Associated with Deep and
Surrounding Wound InfectionAsfandyar Mufti, BMSc; Patricia Coutts, RN;
and R. Gary Sibbald, BSc, MD, MEd, FRCPC(Med)(Derm), MACP, FAAD, MAPWCA, DSc(Hons)
ABSTRACTOBJECTIVE: Increased local skin temperature is a classic sign of
wound infection, repetitive trauma, and deep inflammation.
Noncontact infrared thermometers can help to detect increases in
skin surface temperatures; however, most scientifically tested
devices are far too expensive for everyday wound care providers
to use in routine clinical practice. This noninferiority study was
conducted in an attempt to determine whether 4 less expensive,
commercially available noncontact infrared thermometers have a
similar level of accuracy as the scientifically accepted Exergen
DermaTemp 1001 (Exergen Products, Watertown, Massachusetts).
DESIGN, SETTING, AND PARTICIPANTS: Using an observational
study design, participants with open wounds were randomly
selected from a chronic wound clinic (n = 108). Demographic data
and wound location were documented for all participants. Skin
temperatures were recorded using 5 noncontact infrared
thermometers under consistent environmental conditions. The
thermometer brands were as follows: Exergen DermaTemp,
Mastercool MSC52224-A (Mastercool Inc, Randolph, New Jersey),
ATD Tools 70001 Infrared Thermometer (ATD Tools Inc, Wentzville,
Missouri), Mastercraft Digital Temperature Reader (Mastercraft
Canada, Toronto, Ontario, Canada), and Pro Point Infrared
Thermometer (Princess Auto, Winnipeg, Manitoba, Canada). Data
analysis was based on the skin surface temperature difference
($T in degrees Fahrenheit) between the wound site and an
equivalent contralateral control site.
OUTCOME MEASURES: One-way analysis of variance was used
to compare the mean $T values for all the 5 thermometers,
followed by post hoc analysis. Demographic data were analyzed
using descriptive statistics. Interrater reliability was assessed
for consistency using the intraclass correlation coefficient.
MAIN RESULTS: No statistical difference was reported between
the $T values for the 5 different thermometers (F4,514 = 0.339,
P = .852). Post hoc analysis showed no significant difference when
the thermometers were compared with the Exergen DermaTemp
1001, and Mastercool MSC52224-A (P = .987), ATD Tools 70001
Infrared Thermometer (P = .985), Mastercraft Digital Temperature
Reader (P = .972), and Pro Point Infrared Thermometer (P = .774).
The results for intraclass correlation demonstrated a high
reliability and agreement between raters, as the intraclass correlation
coefficient values for all thermometers were greater than 0.95.
CONCLUSIONS: The results of this study demonstrate that less
expensive, industrial-grade noncontact infrared thermometers
have reliable temperature readings to identify and quantify the
temperature gradients that along with other signs may be
associated with deep and surrounding wound infection or tissue
injury due to repeated microtrauma.
KEYWORDS: infrared thermometers, wound infection, measuring
skin surface temperature
ADV SKIN WOUND CARE 2015;28:11Y6
INTRODUCTION/LITERATURE REVIEWTemperature plays a pivotal role in the body and its outer skin
covering to regulate metabolic and homeostatic processes. The
skin is the largest body organ that also serves as a barrier against
pathogens, contains nerve endings for sensation, acts as storage of
lipids and water, controls evaporation, and is involved in ther-
moregulation. The importance and relationship between body
ADVANCES IN SKIN & WOUND CARE & JANUARY 201511WWW.WOUNDCAREJOURNAL.COM
ORIGINAL INVESTIGATION
Asfandyar Mufti, BMSc, is a Medical Student, University of Ottawa Faculty of Medicine, Ottawa, Ontario, Canada. Patricia Coutts, RN, is Wound Care/Clinical Trials Coordinator, Toronto
Regional Wound Healing Clinic, Mississauga, Ontario. R. Gary Sibbald, BSc, MD, MEd, FRCPC (Med) (Derm), MACP, FAAD, MAPWCA, DSc (Hons), is Professor of Medicine and Public
Health, University of Toronto, Ontario, Canada; Director, International Interprofessional Wound Care Course & Masters of Science in Community Health (Prevention & Wound Care), Dalla
Lana School of Public Health, University of Toronto; Past President, World Union of Wound Healing Societies; Course Coordinator, International Interprofessional Wound Care Course at
New York University Medical Center; Clinical Editor, Advances in Skin & Wound Care, Philadelphia, Pennsylvania. The authors have disclosed they have no financial relationships related to
this article. Submitted August 27, 2014; accepted in revised form November 11, 2014. Editor’s note: For more information on how practitioners can incorporate infrared skin thermometry
for everyday wound care practice and also explore the potential for home use by patients with neuropathy to self-detect damage, see the Clinical Management Extra.

