September 2021
2021-MLR-070

SAFE HARBOR STATEMENT
This presentation contains forward looking statements including, but not limited to, statements concerning the outcome or success ofDBV’s clinical trials; its ability to successfully gain regulatory approvals and commercialize products; its ability to successfully advanceits pipeline of product candidates; the rate and degree of market acceptance of its products; and its ability to develop sales andmarketing capabilities. Forward looking statements are subject to a number of risks, uncertainties and assumptions. Moreover, DBVoperates in a very competitive and rapidly changing environment. New risks emerge from time to time. It is not possible for DBV’smanagement to predict all risks, nor can DBV assess the impact of all factors on its business or the extent to which any factor, orcombination of factors, may cause actual results to differ materially from those contained in any forward looking statements it maymake. In light of these risks, uncertainties and assumptions, the forward looking events and circumstances discussed in thispresentation may not occur and actual results could differ materially and adversely from those anticipated or implied in the forwardlooking statements. You should not rely upon forward looking statements as predictions of future events. Although DBV believes thatthe expectations reflected in the forward looking statements are reasonable, it cannot guarantee that the future results, levels ofactivity, performance or events and circumstances reflected in the forward looking statements will be achieved or occur. Moreover,except as required by law, neither DBV nor any other person assumes responsibility for the accuracy and completeness of the forwardlooking statements. Forward looking statements in this presentation represent DBV’s views only as of the date of this presentation.DBV undertakes no obligation to update or review any forward looking statement, whether as a result of new information, futuredevelopments or otherwise, except as required by law.
2

DBV IS A GLOBAL, CLINICAL-STAGE BIOPHARMACEUTICAL COMPANY
We are dedicated to improving the lives of patients with food allergies and other immunological diseases
Our science-driven leadership team has deep regulatory and commercial experience
We have a dedicated team of ~100 professionals, with locations in the United States and France
DBV shares are traded on Euronext Paris (DBV) and Nasdaq (DBVT)
DBV's approach to allergy research is based on epicutaneous immunotherapy
3

• Downregulation of pro-inflammatory cells
• Suppression of Th2 and other allergen-specific effector T cells
• Suppression of inflammatory DCs• Induction of tolerogenic DCs
• Decrease in allergen-specific IgE• Induction of IgG4
Th2
DC
Mast cell
B cell
Eosinophils
Basophils
4
Antigen Presenting Cells capture allergen and induce unique Regulatory T Cells
Regulatory T Cells act on the immune system to alter allergic response
EPIT delivers allergen to intact skin
Epidermis
Dermis
Allergen
Regulatory T Cells
Antigen Presenting
Cell
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.DC=dendritic cell; IgE=immunoglobulin E; IgG4=immunoglobulin G4; Th2=T-helper 2 cell.1. Mondoulet L, et al. J Allergy Clin Immunol. 2015;135:1546-57. 2. Mondoulet L, et al. Allergy. 2019;74:152-164. 3. Moingeon P, Mascarell L. Sem Immunol. 2017;30:52-60. 4. Feuille E, Nowak-Wegrzyn A. Allergy Asthma Immunol Res. 2018;10:189-206. 5. Tordesillas L, et al. Immunity. 2017;47(1):32-50. 6. Dioszeghy V, et al. Cell Mol Immunol. 2017;14:770-782.
