Utilization Of Lean Process Improvement During Introduction Of Stereotactic Body Radiotherapy And Radiosurgery To Decrease Patient Rescheduling
Nitika ThawaniDepartment of Radiation OncologyAssistant Professor, Department of RadiologyTexas A&M College of MedicineScott & White Healthcare System
Sep 14, 2013
Overview
Introduction- Why we needed this?
Materials/Methods- How we went about doing this?
Results- How it changed our practice?
Discussion- How we compare to others?
Future directions-------------------------
2
3
Introduction
Stereotactic Body Radiotherapy(SBRT) and Radiosurgery (SRS)- specialized forms of radiotherapy. High doses are delivered over a small number of treatment fractions
Treatment requires extreme precision as very high doses of radiation are delivered over short period of time
Potential for a high price to pay for small errors
Multidisciplinary care mandated so that complex treatment modalities can provide safe and expeditious care to patients
4
Introduction
The Radiosurgery program at Scott and White Healthcare system was introduced in 4/2010
The patient need in Central Texas led to a high volume of patients over a short timeframe leading to a high rescheduling rate(RSR)
High RSR can potentially lead to decreased patient and employee satisfaction, increased costs, poor outcomes and rework
5
Introduction
Lean thinking is a management philosophy developed from the manufacturing industry, initially pioneered and championed by Toyota Motor Corporation
The objective is “ to deliver maximum value to the customer while consuming the fewest resources by eliminating waste and reducing lead time”
6
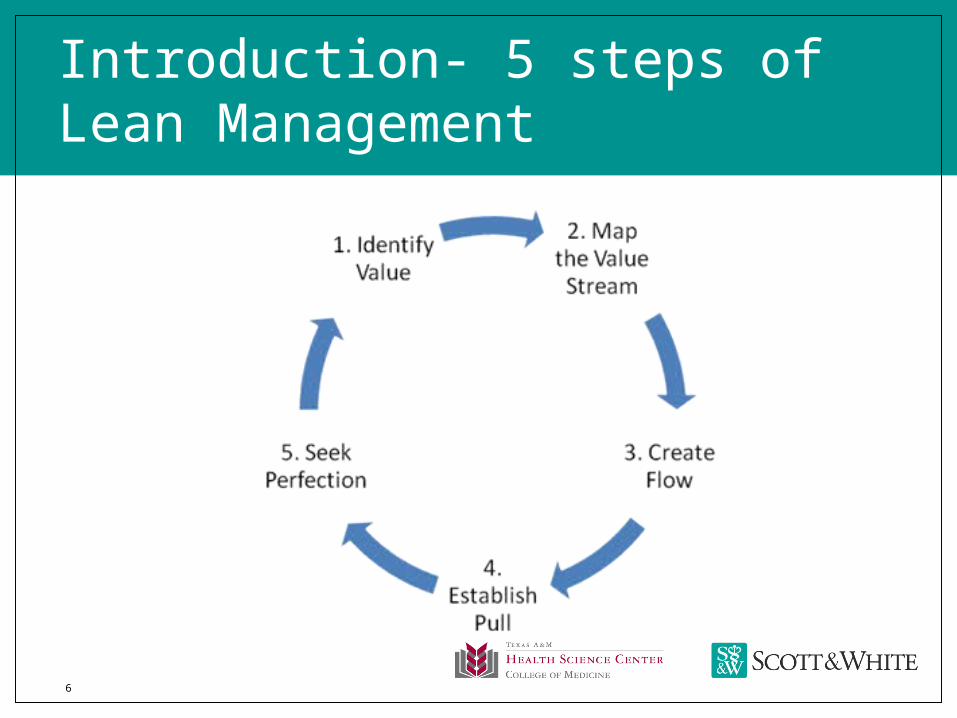