surface temperature and disease have been recognized by phys-
icians for centuries. As early as 400 bc, Hippocrates wrote, ‘‘In
whatever part of the body excess of heat or cold is felt, the disease
is there to be discovered.’’1 Changes in body surface temperature
can be a sign of infection, repetitive trauma, or deep inflammation,
along with less common thromboembolic processes and immune
and metabolic disorders.
Studies conducted by Armstrong et al2Y4 and Lavery et al5Y7
demonstrated the importance of self-monitoring skin temperature
in patients with diabetes, especially those at risk for lower-extremity
complications. These studies demonstrated that regions of elevated
temperature in individuals with diabetic neuropathy were more
likely to ulcerate, unless clinicians introduced aggressive preventive
strategies including plantar pressure redistribution, contact casts
(removable or irremovable), or pneumatic walkers.
More recently, Fierheller and Sibbald8 reported the relationship
between increased periwound skin temperature and local wound
infection in patients with chronic leg ulcers. Prolonged healing of
chronic wounds is a problem that causes tremendous patient dis-
tress and discomfort. Furthermore, delayed wound healing increases
the risk of additional complications and significantly adds to health-
care costs.9,10
Increased periwound temperature is a classic sign of wound in-
fection and is the most reliable clinical sign of deep and surrounding
skin infection, when analyzed with individual factor analysis of
the STONEES (size, temperature,os,new, exudate, erythema and
edema, smell) criteria.11 The quantitative measurement of skin tem-
perature as part of wound assessment facilitates the monitoring of
wound-associated deep and surrounding infection.11 It is impor-
tant to note, however, that an elevated temperature alone does
not necessarily mean that there is an infection. Two or more other
clinical features of the STONEES criteria are also needed that in-
clude increased size, probing or exposed bone, new areas of break-
down, erythema/edema = cellulitis, and increased exudate or smell.
The diagnostic accuracy of manual finger palpation to determine
skin temperature is very limited, especially because it is more sub-
jective than objective.12 Conventional mercury or electronic ther-
mometers are difficult to attach to the wound or periwound skin,
need time to be calibrated, and because of incomplete surface con-
tact are prone to inaccurate readings.13 A handheld nonYskin con-
tact infrared thermometer has the potential to provide an accurate,
objective, and quantitative comparative measurement of skin sur-
face temperature.13
The basic premise behind infrared thermometry is as follows: All
objects above the temperature of absolute zero release infrared
radiation.14 Heat released by inflammation is a form of infrared
radiation. When this infrared radiation hits a sensor in the ther-
mometer, the sensor converts this energy into a specific electrical
signal that corresponds to a given temperature. The higher the
temperature, the greater the infrared radiation received by the sen-
sor that outputs a larger temperature.
Most skin surface infrared thermometers used in everyday clin-
ical practice are of scientific study quality and too expensive for most
healthcare professionals to incorporate into practice. The authors’
goal is to test the accuracy of 4 less expensive commercially avail-
able infrared thermometers normally used for industrial machines
and automobiles. These thermometers will be compared with the
scientifically accepted Exergen DermaTemp 1001 infrared thermo-
meter (Exergen Products, Watertown, Massachusetts) utilized in
several peer-reviewed published studies.2Y7,15Y23
METHODS AND MATERIALSAn observational study design provided both an economic and
simple method for investigation. The Central Ethics Board approval
was obtained, and consenting participants were purposefully re-
cruited from within the patient population of a chronic wound clinic
using specific inclusion/exclusion criteria. One hundred eight patients
(n = 108) with wounds were measured for surface temperature.