EPICUTANEOUS IMMUNOTHERAPY (EPIT™) AIMS TO RE-EDUCATE THE IMMUNE SYSTEM BY INDUCING SPECIFIC REGULATORY T CELLS1-6

THE VIASKIN™ PATCH, OUR NOVEL APPROACH TO EPIT, USES MINIMAL AMOUNTS OF ANTIGEN TO INDUCE AN IMMUNE RESPONSE1-4
The condensation chamber enables natural epidermal water loss to solubilize dry antigen deposited on the patch using an innovative electrospray technology
Solubilized antigen is captured by skin dendriticcells (eg, Langerhans cells) in the epidermis
Langerhans cells process the antigen, migrate to the lymph nodes and present its epitopes to the lymphocytes, leading to a specific immune response
Antigen delivered via Viaskin is not detected in the bloodstream in animal models
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.1. Dioszeghy V, et al. J Immunol. 2011;186:5629-5637. 2. Mondoulet L, et al. Immunotherapy. 2015;7:1293-1305. 3. Mondoulet L, et al. Clin Transl Allergy. 2012;2:22. 4. Fleischer DM, et al. Allergy Asthma Proc.2020; 41(5):326-335. 5
Water loss and
solubilization
Condensation chamber
Langerhans cells

VIASKIN™ HAS MULTIPLE POTENTIAL APPLICATIONS IN FOOD ALLERGIES AND IN OTHER IMMUNOLOGICAL CONDITIONS
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority. 6
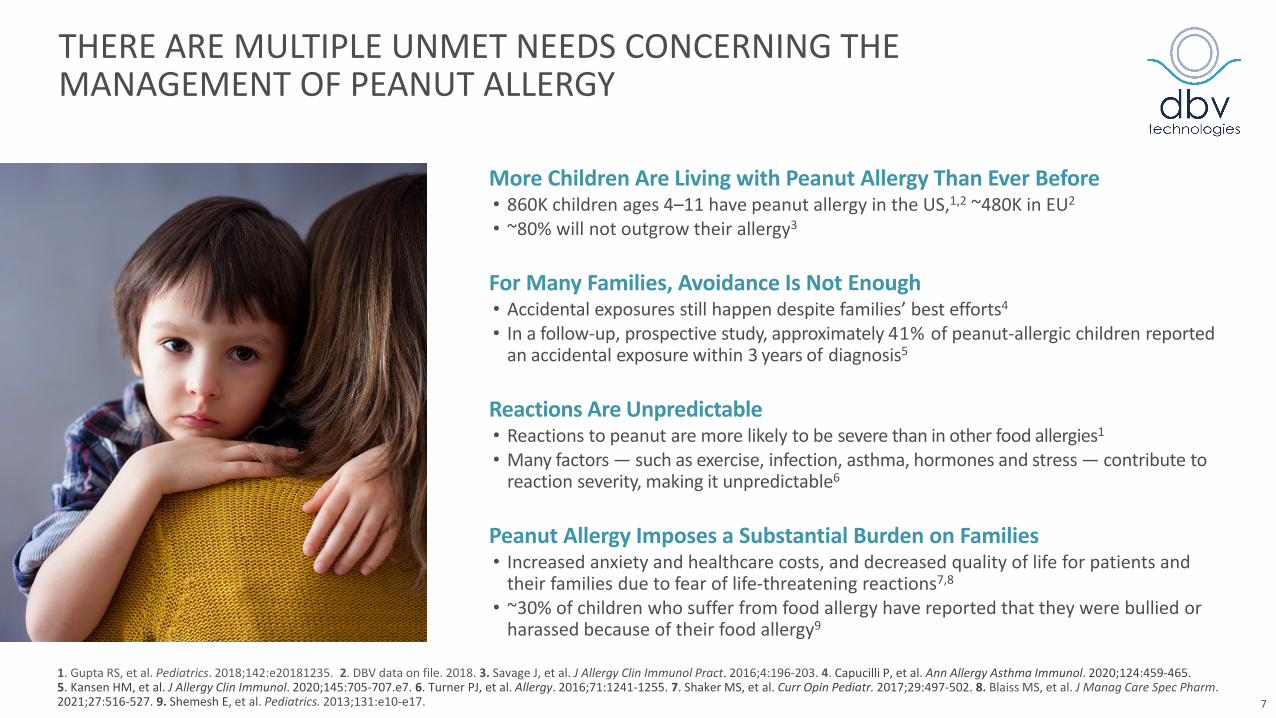
THERE ARE MULTIPLE UNMET NEEDS CONCERNING THE MANAGEMENT OF PEANUT ALLERGY
