VAGINAL MYOMECTOMY IN TREATMENT OF UTERINE
FIBROIDS.
K.V. Mekoshvili, E.B. Troik, S.V. Vardanyan,
B.L. Tsivyan.
Department of Obstetrics and Gynecology, City Hospital 40,
Saint Petersburg, Russia.
23rd ESGE Congress Brussels BE
25.09.2014

The History
Vaginal myomectomy was the first described by James Murphy in 1893.
D. O. Ott is the famous Russian gynecologist, reported 50 fibroids cases that were successfully performed by vaginal route from 1898 to 1912.
( D.O.Ott, Operative gynecology, 1912)

Design: Retrospective and prospective study.
Object: To establish the feasibility, safety and clinical effectiveness of vaginal myomectomy in comparison with laparoscopic and traditional approaches.
Patients: 61 women with symptomatic myomas who refused hysterectomy and/or desired to become pregnant.

Preoperative investigations
Anamnesis
Clinical - laboratory examination
US
MRI

Сharacteristics of the fibroids
Form of the fibroids:
Subserous - 19 (31%).
Intramural and subserous - 42 (68%).
Location:
Posterior wall - 31 (51%).
Fundal - 14 (23%).
Combined -16 (26 %).
Number of fibroids:
1- 18 (29,5%)
2- 13(21,3%)
>2- 30 (49%)
Weight of excised fibroids, g.(M+/-SD) 124,5±35,78
Diameter of dominant fibroid, cm.(M+/-SD) 8,6 ±1,3.

Indications for surgical treatment
Menorrhagia in 27 (44%) of cases.Pelvic pain in 8 (13%) of cases.Rapid growth in 11 (18%) of cases.Recurrent pregnancy loss in 6 (9,8%) of cases. Primary infertility in 17 (27,8%) of cases.Secondary infertility in 5 (8%) of cases.

The first study group comprised 18 patients underwent vaginal myomectomy.
.

The control groups
Second study group comprised 24 patients underwent laparoscopic myomectomy.
Third study group comprised 19 patients underwent laparotomic myomectomy.

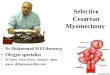
Surgical Technique
Steps:
1. Infiltration of posterior vaginal wall by vasoconstrictor solution.
2. Posterior colpotomy.

3. Removal body uterus with
myoma into the vagina
a. b.

4. Removing of the myoma(s)

5. Suturing the uterine wall
6. Moving the uterus back inside and draining the abdominal cavity
7. Suturing the vaginal wall.

Main results
Characteristics
Operative way
Blood loss
Operating time
Vaginal (n=18).
113,61±67,12 63,61±32,84
Laparoscopic (n=24)
135±97,08 114,58±48,09
Laparotomic (n=19)
246±113,18 97±33,60
Length of hospital stay 3,6±1,4. 4,2 ±1,1. 5,35 ±1,2.

VAS pain score
Vaginal group-
3,5±0,9.
Laparoscopic group-
3,3 ±1,3.
Laparotomic group-
4,7 ±1,3.

Complications
Intraoperative complications - 1 case
(5,5%) in vaginal group (injury of small
intestine.)
Postoperative complications - 0 case.
Conversion to laparotomy - 0 case.

Comparison current and previous studies in vaginal myomectomy.
Source. No of patients.
Blood loss, ml Operative time, min
Hospital stay, days
Bowel injury
No. of conversionsto laparotomy
Current, n=18
113,61±67,12 63,61±32,84 3,6±1,4. 1 0
Rolli R2012n= 46
data not available
70 (30-120) 1 (1-6) 0 2
Yu X2011n=43
78.3 ± 64.4 66.4 ± 22.6 4.9 ± 3.3 0 0
Plotti 2008n=18
210 (350) 48±22 3,5±2,4 0 1
Carminati 2006n=54
80 (20–350) 80 (30–170) 2 (1-3) 0 0

Subsequent Fertility
Operative way No. ofpregnancies
Method of delivery
Vaginal 4 (22.2%)spontaneously
1-Vaginal
3- Cesarean section
Laparoscopic 7 (29,16 %) 4-spontaneously 3- ART
6- Cesarean section
1- Elective abortion
Laparotomic 2 (10,2%) spontaneously
2- Cesarean section

Fertility after vaginal myomectomy (current and previous studies)
Source No. ofpregnancies
Method of delivery
Currentn= 18
4 (22,2%) 1- Vaginal
3- Cesarean section
Plotti n= 18
3 (16,6%) 1- Elective abortion
2 - Vaginal
Daviesn=35
3 (8,57%) 1 - Vaginal
2- Cesarean section
Rovion=10
3 (30%) 2 - Vaginal
1- Cesarean section
Carminatin=54
6 (11,1%) data not available.

Advantages of vaginal myomectomy
Vaginal myomectomy as laparoscopy may offer same advantages:
low intraoperative blood loss
less trauma
short recovery time in comparison with laparotomy.

Advantages of vaginal myomectomy
In addition
Short operating time is the benefit of this surgical aproach.
The quality of uterine suturing is better (in comparison with laparoscopy).
Morcelation is no necessary.

Main conditions for successful operation = features for selection of patients
Mobility of the uterus (parous women).
Localization of myomas – fundus and posterior
uterine wall
Size of myomas < 8 cm.
Number of myomas ≤ 5.
No pathologic pelvic adhesions, no associated
adnexal disease

Conclusions
Vaginal myomectomy in selected cases is a feasible, safe and effective surgical procedure. This approach may be an alternative to laparoscopic and traditional routes in surgery to treat uterine fibroids.

Thank you for your attention
Recommended