Demographic data (eg, age, height, weight, gender, and ethnicity)
were also collected from all patients. Each limb was measured using
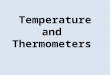
5 different devices (Table 1 and Figures 1 and 2).
(1) Exergen DermaTemp 1001;
(2) Mastercraft Digital Temperature Reader (Mastercraft Toronto,
Ontario, Canada);
Table 1.
INFRARED THERMOMETER SPECIFICATIONS
Device Measurement Range Operating RangeAccuracy (AmbientTemperature = 25-C)
Distance-to-Size Ratio
ContinuousScanning
‘‘Maximum’’Temperature
Exergen DermaTemp 1001 18-C to 43-C (65- F to 110- F) 16-CY43-C (60-FY110- F) T0.1-C (0.2- F) 1:1 Yes YesMastercraft DigitalTemperature Reader
j30-C to 480-C (j22-F to 896- F) 0-CY50-C (32- FY122- F) T2.0-C (4.0- F)a 8:1 Yes Yes
ATD Tools 70001Infrared Thermometer
j60-C to 550-C (j76- F to 1022- F) 0-CY50-C (32- FY122- F) T1.5-C (2.7- F) 12:1 Yes Yes
Pro Point InfraredThermometer
j60-C to 500-C (j76-F to 932- F) 0-CY50-C (32- FY122- F) T1.0-C (1.8- F) 12:1 Yes Yes
Mastercool MSC52224-A j58-C to 932-C (j50-F to 500- F) 0-CY40-C (32- FY104- F) T2.0-C (4.0- F) 12:1 Yes Yes
aAccuracy at ambient temperature 23-C.
ADVANCES IN SKIN & WOUND CARE & VOL. 28 NO. 1 12 WWW.WOUNDCAREJOURNAL.COM
ORIGINAL INVESTIGATION

(3) ATD Tools 70001 Infrared Thermometer (ATD Tools Inc,
Wentzville, Missouri);
(4) Pro Point Infrared Thermometer (Princess Auto, Winnipeg,
Manitoba, Canada); and
(5) Mastercool MSC52224-A (Mastercool Inc, Randolph,
New Jersey).
The Mastercool MSC52224-A was introduced 2 days late into
the study and was tested on a total of 87 patients (n = 87) over the
course of the study. Under consistent environmental conditions,
skin temperature data were obtained from both the target (wound
site) and contralateral control sites at a distance of 3 cm above
the skin using each of the thermometers for a total of 5 patient
recordings.
In the case of wounds located in the sacral region, the authors
compared the target temperature with an unwounded area above
or below the wound. This was a standard procedure for all wounds
that were anatomically located along the midline and did not have
a ‘‘contralateral’’ side as a comparator.
Temperature readings were made approximately 10 minutes
after removing the wound dressings. This delay was timed to avoid
heat collected under occlusive dressings or evaporation artifacts.
Using gun-shaped infrared thermometers in this study was easy
and intuitive. Once the trigger was depressed, real-time tempera-
ture acquisition started. The authors moved the thermometer over
and around the wound in a ‘‘grid pattern’’ to ensure that all regions
surrounding the wound were covered. The temperature was recorded
in degrees Fahrenheit for convenience of detecting temperature
differentials. The location of the wound and the contralateral site
was also recorded. The target temperature was subtracted from
the contralateral temperature, in order to obtain the temperature
difference/gradient: $T. To validate the interrater reliability of the
thermometer between clinicians, the principal investigator and an
experienced wound care nurse duplicated temperature readings
independently on 20 participants.
Participants were included if they (1) were 18 years or older, (2)
provided written informed consent, (3) participated in 1 study as-
sessment, and (4) had a wound. Participants were excluded if they
(1) were younger than 18 years, (2) were unable to consent due to
language barrier, or (3) had no current skin ulcer.
Data AnalysisStatistical analysis was conducted using SPSS Statistics 22 for
Windows (IBM, Armonk, New York). A 1-way analysis of variance
compared the mean $T between the 5 different thermometers.
Figure 1.