Reactions Are Unpredictable• Reactions to peanut are more likely to be severe than in other food allergies1
• Many factors — such as exercise, infection, asthma, hormones and stress — contribute to reaction severity, making it unpredictable6
For Many Families, Avoidance Is Not Enough • Accidental exposures still happen despite families’ best efforts4
• In a follow-up, prospective study, approximately 41% of peanut-allergic children reported an accidental exposure within 3 years of diagnosis5
Peanut Allergy Imposes a Substantial Burden on Families• Increased anxiety and healthcare costs, and decreased quality of life for patients and
their families due to fear of life-threatening reactions7,8
• ~30% of children who suffer from food allergy have reported that they were bullied or harassed because of their food allergy9
More Children Are Living with Peanut Allergy Than Ever Before• 860K children ages 4–11 have peanut allergy in the US,1,2 ~480K in EU2
• ~80% will not outgrow their allergy3
1. Gupta RS, et al. Pediatrics. 2018;142:e20181235. 2. DBV data on file. 2018. 3. Savage J, et al. J Allergy Clin Immunol Pract. 2016;4:196-203. 4. Capucilli P, et al. Ann Allergy Asthma Immunol. 2020;124:459-465. 5. Kansen HM, et al. J Allergy Clin Immunol. 2020;145:705-707.e7. 6. Turner PJ, et al. Allergy. 2016;71:1241-1255. 7. Shaker MS, et al. Curr Opin Pediatr. 2017;29:497-502. 8. Blaiss MS, et al. J Manag Care Spec Pharm. 2021;27:516-527. 9. Shemesh E, et al. Pediatrics. 2013;131:e10-e17. 7