Introduction- 5 steps of Lean Management
7
Material/ Methods
Data on rescheduling along with the reasons for rescheduling were collected on all patients
Data from 5/2012 to 7/2012 was used to define the problem
A team including scheduling, nursing, therapy (simulation and treatment delivery), physics and physicians, used A3 structured problem solving for each step of the workflow
8
Materials/ Methods
1. Develop a Current state value stream map (CVSM) for the treatment flow. UDE( undesirable effects were recorded at each step)
2. Designed the Future state value Stream map(FSVSM)
Kaizens- (continuous, incremental improvement of an activity to create more value with less muda) were recorded for each step
3. Detailed work plan was created for implementing the FSVSM. Each member of the team assigned specific tasks with timelines
9
Materials/ Methods
Data was collected from 9/2012- 12/2012 to assess improvement-
1.Rescheduling rates
2.Treatment start times ( time from patient check in to start of treatment)
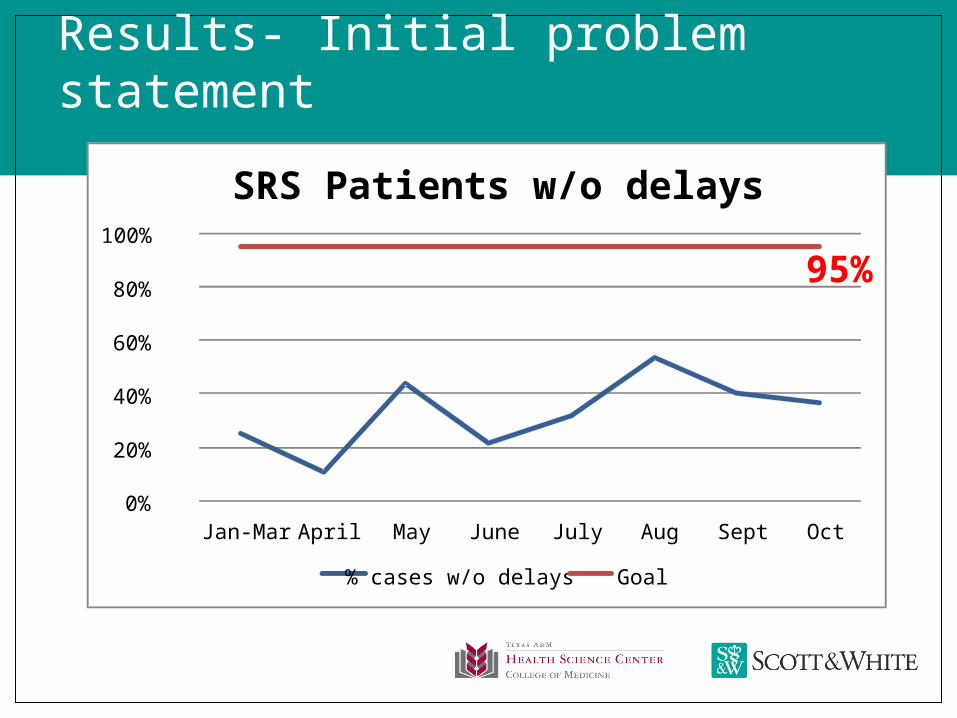
Results- Initial problem statement
0%
20%
40%
60%
80%
100%
Jan-Mar April May June July Aug Sept Oct
SRS Patients w/o delays
% cases w/o delays Goal
95%
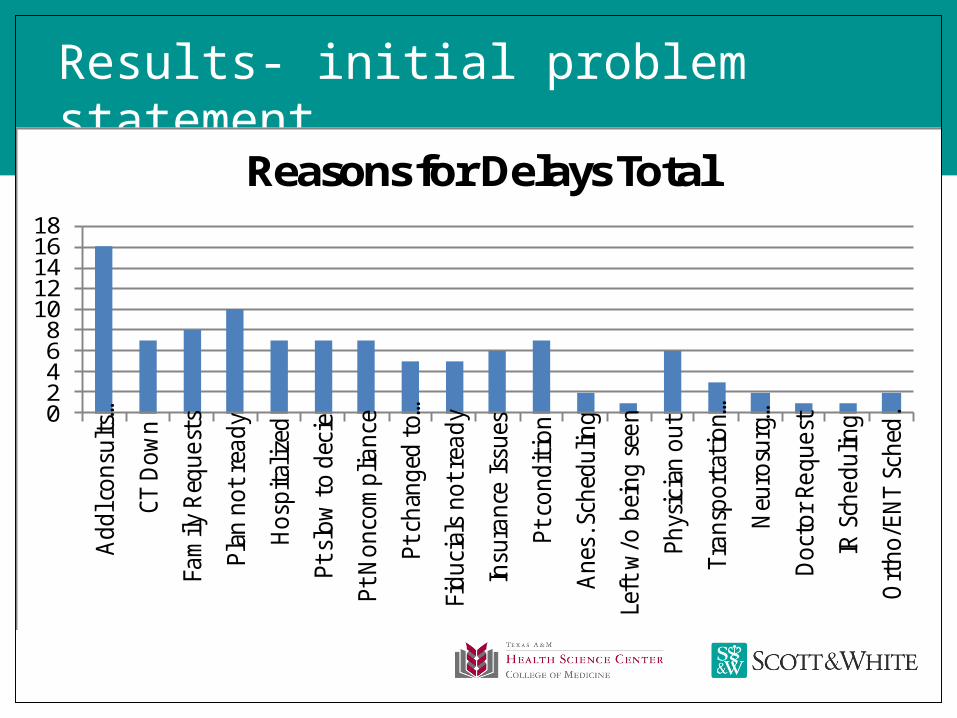
Results- initial problem statement
02468
1012141618
Add
l con
sults
…
CT D
own
Fam
ily R
eque
sts
Plan
not
rea
dy
Hos
pita
lized
Pt s
low
to
deci
e
Pt N
onco
mpl
ianc
e
Pt c
hang
ed t
o…
Fidu
cial
s no
t rea
dy
Insu
ranc
e Is
sues
Pt c
ondi
tion
Ane
s. S
ched
ulin
g
Left
w/o
bei
ng s
een
Phys
icia
n ou
t
Tran
spor
tati
on…
Neu
rosu
rg…
Doc
tor
Requ
est
IR S
ched
ulin
g
Ort
ho/E
NT
Sche
d.