COMMERCIAL LOWER COST INFRARED THERMOMETERS WITH ESTIMATED US DOLLAR COST
ADVANCES IN SKIN & WOUND CARE & JANUARY 201513WWW.WOUNDCAREJOURNAL.COM
ORIGINAL INVESTIGATION

Post hoc analysis was conducted using Tukey test to compare
4 different thermometers, with the DermaTemp Exergen 1001 as
the criterion standard. Interrater reliability of the 5 different thermo-
meters was analyzed using intraclass correlation coefficient. Further-
more, a 2-way mixed model was selected for analysis. The authors
used an > level of .05 as the cut-off point for all test significance.
RESULTSA total of 188 patients (n = 108) participated in the study. The
study population consisted of 61 men (n = 61) and 47 women
(n = 47). All demographic data were reported by the patient. The
mean age ranged from 26 to 94 years (mean, 62.9 [SD, 15.55] years).
The weight ranged from 100 to 480 lb (mean, 194.68 [SD, 66.23] lb).
The reported height ranged from 60 to 80 inches (mean, 67.93 [SD,
4.32] inches). The wound duration varied from 5 days up to 6 years
(mean, 21.49 [SD, 18.2] months). Forty-four percent (n = 47) of the
participants were diagnosed with diabetes at the time of their visit.
Eighty-nine percent (n = 42) of these patients had type 2 diabetes.
The study wounds had a wide variety of etiologies (Figure 3).
A 1-way analysis of variance yielded no significant difference
between the 5 different thermometers in regard to the $T value
(F4,514 = 0.339, P = .852). Post hoc analysis using Tukey honest
significant difference indicated that the DermaTemp thermometer
did not have a significantly different$T value when compared with
Mastercool MSC52224-A (P = .987), ATD Tools 70001 Infrared
Thermometer (P = .985), Mastercraft Digital Temperature Reader
(P=.972), and Pro Point Infrared Thermometer (P= .774). The mean
$T value for each thermometer is indicated in Table 2.
The interrater reliability was examined with the calculation of
the intraclass correlation coefficient. for each thermometer. There
was a high level of consistency and agreement between the 2 clin-
icians and the 5 thermometers (Table 3).
DISCUSSIONThis clinical study was conducted to demonstrate that readily avail-
able infrared thermometers have an acceptable accuracy for clinical
practice. The statistical analysis of periwound temperature data
strongly supports the reliability between thermometers and
Figure 2.
COMPARISON OF INFRARED THERMOMETER SCREENS SHOWING DESIRED MAXIMUM READING, FARENHEIT SCALE
AND SCANNING MODE
ADVANCES IN SKIN & WOUND CARE & VOL. 28 NO. 1 14 WWW.WOUNDCAREJOURNAL.COM
ORIGINAL INVESTIGATION

operators of less expensive devices when compared with DermaTemp
Exergen 1001. The strong interrater reliability that was obtained for all
5 thermometers confirms that the less expensive thermometers give
similar temperature readings, regardless of the operator.
The study thermometers had valuable bedside tool features. All
the thermometers had real-time scanning features. Thus, once the
temperature acquisition started, the temperature would change as
the thermometer was moved across a surface instead of pressing
the button each time the operator moved to a new location. Ar-
guably the most important feature in these thermometers is the
‘‘maximum temperature recorded’’ function. During the course of
temperature acquisition, it is difficult for the clinician to remem-
ber the maximum temperature that was observed over and around
the wound. This is because skin surface temperature is variable
Figure 3.
Table 2.
THEMEANTEMPERATUREGRADIENTSOFTHE5 DIFFERENT THERMOMETERS
Thermometer Mean ‘‘$T’’
Exergen DermaTemp 1001 2.39- F (SD, 3.54- F)Mastercool MSC52224-A 2.68- F (SD, 4.06- F)a
ATD Tools 70001 Infrared Thermometer 2.67- F (SD, 3.93- F)b
Mastercraft Digital Temperature Reader 2.72- F (SD, 4.26- F)c
Pro Point Infrared Thermometer 3.01- F (SD, 3.90- F)d
aP = .987.bP = .985.cP = .972.dP = .774.
Table 3.
