Upper extremity deep vein thrombosismanagement in a district general hospitalBabu Pusuluri, Shiva Sreenivasan
Gloucestershire Hospitals NHS Foundation Trust, Gloucester, United Kingdom [email protected]
Recent UK guidance on venous thromboembolic disease1 is notably silent
on upper extremity deep vein thrombosis (UEDVT) management, despite its
high incidence (10% of all cases of DVT)2. Available guidance3 recommends
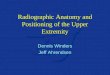
catheter-directed thrombolysis (CDT) (Figure 1) for patients with acute
extensive UEDVT, good functional status, and low bleeding risk, followed by
anticoagulation for 3 months. First rib resection is currently not routinely
recommended. With increasing use of CDT in UEDVT, we reviewed the
demographics and management of patients diagnosed with UEDVT at our
hospital over the past 5 years.
Cases of UEDVT were retrospectively identified over a 5–year period from
archived radiological imaging, as well as from admission records from our
Ambulatory Day Unit and Vascular Imaging Laboratory.
54 cases were identified, of which records for 4 were unavailable. 30 cases
(60%) were men. The majority of cases (70%) were provoked by central venous
catheter (CVC)/pacemaker insertion or malignancy. The rest were either
unprovoked or effort-related (Paget–Schrötter disease). 8 cases (16%) were
referred to vascular surgery for consideration of CDT, which was performed
successfully in 5 patients. 1 patient had first rib resection, and 1 patient had
cervical band excision. Anticoagulation treatment was only documented in 6
cases, and duration varied from 3 months to lifelong.
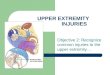
Treatment of UEDVT locally is currently haphazard and has no clear protocol
for either referral for CDT or for anticoagulation duration. We propose a
streamlined multidisciplinary pathway (Figure 2) which can be instigated
in our Ambulatory Day Unit, and which will hopefully optimise care of
patients with UEDVT. This will need subsequent audit to ascertain uptake and
compliance.
References