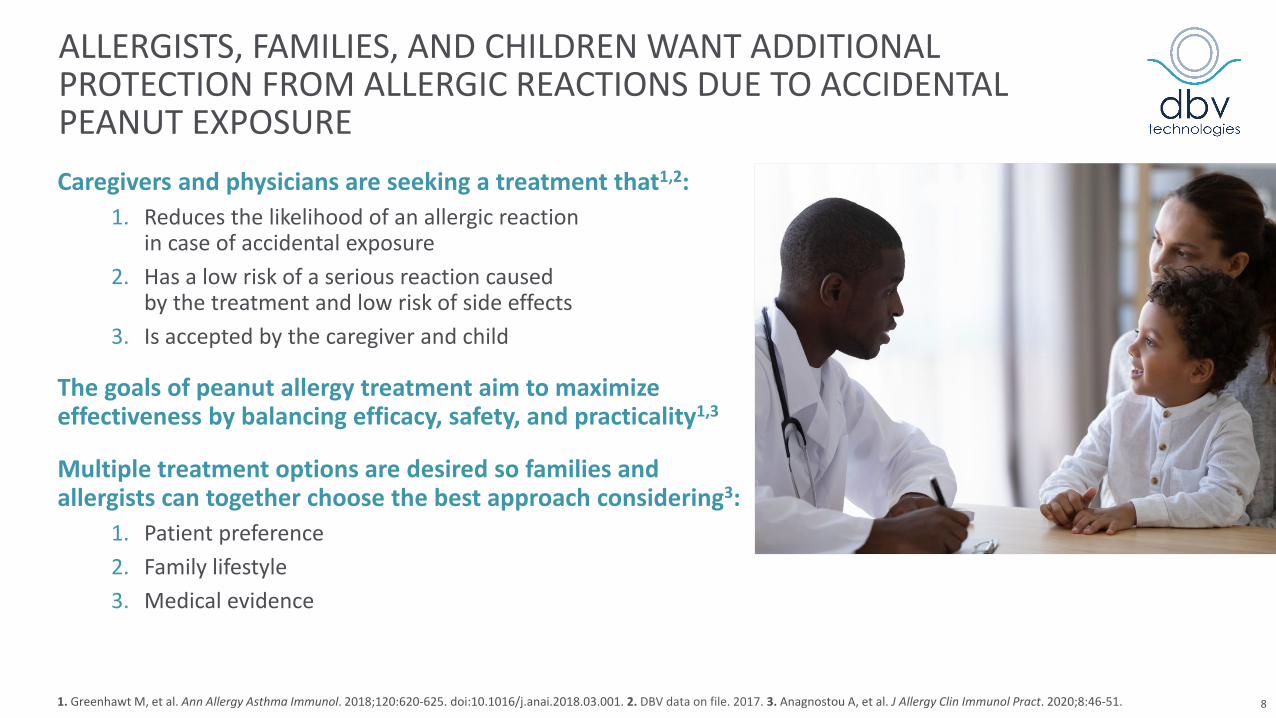
ALLERGISTS, FAMILIES, AND CHILDREN WANT ADDITIONAL PROTECTION FROM ALLERGIC REACTIONS DUE TO ACCIDENTAL PEANUT EXPOSURECaregivers and physicians are seeking a treatment that1,2:
1. Reduces the likelihood of an allergic reaction in case of accidental exposure
2. Has a low risk of a serious reaction caused by the treatment and low risk of side effects
3. Is accepted by the caregiver and child
The goals of peanut allergy treatment aim to maximize effectiveness by balancing efficacy, safety, and practicality1,3
Multiple treatment options are desired so families and allergists can together choose the best approach considering3:
1. Patient preference2. Family lifestyle3. Medical evidence
1. Greenhawt M, et al. Ann Allergy Asthma Immunol. 2018;120:620-625. doi:10.1016/j.anai.2018.03.001. 2. DBV data on file. 2017. 3. Anagnostou A, et al. J Allergy Clin Immunol Pract. 2020;8:46-51. 8
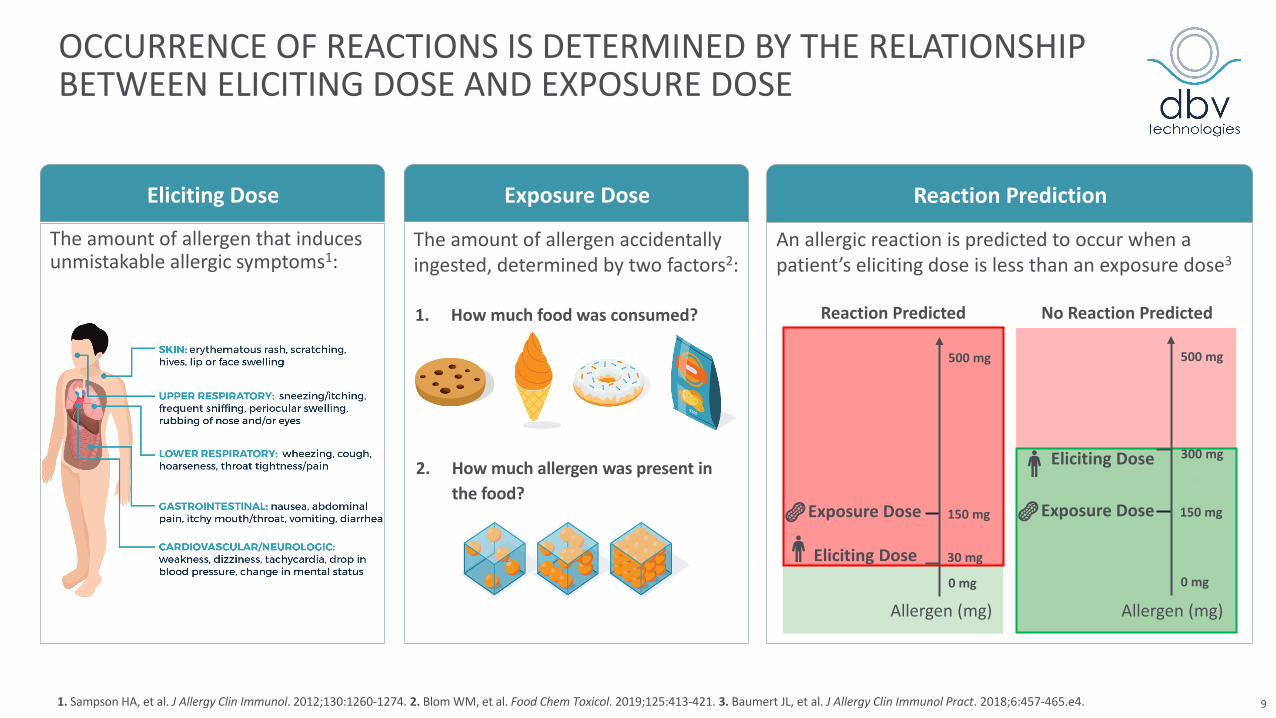
OCCURRENCE OF REACTIONS IS DETERMINED BY THE RELATIONSHIP BETWEEN ELICITING DOSE AND EXPOSURE DOSE
The amount of allergen that induces unmistakable allergic symptoms1:
1. How much food was consumed?
2. How much allergen was present in the food?
The amount of allergen accidentally ingested, determined by two factors2:
1. Sampson HA, et al. J Allergy Clin Immunol. 2012;130:1260-1274. 2. Blom WM, et al. Food Chem Toxicol. 2019;125:413-421. 3. Baumert JL, et al. J Allergy Clin Immunol Pract. 2018;6:457-465.e4. 9
Eliciting Dose Exposure Dose
An allergic reaction is predicted to occur when a patient’s eliciting dose is less than an exposure dose3
Reaction Prediction
Allergen (mg)
Reaction Predicted
0 mg
500 mg
150 mg
30 mgEliciting Dose
Exposure Dose
No Reaction Predicted
0 mg
300 mg
500 mg
Allergen (mg)
150 mgExposure Dose
Eliciting Dose

MODELING* DATA SUGGEST INCREASING A PATIENT’S ELICITING DOSE DECREASES THE RISK OF AN ALLERGIC REACTION1
*The Quantitative Risk Analysis model inputs variables including the clinical threshold for peanut-allergic individuals and the exposure dose of peanut residue to predict the allergenic risk associated with the exposure to residual peanut protein. ED=eliciting dose.1. Baumert JL, et al. J Allergy Clin Immunol Pract. 2018;6:457-465. 10
Decrease in Reaction Risk Following Allergen Immunotherapy
ED before allergen immunotherapy 1 mg
10 mg
30 mg
300 mgED after allergen immunotherapy
Increasing a patient’s eliciting dose from 1, 10, or 30 mg to 300 mg or100 or 300 mg to 1,000 mg
via allergen immunotherapy is predicted to reduce their risk of an allergic reaction by >99%
ED before allergen immunotherapy
300 mg
ED after allergen immunotherapy
100 mg
1,000 mg
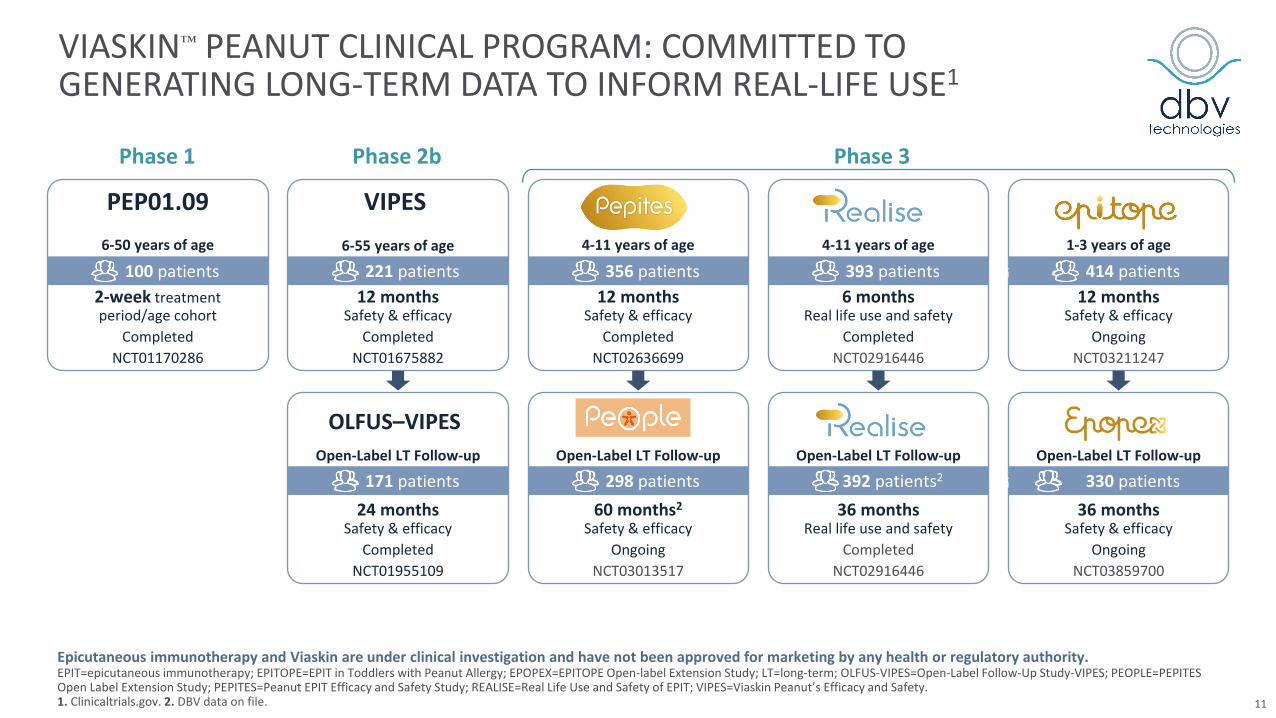
VIASKIN™ PEANUT CLINICAL PROGRAM: COMMITTED TO GENERATING LONG-TERM DATA TO INFORM REAL-LIFE USE1
Phase 1 Phase 2b
36 months Real life use and safety
CompletedNCT02916446
Open-Label LT Follow-up
392 patients2
24 months Safety & efficacy