INTERRATER RELIABILITY ASSESSED USINGINTRACLASSCORRELATIONCOEFFICIENT(ICC)
Thermometer ICCa
Exergen DermaTemp 1001 0.967 (0.92Y0.987)ATD Tools 70001 Infrared Thermometer 0.970 (0.925Y0.988)Pro Point Infrared Thermometer 0.969 (0.922Y0.987)Mastercool MSC52224-A 0.968 (0.92Y0.987)Mastercraft Digital Temperature Reader 0.952 (0.884Y0.981)
a95% Confidence interval values stated in parenthesis.
ADVANCES IN SKIN & WOUND CARE & JANUARY 201515WWW.WOUNDCAREJOURNAL.COM
ORIGINAL INVESTIGATION

over a given surface area and may depend on vascular supply,
inflammation, and infection. The authors’ previous work has
already demonstrated that a temperature difference of greater
than 3-F between a wound and mirror anatomical site, along
with 2 or more other clinical signs, is highly suggestive of deep
infection.8 Individual factor analysis for the clinical signs in the
7 STONEES criteria identified an elevated temperature to be
8 times more likely associated with deep and surrounding infec-
tion. All of the other 6 signs were 2 to 5 times more likely.8 In fact,
the elevated temperature gradient is one of the most important
indications of deep and surrounding infection. Although tempera-
ture elevation is suggestive of deep infection, it is also indicative of
other causes of tissue damage. In the case of tissue damage, it is
important to correct the cause and prevent further tissue damage.
Systemic antibiotics should be ordered only when there is a deep
and surrounding tissue infection.
An important feature of the infrared thermometers in this study
is the distance-to-spot ratio. As the name suggests, this is a ratio
between the distance to the object and the diameter of the object.
For instance, if a device has a distance-to-spot ratio of 8:1, what
this implies is that if the infrared thermometer was 8 inches away
from the wound, the highest temperature within a 1-inch diameter
of the wound surface would be recorded. The closer the thermo-
meter is to the wound, the smaller the diameter of skin tempera-
ture differential that will be recorded. For a smaller wound, better
temperature discrimination occurs in a smaller diameter if the
thermometer is closer to the wound but not touching. The non-
contact infrared thermometers tested in this study may help prevent
the spread of infection. This is because of the higher distance-to-
spot ratio, compared with the Exergen DermaTemp 1001, and
the thermometers did not need to be too close to the wound, avoid-
ing accidental contact and the risk of contaminating other wounds
with subsequent examinations. In the authors’ experience, the
Exergen DermaTemp 1001 examination will cause wound care pro-
viders to accidently touch portions of the wound that could be a
cause of future contamination to other patients. The thermometers
should be swabbed with alcohol or other disinfectants between
examinations.
Some of these thermometers also have a laser pointer. It is a
common misconception that the laser pointer reads the tempera-
ture. It is most important to ensure that the aperture of the infrared
thermometer is pointing at the wound and surrounding surface.
Depending on the model of the infrared thermometer, temperature
will be read above, below, or around the laser pointer. Another
common misconception about infrared thermometers is that they
provide information regarding internal temperature. This is abso-
lutely false. Infrared thermometers are only skin surface tempera-
ture tools.
CONCLUSIONSThe results of this study demonstrate that less expensive, industrial-
grade noncontact infrared thermometers possess reliable temper-
ature readings that identify and quantify temperature gradients in
the periwound skin. This study further demonstrates that infrared
thermometers can add objectivity to the time-honored subjective
method of clinical palpation for elevated skin temperature asso-
ciated with deep and surrounding wound infection.
REFERENCES1. Chambliss J. Case of traumatic femoral aneurism (sic) treated by digital compression-ligation
afterwards of the external iliac artery. Confederate States Med Surg J 1864;1:97-9.
2. Armstrong DG, Lavery LA, Liswood PJ, Todd WF, Tredwell JA. Infrared dermal thermometry
for the high-risk diabetic foot. Phys Ther 1997;77:169-75.
3. Armstrong DG, Lavery LA. Predicting neuropathic ulceration with infrared dermal thermometry.
J Am Podiatr Med Assoc 1997;87:336-7.