Reasons for Delays Total
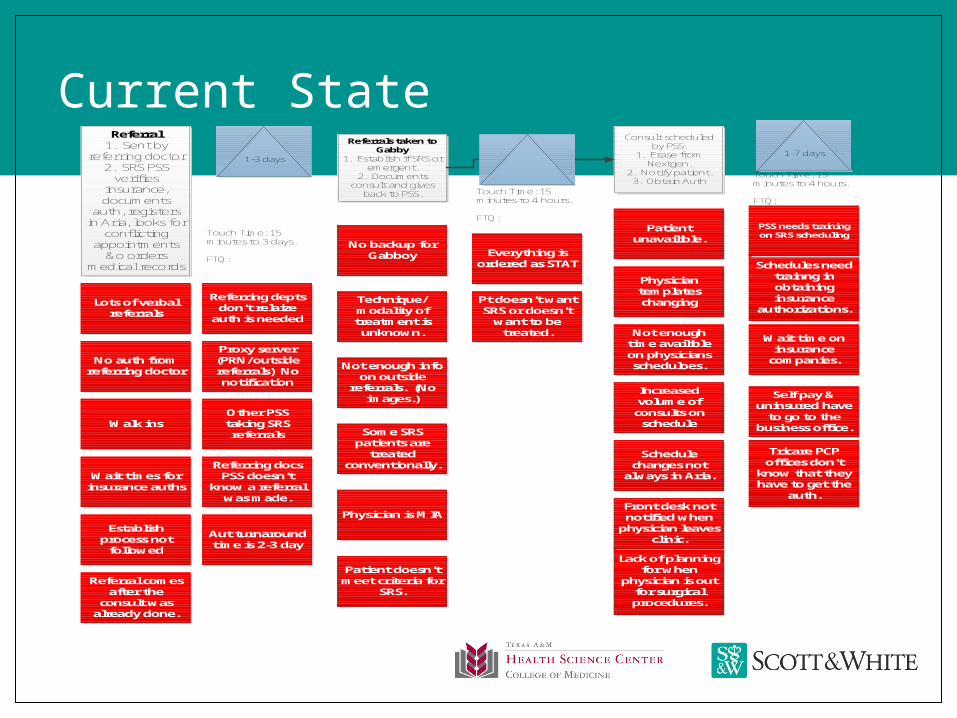
Current StateReferral
1. Sent by referring doctor
2. SRS PSS verifies
insurance, documents
auth, registers in Aria, looks for
conflicting appointments
&o orders medical records
Referring docs PSS doesn’t
know a referral was made.
Referring depts don’t relaize
auth is needed
Aut turnaround time is 2-3 day
Other PSS taking SRS referrals
Proxy server (PRN/outside referrals) No notification
Establish process not
followed
Wait times for insurance auths
Walk ins
No auth from referring doctor
Lots of verbal referrals
Referral comes after the
consult was already done.
Touch Time: 15 minutes to 3 days.
FTQ:
Referrals taken to Gabby
1. Establish if SRS or emergent.
2. Documents consult and gives
back to PSS.
Not enough info on outside
referrals. (No images.)
Technique/modality of treatment is
unknown.
No backup for Gabboy
Physician is MIA
Some SRS patients are
treated conventionally.
Patient doesn’t meet criteria for
SRS.
Pt doesn’t want SRS or doesn’t
want to be treated.
Touch Time: 15 minutes to 4 hours.
FTQ:
Consult scheduled by PSS.
1. Erase from Nextgen.
2. Notify patient. 3. Obtain Auth
Lack of planning for when
physician is out for surgical procedures.
Front desk not notified when
physician leaves clinic.
Schedule changes not
always in Aria.
Increased volume of
consults on schedule
Not enough time availible on physicians scheduloes.
Physician templates changing
Patient unavailible.
Wait time on insurance
companies.
Tricare PCP offices don’t
know that they have to get the
auth.
Self pay & uninsured have
to go to the business office.
Schedules need trainng in obtaining insurance
authorizations.
PSS needs training on SRS scheduling
Touch Time: 15 minutes to 4 hours.
FTQ:
Everything is ordered as STAT
1-3 days1-7 days
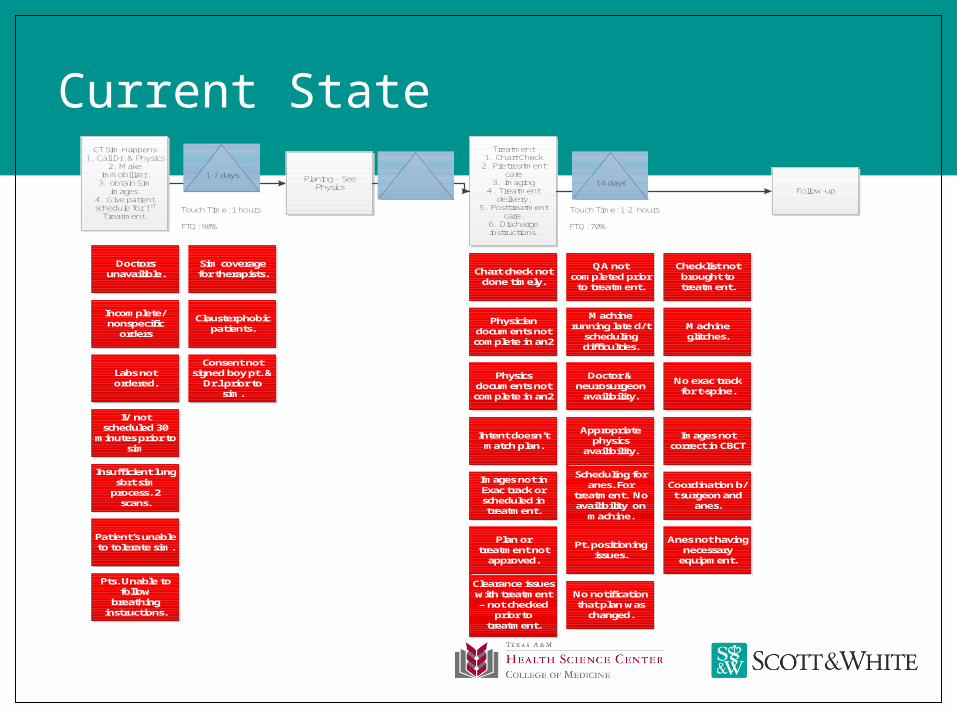
Current StateCT Sim Happens
1. Call Dr. & Physics2. Make
immobilizer.3. obtain Sim
images.4. Give patient schedule for 1st
Treatment.Touch Time: 1 hours
FTQ: 90%
Insufficient lung sbrt sim
process. 2 scans.