CompletedNCT01955109
Open-Label LT Follow-up
171 patients
OLFUS–VIPES
60 months2
Safety & efficacyOngoing
NCT03013517
Open-Label LT Follow-up
298 patients36 months
Safety & efficacyOngoing
NCT03859700
Open-Label LT Follow-up
330 patients
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.EPIT=epicutaneous immunotherapy; EPITOPE=EPIT in Toddlers with Peanut Allergy; EPOPEX=EPITOPE Open-label Extension Study; LT=long-term; OLFUS-VIPES=Open-Label Follow-Up Study-VIPES; PEOPLE=PEPITES Open Label Extension Study; PEPITES=Peanut EPIT Efficacy and Safety Study; REALISE=Real Life Use and Safety of EPIT; VIPES=Viaskin Peanut’s Efficacy and Safety. 1. Clinicaltrials.gov. 2. DBV data on file.
2-week treatment period/age cohort
CompletedNCT01170286
PEP01.09
100 patients6-50 years of age
12 months Safety & efficacy
CompletedNCT01675882
VIPES6-55 years of age
221 patients12 months
Safety & efficacyCompleted
NCT02636699
4-11 years of age
356 patients6 months
Real life use and safetyCompleted
NCT02916446
4-11 years of age
393 patients12 months
Safety & efficacyOngoing
NCT03211247
1-3 years of age
414 patients
Phase 3
11

EFFICACY DATA OF VIASKIN™ PEANUT IN CHILDREN AGES 4–11 YEARS
Pivotal Phase 3 Study (PEPITES)1 Open-label Follow-on Study (PEOPLE)2
12
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*The prespecified 15% lower bound of the 95% CI of the difference between treatment groups was not met (95% CI: 12.4, 29.8). The clinical relevance of this in food allergy is unknown.1
†Based on ITT population; missing data calculated using mBOCF. DBPCFC=double-blind, placebo-controlled food challenge; ED=eliciting dose.1. Fleischer DM, et al. JAMA. 2019;321:946-955. 2. Fleischer DM, et al. J Allergy Clin Immunol. 2020;146:863-874. 3. DunnGalvin A et al. J Allergy Clin Immunol Pract. 2021;9:216-224.e1.
