Update on Hepatitis C virus
infection
24th Annual Southwestern
Conference on Medicine
April 2015
Ester C. Little, MD, FACP
Banner University Medical Center
Phoenix Campus

Disclosures:
Advisory board for Gilead
Speaker for Abbvie

Hepatitis C Virus :
• Structure of the virus
• Historical facts
• Prevalence
• Diagnosis
• Clinical manifestations
• Natural history
• Treatment

Nucleic Acid: 9.6 kb ssRNA
Classification: Flaviviridae, Hepacivirus
Genotypes: 1 to 9
Enveloped
In vitro model: primary hepatocyte and T cell cultures; replicon system
In vivo replication: in cytoplasm, hepatocyte and lymphocyte; human and other primates
40-60 nm
Hepatitis C Virus
Hepatitis C Virus: Morphology and Characteristics

Hepatitis C Virus
5’ UTR 3’ UTR
C E1 E2 NS2 NS3
NS4A
NS4B NS5A NS5B
C E1 E2 NS2 NS3 A NS4 NS5A NS5BB
P7
Core
Envelope
Protease
Serine protease
Protease Cofactor
RNA polymerase
Structural protein coding region
Nonstructural protein coding region
Serine ProteaseHost signal peptidase
Helicase
Genome and Gene Products
Hepatitis C Virus: Genome and Gene Products, pt.5

HCV historical facts:• 1970-80’s a chronic type of hepatitis associated
with transfusion was recognized
• 1989 the HCV virus was identified
• 1990 blood banks start screening but tests were not perfected until 1992
• 1991 FDA approved first Interferon alpha
• 1998 FDA approved Interferon plus Ribavirin
• 2001 FDA approved Pegylated Interferon
• 2011 FDA approved first direct anti viral agent for HCV

Prevalence
HCV - Epidemiology
United States
Anti-HCV positive 3.9 million (1.8%)
HCV RNA positive 2.7 million (1.4%)
Worldwide 170 million ( 3%)
Alter MJ et al., New Engl J Med 1999; 341:556
Lavanchy D & McMahon B, In: Liang TJ & Hoofnagle JH (eds.)
Hepatitis C. New York: Academic Press, 2000:185
Prevalence

HCV - Epidemiology
Heintges, T., Hepatology 1997; 26:521
10 to 205 to 102 to 51 to 20 to 1
HCV Ab pos (%)
Worldwide Prevalence
Worldwide Prevalence


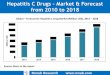
By 2007 hepatitis C-associated deaths had overtaken HIV as a cause of mortality in the United States. To achieve declines in mortality similar to those seen with HIV will require new policy directions and commitment to detect and link infected persons to care and successful treatment.
Mortality Rates of HBV, HCV and HIV: 1999-20071
Morbidity and MortalityPredictions2
DCC, decompensated cirrhosis1. Adapted from Ly KN et al. Ann Intern Med. 2012;156:271-278. 2. Adapted from Rein DB et al. Dig Liver Dis. 2011;43:66-72.
United States: Increased Morbidity and Mortality Due to
HCV Now and in the Future


Holmberg SD et al. New Engl J Med. 2013;368:1859-1861.
Most Americans With Chronic HCV Have Not Been Diagnosed
and Few Have Been Treated
• Limited response to treatment with Interferon• Severe side effect profile• Multiple contra indications

HCV - Epidemiology
Risk Factorsfor Hepatitis C Injection
Drug Use
Multiple
Sexual Partners
Clotting Factor
Treatment Prior
to 1987Long-Term
Hemodialysis
Blood
Transfusion
or Organ Transplant
Prior to 1992
Birth from
Infected Mother
Mass Injections
and Traditional
Practices
Risk Factors for Hepatitis C



Baby boomers
Who should be tested for
hepatitis C
Test for HCVantibody
Riskfactors for HCV
ElevatedALT
Extra-hepatic

HCV Antibody
test
If positive,
test HCV RNA
HCVRNA negative=
False positive or past
infection
HCV RNA positive =
current HCV infection
If negative
No HCV infection
Diagnostic Tests for HCV

Diagnostic Tests
• Hepatitis C antibody test: screening
• Qualitative HCV RNA test: confirmatory
• Quantitative HCV RNA test: monitor treatment
• Genotype: how to treat and for how long
• Liver biopsy: when to treat*
HCV - Diagnosis
Diagnostic Tests

Hoofnagle JH, Hepatology 1997; 26:15S
HCV - Diagnosis
Acute HCV Infection
Time After Exposure
0
400
600
800
1000
ALT(IU/L)
0 2 4 6 8 10 12 24 1 2 3 4 5 6
Anti-HCV
Symptoms
Weeks Months
HCV RNA positive
200
7
Normal
ALT
Acute hepatitis C infection

Acute hepatitis C• Signs and symptoms:
• Asymptomatic ( 79% of cases)
• Anorexia, right upper quadrant abdominal pain, with or without jaundice, arthralgia, myalgia, fatigue, weight loss, skin rash and fever.
• Laboratory tests: • CMP: increased AST, ALT up to thousands, mild
increase in ALK phosphatase and GGT, variable increase in bilirubin, decreased albumin
• Coagulation: prolonged prothrombin time in severe cases.
• Natural history: 55 to 85% of the patients will progress to chronic HCV

Chronic hepatitis C
• Signs and symptoms:• Asymptomatic
• Fatigue, join pain, dull right upper quadrant abdominal pain, anorexia, nausea, pruritus, memory loss
• Laboratory tests:• 1/3 of patients have normal ALT/AST.
• Mildly increased AST/ALT ( 50-low hundreds), with typical fluctuation over time.
• Increased PT and bilirubin, low albumin is seen as the disease progresses to cirrhosis.
• Natural history:• Remain as chronic hepatitis
• Progress to cirrhosis and liver failure
• Patients may develop liver cancer.