IV not scheduled 30
minutes prior to sim
Labs not ordered.
Incomplete/nonspecific
orders
Doctors unavailible.
Clausterphobic patients.
Sim coverage for therapists.
Pts. Unable to follow
breathing instructions.
Patient’s unable to tolerate sim.
Planing – See Physics
Treatment1. Chart Check
2. Pretreatment care
3. Imaging4. Treatment
delivery.5. Posttreatment
care.6. Discharge instructions.
Intent doesn’t match plan.
Physics documents not complete in an2
Physician documents not complete in an2
Chart check not done timely.
QA not completed prior
to treatment.
Clearance issues with treatment – not checked
prior to treatment.
Plan or treatment not
approved.
Images not in Exac track or scheduled in treatment.
Scheduling for anes. For
treatment. No availibility on
machine.
Appropriate physics
availibility.
Doctor & neurosurgeon
availibility.
Machine running late d/t
scheduling difficulties.
No exac track for t-spine.
Machine glitches.
Checklist not brought to treatment.
No notification that plan was
changed.
Pt. positioning issues.
Anes not having necessary
equipment.
Coordination b/t surgeon and
anes.
Images not correct in CBCT
Touch Time: 1-2 hours
FTQ: 70%
Follow-up
1-7 days14 days
Consent not signed boy pt. &
Dr.l prior to sim.
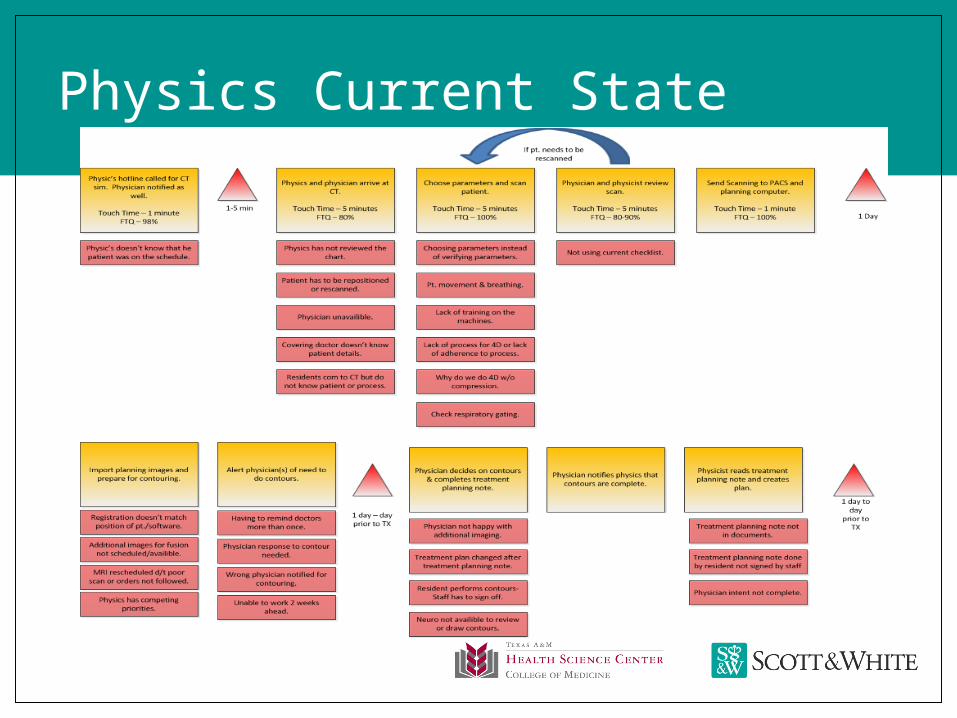
Physics Current State
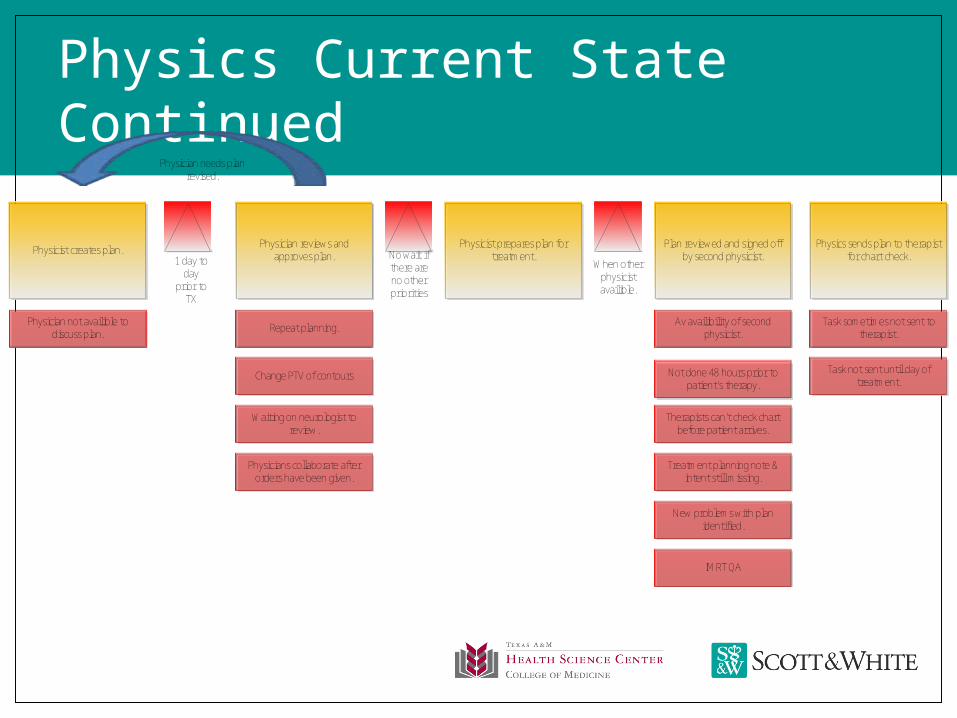
Physics Current State Continued
Physicist creates plan. Plan reviewed and signed off by second physicist.
Physician reviews and approves plan.
Physicist prepares plan for treatment.
Physics sends plan to therapist for chart check.
Physician not availible to discuss plan. Repeat planning.
Waiting on neurologist to review.
1 day to day
prior to TX
No wait if there are no other priorities
Physician needs plan revised.
Change PTV of contours Not done 48 hours prior to patient’s therapy.
Therapists can’t check chart before patient arrives.
Av availibility of second physicist.
Physicians collaborate after orders have been given.
Treatment planning note & intent still missing.
New problems with plan identified.
IMRT QA
Task not sent until day of treatment.
Task sometimes not sent to therapist.
When other physicist availible.
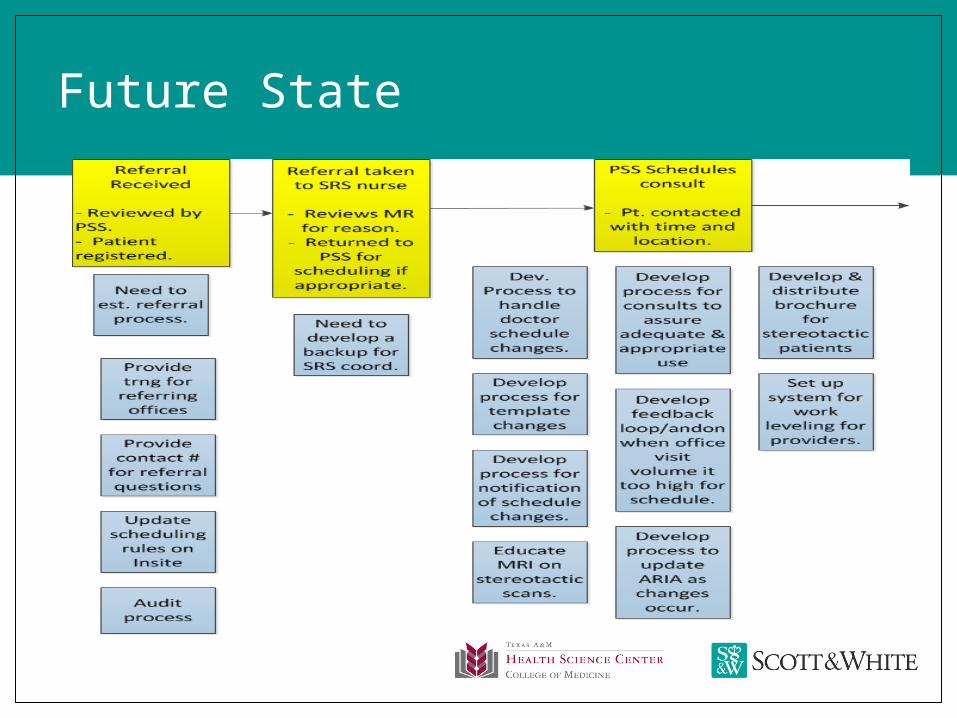
Future State