After 12 months, a significantly larger percentage of participants responded to Viaskin Peanut treatment vs placebo patch (35.3% vs 13.6% [P<0.001])*
75.9% of subjects demonstrated an increase in ED from baseline to Month 36
51.8% of subjects reached an ED of ≥1,000 mg at Month 36, compared to 40.4% at Month 12
Patients in the Viaskin Peanut treatment arm were 4x more likely to experience an increase in eliciting dose than patients in the placebo arm
13.5% of subjects were able to tolerate the full DBPCFC of 5,444 mg (~18 peanuts) at Month 36
Food Allergy Quality of Life (QoL) Assessment in PEPITES, PEOPLE3
• Based on validated food allergy QoL questionnaires, children experienced statistically significant QoL improvements after 2 years of Viaskin Peanut treatment

VIASKIN™ PEANUT SAFETY INFORMATION FROMCLINICAL TRIALS TO DATE1,2
Most Common AEs In PEPITES (Months 0–12) and PEOPLE (Months 12–36),
the most commonly reported treatment-related AEs were local application site reactions, which were mostly mild to moderate in severity
– Local application site reactions decreased in frequency and severity over time
Adherence and Discontinuation Rates A mean compliance of 98% was observed over 3 years of
treatment TEAEs leading to permanent discontinuation occurred in:
– 1.7% of patients treated with Viaskin Peanut vs 0% with placebo from Months 0–12
– 2% of patients treated with Viaskin Peanut from Months 12–36
Treatment-related Anaphylaxis* and Epinephrine Use 8 (3.4%) Viaskin Peanut participants experienced
10 events of treatment-related anaphylaxis* in 12 months of treatment
– All were graded as mild or moderate, and 6 of the 10 events were treated with injectable epinephrine
No treatment-related epinephrine use was observed in the PEOPLE study (Months 12–36)
– 1 patient experienced 1 possibly related mild anaphylaxis that resolved without treatment
13
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*Anaphylaxis was defined according to NIAID, which has been shown to be highly sensitive but moderately specific, in an attempt to capture as many reactions as possible. Severe anaphylaxis was defined by the presence of cyanosis, hypoxia, hypotension, confusion, loss of consciousness, or incontinence. AE=adverse event; TEAE=treatment-emergent adverse event.1. Fleischer DM, et al. JAMA. 2019;321:946-955. 2. Fleischer DM, et al. J Allergy Clin Immunol. 2020;146:863-874.