1. NationalClinicalGuidelineCentre(UK).VenousThromboembolicDiseases:TheManagementofVenousThromboembolicDiseasesandtheRoleofThrombophiliaTesting[Internet].London:RoyalCollegeofPhysicians(UK);2012Jun.(NICEClinicalGuidelines,No.144.)Availablefrom:http://www.ncbi.nlm.nih.gov/books/NBK132796/
2. JoffeHV,KucherN,TapsonVF,et. al.Upper-extremitydeepveinthrombosis:aprospectiveregistryof592patients.Circulation2004;110:1605–1611.
3. KearonC,AklEA,ComerotaAJ,et. al.AntithrombotictherapyforVTEdisease:antithrombotictherapyandpreventionofthrombosis,9thedition:AmericanCollegeofChestPhysiciansEvidence-BasedClinicalPracticeGuidelines.Chest2012;141:e419S–e494S.
4. EngelbergerRP,KucherN.Managementofdeepveinthrombosisoftheupperextremity.Circulation2012;126:768–773.
Introduction
Method
Results
Conclusions
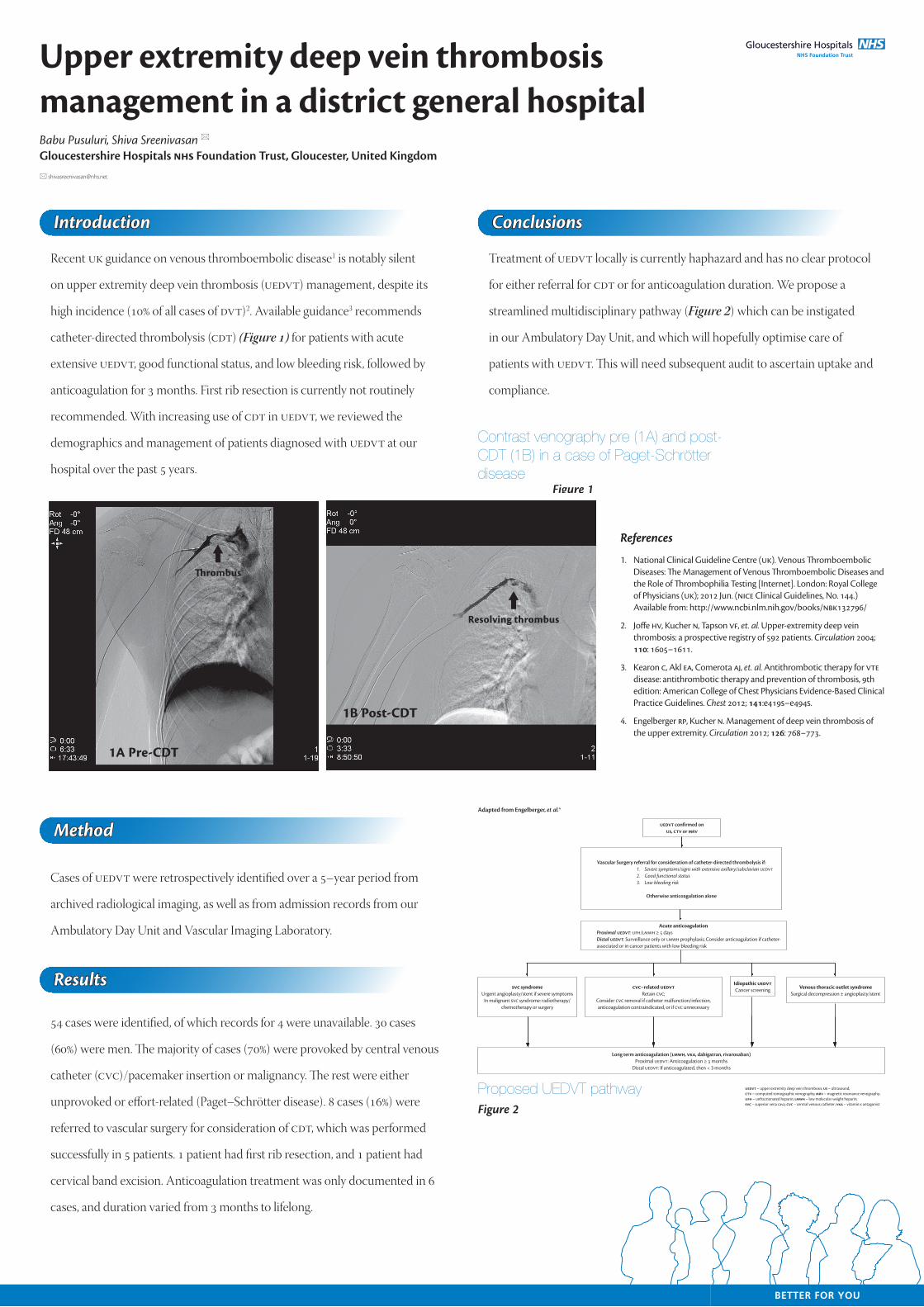
Contrast venography pre (1A) and post-CDT (1B) in a case of Paget-Schrötter disease
Figure 1
1A Pre-CDT
1B Post-CDT
�rombus
Resolving thrombus
Figure 2Proposed UEDVT pathway
Acute anticoagulationProximal UEDVT:UFH/LMWH≥5daysDistal UEDVT:SurveillanceonlyorLMWHprophylaxis;Consideranticoagulationifcatheter-associatedorincancerpatientswithlowbleedingrisk
UEDVT confirmed on US, CTV or MRV
Vascular Surgery referral for consideration of catheter-directed thrombolysis if:1. Severe symptoms/signs with extensive axillary/subclavian UEDVT2. Good functional status3. Low bleeding risk
Otherwise anticoagulation alone
SVC syndromeUrgentangioplasty/stentifseveresymptoms
InmalignantSVCsyndrome:radiotherapy/chemotherapyorsurgery
Idiopathic UEDVTCancerscreening Venous thoracic outlet syndrome
Surgicaldecompression±angioplasty/stentCVC–related UEDVT
RetainCVC;ConsiderCVCremovalifcathetermalfunction/infection,anticoagulationcontraindicated,orifCVCunnecessary
Long term anticoagulation (LMWH, VKA, dabigatran, rivaroxaban)ProximalUEDVT:Anticoagulation≥3months
DistalUEDVT:Ifanticoagulated,then<3months
UEDVT–upperextremitydeepveinthrombosis;US–ultrasound;CTV–computedtomographicvenography;MRV–magneticresonancevenography;UFH–unfractionatedheparin;LMWH–lowmolecularweightheparin;SVC–superiorvenacava;CVC–centralvenouscatheter;VKA–vitaminKantagonist
Adapted from Engelberger, et al.4
Recommended