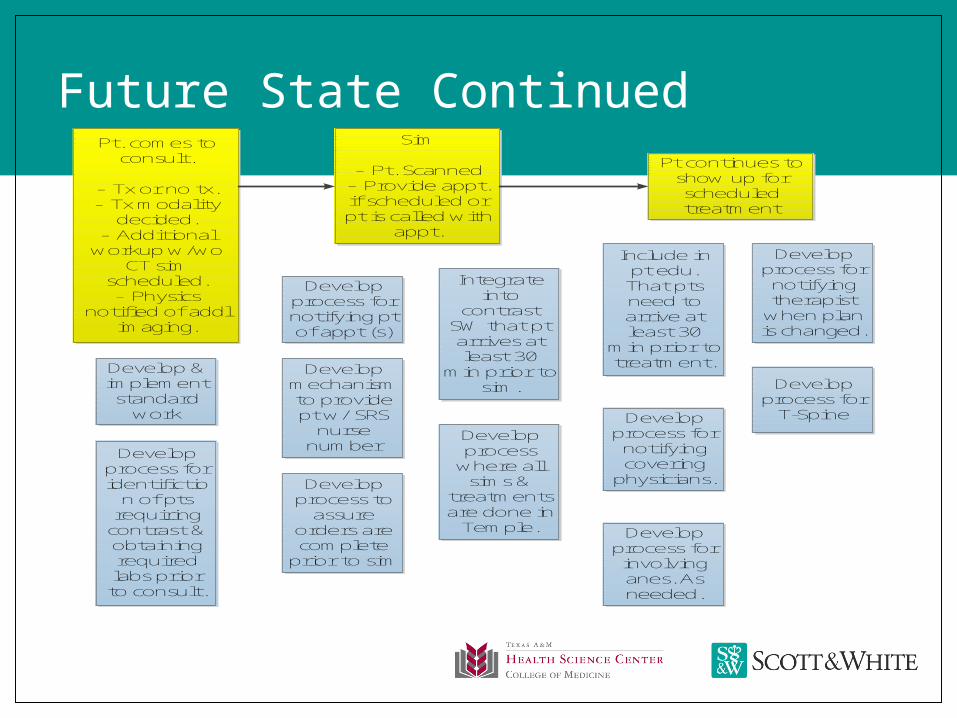
Future State ContinuedPt continues to
show up for scheduled treatment
Sim
- Pt. Scanned- Provide appt. if scheduled or pt is called with
appt.
Pt. comes to consult.
- Tx or no tx.- Tx modality
decided.- Additional
workup w/wo CT sim
scheduled.- Physics
notified of addl imaging.
Develop process for identifictio
n of pts requiring
contrast & obtaining required labs prior
to consult.
Develop & implement standard
work
Develop process
where all sims &
treatments are done in
Temple.
Integrate into
contrast SW that pt arrives at least 30
min prior to sim.
Develop process to
assure orders are complete
prior to sim
Develop mechanism to provide pt w/ SRS
nurse number
Develop process for notifying pt of appt (s)
Develop process for involving anes. As needed.
Develop process for
notifying covering
physicians.
Include in pt edu. That pts need to arrive at least 30
min prior to treatment.
Develop process for
T-Spine
Develop process for
notifying therapist
when plan is changed.
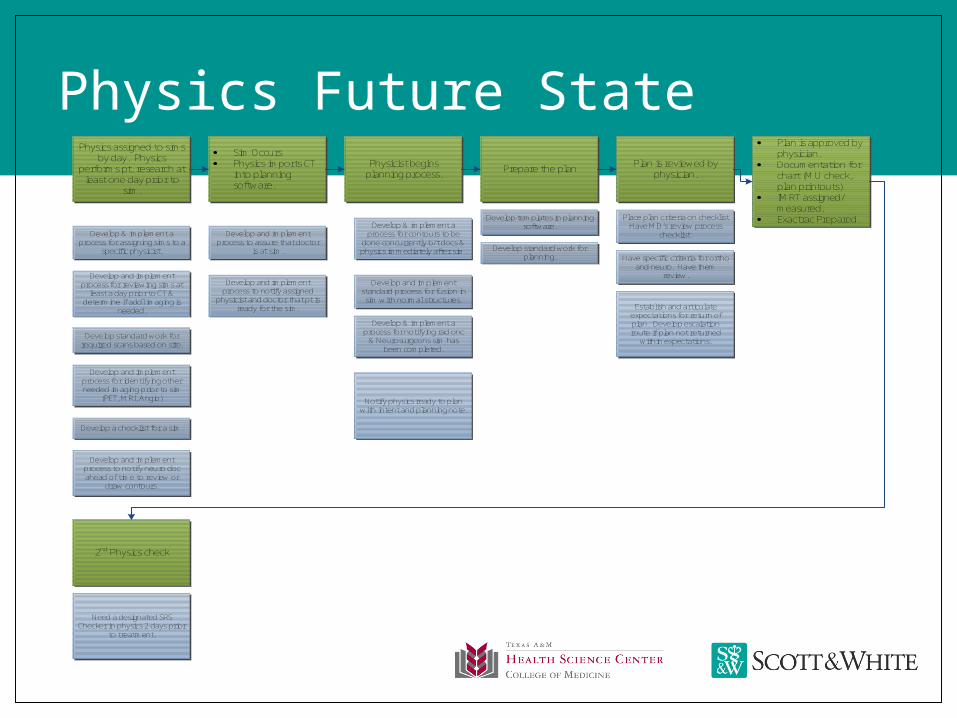
Physics Future State
2nd Physics check
Physicist begins planning process.