4. Armstrong DG, Holtz-Neiderer K, Wendel C, Mohler MJ, Kimbriel HR, Lavery LA. Skin temperature
monitoring reduces the risk for diabetic foot ulceration in high-risk patients. Am J Med 2007;
120:1042-6.
5. Lavery LA, Higgins KR, Lanctot DR, et al. Home monitoring of foot skin temperatures to prevent
ulceration. Diabetes Care 2004;27:2642-7.
6. Lavery LA, Higgins KR, Lanctot DR, et al. Preventing diabetic foot ulcer recurrence in high-risk
patients: use of temperature monitoring as a self-assessment tool. Diabetes Care 2007;30(1):14-20.
7. Lavery LA, Peters EJ, Armstrong DG. What are the most effective interventions in preventing
diabetic foot ulcers? Int Wound J 2008;5:425-33.
8. Fierheller M, Sibbald RG. A clinical investigation into the relationship between increased
periwound skin temperature and local wound infection in patients with chronic leg ulcers. Adv
Skin Wound Care 2010;23:369-79.
9. Dow G. Bacterial swabs and the chronic wound: when, how, and what do they mean? Ostomy
Wound Manage 2003;49(5A Suppl):8-13.
10. Bowler PG, Duerden BI, Armstrong DG. Wound microbiology and associated approaches to
wound management. Clin Microbiol Rev 2001;14:244-69.
11. Robson MC. Wound infection. A failure of wound healing caused by an imbalance of bacteria.
Surg Clin North Am 1997;77:637-50.
12. Murff RT, Armstrong DG, Lanctot D, Lavery LA, Athanasiou KA. How effective is manual palpation
in detecting subtle temperature differences? Clin Podiatr Med Surg 1998;15:151-4.
13. Romanelli M, Gaggio G, Coluccia M, Rizzello F, Piaggesi A. Technological advances in wound
bed measurements. Wounds 2002;14(2):58-66.
14. Blundell S, Blundell K., Concepts in Modern Physics. Oxford, England: Oxford University Press; 2006.
15. Armstrong DG, Lavery LA. Monitoring healing of acute Charcot’s arthropathy with infrared
dermal thermometry. J Rehabil Res Dev 1997;34:317-21.
16. Armstrong DG, Todd WF, Lavery LA, Harkless LB, Bushman TR. The natural history of acute
Charcot’s arthropathy in a diabetic foot specialty clinic. J Am Podiatr Med Assoc 1997;87:272-8.
17. Armstrong DG, Lavery LA. Acute Charcot’s arthropathy of the foot and ankle. Phys Ther 1998;
78(1):74-80.
18. Armstrong DG, Lavery LA, Wu S, Boulton AJ. Evaluation of removable and irremovable cast
walkers in the healing of diabetic foot wounds: a randomized controlled trial. Diabetes Care
2005;28:551-4.
19. Armstrong DG, Lipsky BA, Polis AB, Abramson MA. Does dermal thermometry predict clinical
outcome in diabetic foot infection? Analysis of data from the SIDESTEP* trial. Int Wound J 2006;
3:302-7.
20. Burns J, Ouvrier RA, Yiu EM, et al. Ascorbic acid for Charcot-Marie-Tooth disease type 1A in
children: a randomised, double-blind, placebo-controlled, safety and efficacy trial. Lancet
Neurol 2009;8:537-44.
21. Foltz KD, Fallat LM, Schwartz S. Usefulness of a brief assessment battery for early detection
of Charcot foot deformity in patients with diabetes. J Foot Ankle Surg 2004;43(2):87-92.
22. McGuiness W, Vella E, Harrison D. Influence of dressing changes on wound temperature.
J Wound Care 2004;13:383-5.
23. Petrova NL, Moniz C, Elias DA, Buxton-Thomas M, Bates M, Edmonds ME. Is there a systemic
inflammatory response in the acute Charcot foot? Diabetes Care 2007;30:997-8.
ADVANCES IN SKIN & WOUND CARE & VOL. 28 NO. 1 16 WWW.WOUNDCAREJOURNAL.COM
ORIGINAL INVESTIGATION
Recommended