Extra hepatic DisordersAssociated with Chronic HCV
Hematological Essential mixed cryoglobulinemia
Non-Hodgkin’s lymphoma
Renal Membranoproliferative glomerulonephritis
Membranous nephropathy
Dermatological Porphyria cutanea tarda
Leukocytoclastic vasculitis
Lichen planus
Autoimmune Diabetes mellitus *
Idiopathic thrombocytopenic purpura
Gumber SC and Chopra S., Ann Intern Med 1995;126
Cacoub P, et al., Medicine 2000; 79:47
Extrahepatic Disorders Associated with Chronic HCV

Photo

Skin Lesion in PCT

HCV - Natural History
Outcome Following Hepatitis C InfectionAcute hepatitis C
Chronic infection
Chronic hepatitis
Cirrhosis
Time(yr)
55 - 85%
70%
20%
10 20 30
Decompensation
HCC1 - 4%/yr
4 - 5%/yr
Outcome Following Hepatitis C Infection

Stages of Fibrosis In Chronic
Hepatitis
HCV - Natural History
Portal Periportal
Septal Cirrhosis
1 2
3 4
Stages of Fibrosis In Chronic Hepatitis

HCV - Diagnosis
Liver biopsy or image modalities
• Degree of fibrosis is most important
predictor of prognosis
• Useful in determining need for
anti-viral therapy
• Advanced cirrhosis is associated with
reduced response to treatment
Liver biopsy in chronic hepatitis C

Liver Biopsy
X
X
X
X

HCV - Natural History
Poynard T, et al., Lancet 1997; 349:825
Duration of infection
Alcohol > 50 gm per day
Age > 40 years at infection
Male gender
Factors Associated With Fibrosis
Factors Associated With Fibrosis

HCV - Diagnosis
HCV Genotypes• Six major genotypes found throughout the
world ( 1 to 6).
• In Europe and U.S., 60-70% of patients
have genotype 1 infection, followed by
genotypes 2 and 3.
• Treatment is different for G 1 and G 2 and 3.
Genotype in hepatitis C

HCV - Treatment
Goals of Hepatitis C Treatment
Goals of Hepatitis C
Treatment Primary
Eradicate the virus
Secondary
Prevent progression to cirrhosis
Reduce incidence of HCC
Reduce need for transplantation
Enhance survival

HCV - Natural History
Outcome Following Hepatitis C InfectionAcute hepatitis C
Chronic infection
Chronic hepatitis
Cirrhosis
Time(yr)
55 - 85%
70%
20%
10 20 30
Decompensation
HCC1 - 4%/yr
4 - 5%/yr
Outcome Following Hepatitis C Infection

HCV - Treatment
Patterns of response to treatment in hepatitis C
HCV RNANegative
SustainedResponder
Nonresponder
Baseline Treatment
Time
HCV RNA
Relapser
Patterns of Response to Hepatitis C
Treatment


Current HCV therapy Genotype 1:
• Sofosbuvir and Ledipasvir for 12 weeks or 24 weeks if patients is treatment experienced with cirrhosis.
• Sofosbuvir and Simeprevir combination for 12 weeks if treatment naïve, for 24 weeks if treatment experienced
• Ombitasvir/Paritaprevir/Ritonavir without Ribavirin for Genotype 1b and with Ribavirin for Genotype 1a. Treat for 12 weeks if treatment naïve and 24 if treatment experienced

HCV therapy for Genotypes 2 and 3:
• Sofosbuvir and Ribavirin for 12 weeks (Genotype 2)
• Sofosbuvir and Ribavirin for 24 weeks (Genotype 3)

HCV treatment special
populations:
• HIV co-infected patients (pts) can be treated with similar response rate
• Pts with GFR no less than 30 can be treated safely
• Post liver and post kidney transplant pts can be treated with excellent response rate
• On going trials for treatment of pts on dialysis
• DAA awaiting FDA approval for pts on dialysis

Current HCV therapy:
• Response rate is similar regardless of genotype
• Response rate is similar regardless of the presence of cirrhosis
• Response rate is similar in different ethnic groups
• Overall response rates are 70 to 90 %
• Interferon free regimens are well tolerated with mild adverse effects (headache, nausea, diarrhea and anemia)
•

Resources for DDIs
• AASLD treatment guidelines with regular updates
• Outstanding – University of Liverpool (David Back, Editorial Board, EASL reps); sponsored by Janssen, MSD, Roche, Vertex:– http://www.hep-druginteractions.org
• FDA:– http://www.fda.gov/Drugs/DrugSafety/
• Other Online Resources –– http://www.drugs.com/drug-interactions/html
– http://www.merckmedicus.com/pp/us/hep
– Epocrates
– Micromedex, Lexicomp and Others

What is in the pipeline?
• Even more effective direct anti-viral agents
• Shorter duration of therapy
• Therapy for pts on HD

HCV summary• HCV infection is common and can be silent
• In addition to the classic risk factors all baby boomers MUST be tested
• Normal AST and ALT does not exclude HCV
• Untreated HCV may progress to cirrhosis and HCC
• Treatment is no simpler, better tolerated and shorter duration
• Response to therapy is seen in 70 to 90% of the treated patients

Thank you!
Recommended