· Sim Occurs· Physics imports CT
into planning software.
Physics assigned to sims by day. Physics
performs pt. research at least one day prior to
sim.
Develop & implement a process for assigning sims to a
specific physicist.
Develop and implement process for reviewing sims at
least a day prior to CT & determine if addl imaging is
needed.
Develop & implement a process for contours to be
done concurrently b/t docs & physics immediately after sim.
Develop and implement process to notify assigned
physicist and doctor that pt is ready for the sim.
Develop and implement process to assure that doctor
is at sim.
Develop and implement process to notify neuro doc ahead of time to review or
draw contours.
Develop a checklist for a sim.
Develop and implement process for identifying other needed imaging prior to sim
(PET, MRI, Angio)
Develop standard work for required scans based on site.
Develop standard work for planning.
Develop templates in planning software.
Notify physics ready to plan with intent and planning note.
Develop & implement a process for notifying rad onc
& Neurosurgeons sim has been completed.
Develop and implement standard process for fusion in sim with normal structures.
· Plan is approved by physician.
· Documentation for chart (MU check, plan printouts)
· IMRT assigned/measured.
· Exactrac Prepared.
Plan is reviewed by physician.Prepare the plan
Need a designated SRS Checker in physics 2 days prior
to treatment.
Establish and articulate expectations for return of plan. Develop escalation route if plan not returned
within expectations.
Have specific criteria for ortho and neuro. Have them
review.
Place plan criteria on checklist Have MD’s review process
checklist.
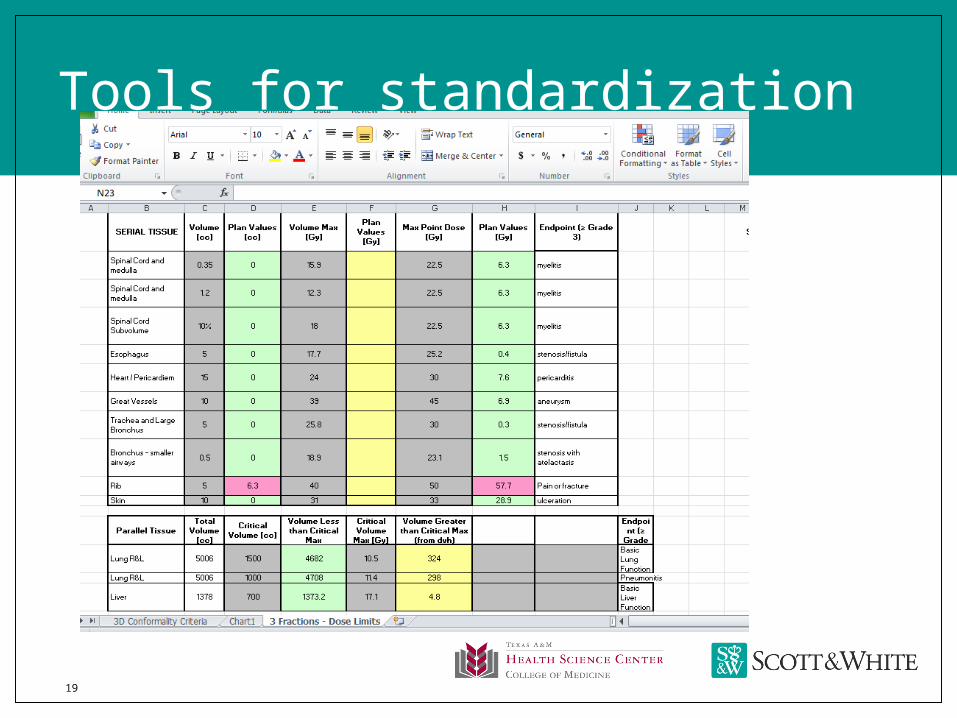
Tools for standardization
19
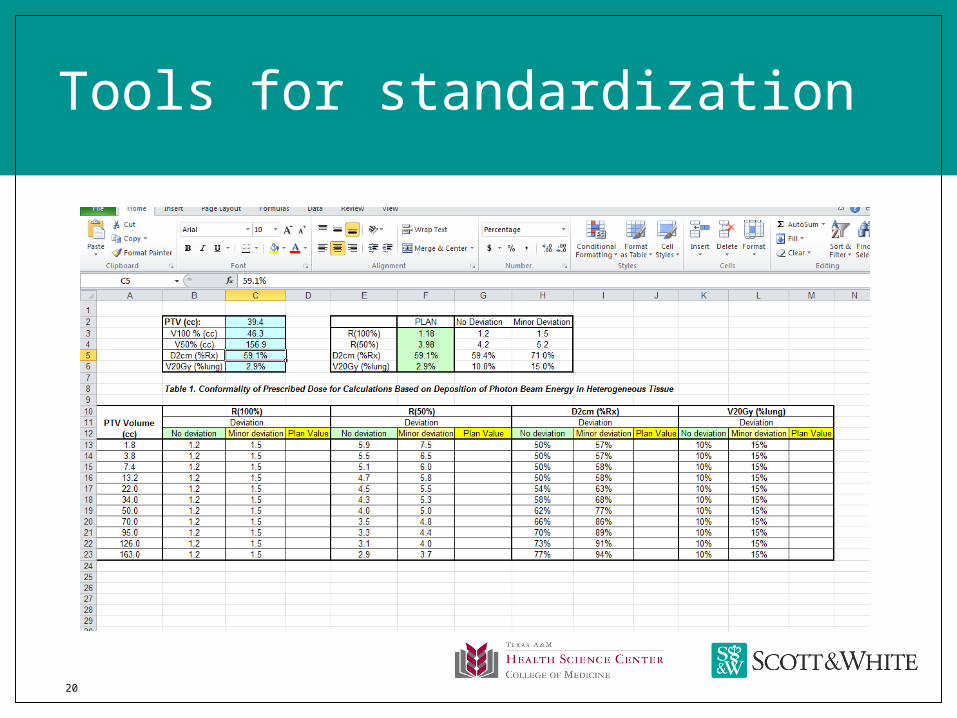
Tools for standardization
20

Checklists
21
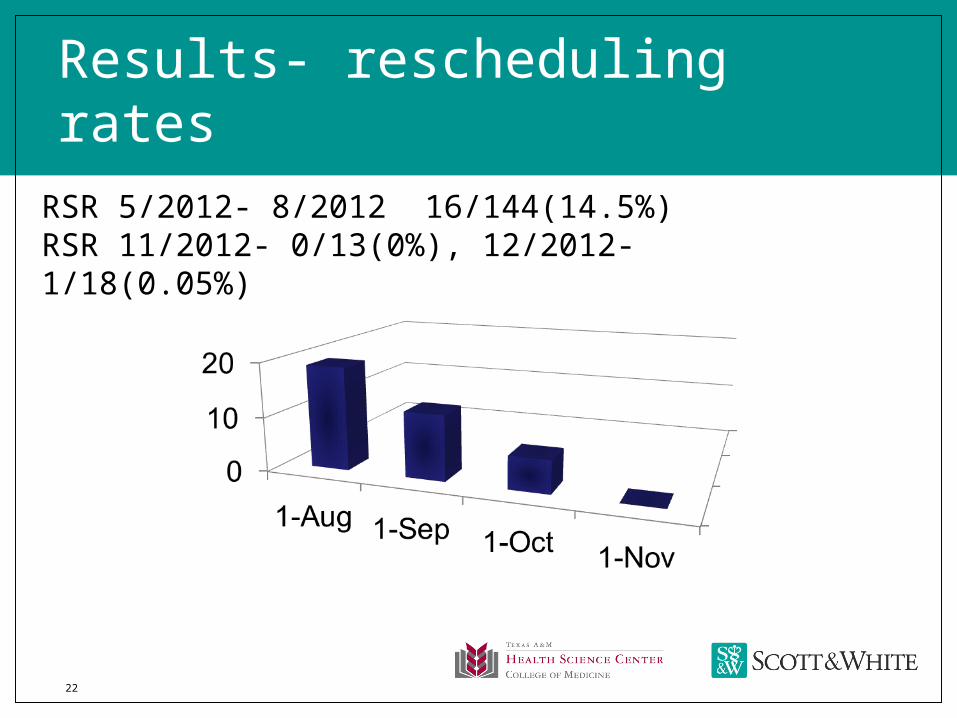
Results- rescheduling rates
22
RSR 5/2012- 8/2012 16/144(14.5%)RSR 11/2012- 0/13(0%), 12/2012- 1/18(0.05%)
23
Results
Treatment start time (check in time- start)
8/2012- 31 minutes( mean 27 min)
10/2012- 9 min( mean 3 min)
Number of steps in the physics process decreased from 15 to 7
24
Discussion
Lean thinking application in the manufacturing sector has been very successful and reproducible
We realized that our current system of operation was a fragmented process
During this process of self discovery, we developed various tools to improve quality and standardize the process
Biggest advantage- Eliminated the usual state where a quickfix/ workaround developed with each problem.
Once a solution obtained- gets incorporated into the process and does not need rework

25
Limitations- No before and after
We improved while going through the process but difficult to obtain parameters to prove the success
26
Conclusions
Using Lean production principles, we improved our stereotactic radiosurgery process and decreased rescheduling of patients
This improvement ( WE THINK!!!) has led to improved safety, quality, patient satisfaction and outcomes
27
Future Directions
Continuous reassessment and improvement
Incorporate new technologies
Institute the process for new sites
28
Acknowledgements
Entire Radiosurgery team-
Front Desk- Courtney, Jessica
Therapists- Ayeisha, Arlene, Jeni, Jessica,
Nursing- Gabby
Physics- Chris Cherry, Sangroh Kim, Andrew Morrow
Department Support- Dr. Mutyala, Dr. Deb, Dr. Rangaraj
Radiosurgery physicians- Dr. Maraboyina, Dr. Patel
CLIP team
especially Gretchen Davenport
29
Questions???
Recommended