IF APPROVED, VIASKIN PEANUT MAY OFFER A CONVENIENT, EASY-TO-USE TREATMENT FOR PATIENTS AND THEIR FAMILIES
Viaskin Peanut is designed to have the following features:
Applied at home, once a day
No treatment escalation, minimizing number of extra doctor's appointments
No activity limitations
No restriction on activities such as exercise or hot bath/shower
No oral peanut ingestion required
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority. 14

WE ARE PURSUING POTENTIAL APPROVAL OF VIASKIN™
PEANUT IN CHILDREN AGES 4–11 IN THE UNITED STATES
Complete Response Letter (CRL) received in August 2020. FDA identified the following concerns1:– Impact of patch-site adhesion on efficacy– Need for patch modifications and supplementary clinical data to support a modified patch– Need for Human Factors study with modified patch – Additional Chemistry, Manufacturing and Controls (CMC) data requested – FDA did not raise any safety concerns related to Viaskin Peanut
FDA feedback received in January 2021 provided a well-defined regulatory path forward for Viaskin Peanut2
– A modified Viaskin Peanut patch (mVP) should not be considered a new product entity provided the occlusion chamber and the peanut protein dose of the current Viaskin Peanut patch (cVP) remain unchanged and perform in the same way
– FDA requested an assessment comparing the uptake of allergen (peanut protein) between cVP and mVP– FDA recommended a 6-month, well-controlled safety and adhesion trial to assess mVP in children ages 4-11– FDA did not require a trial with mVP that includes an efficacy measure such as a double-blind placebo-controlled
food challenge
15
Epicutaneous immunotherapy and Viaskin Peanut are under clinical investigation and have not been approved for marketing by any health or regulatory authority.FDA=US Food and Drug Administration.1. DBV Technologies. Press Release. August 4, 2020. Accessed July 13, 2021. https://www.dbv-technologies.com/wp-content/uploads/2020/08/dbv-technologies-receives-complete-response-letter-from-fda-for-viaskin-peanut-bla-.pdf. 2. DBV Technologies. Press Release. January 14, 2021. Accessed July 13, 2021. https://www.dbv-technologies.com/wp-content/uploads/2021/01/dbv-press-release-fda-feedback_01.14.2021_final_english.pdf.
VIASKIN PEANUTUS

SIGNIFICANT PROGRESS MADE IN DEVELOPING MODIFIED PATCHES AND MVP CLINICAL STUDY EFFORTS
16
VIASKIN PEANUTUS
Identify potential modifications
Produce modified patch prototypes
In vitro, in vivo testing
Initiate manufacturing modifications
Select 5 mVPs to advance to CHAMP
mVP Clinical Development PlanPatch Modification
5 mVP Candidates
CHAMP: Modified patch study (5 mVPs, 1 cVP) in healthy adult volunteers Two mVPs selected for further development
STAMP: 6-month safety, adhesion study in children ages 4–11 with peanut allergy Protocol submitted to FDA for review
PREQUAL: EQUAL methodology and assay validation study in healthy adult volunteers Study initiated
EQUAL: Allergen uptake equivalence study Ongoing exchanges with FDA
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.CHAMP=Comparison of adHesion Among Modified Patches; cVP=current Viaskin Peanut; EQUAL=EQuivalence in Uptake of ALlergen; FDA=Food and Drug Administration; mVP=modified Viaskin Peanut; STAMP=Safety, Tolerability, and Adhesion of Modified Patches.

Pre-submission Validation Clock Stop*
Primary Evaluation
Secondary Evaluation
Clock Stop*
Final Evaluation
CHMPOpinion
EMA REVIEW OF VIASKIN™ PEANUT MAA PROCEEDING ACCORDING TO STANDARD EVALUATION TIMELINE1
Day 0 Day 1
4Q 2020
Day 120
1Q 2021
Day 121
Day 181
Day 210
Day 277
4Q21 – 1Q22
Day 180
3Q 2021
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*During a 'clock stop' the evaluation is paused while the applicant prepares the responses to the CHMP’s questions and issues.CHMP=Committee for Medicinal Products for Human Use; EMA=European Medicines Agency; MAA=Marketing Authorization Application.1. European Medicines Agency. Updated October 2, 2020. Accessed June 29, 2021. https://www.ema.europa.eu/en/human-regulatory/marketing-authorisation/evaluation-medicines-step-step. 17
VIASKIN PEANUT EU

0
5
10
15
20
1Q20 2Q20 3Q20 4Q20 1Q21 2Q21
CONTINUED FINANCIAL DILIGENCE MAINTAINS OPERATING LATITUDE TO PROGRESS VIASKIN™ PEANUT
Cash balance of $125.5 million at end of 2Q 2021
Cash and cash equivalents to support business operations until 2H 2022
Global cost reduction program initiated in 1H 2020 and completed in 1H 2021, resulting in leaner organization and greater operating latitude
Net cash flow used in operating activities* in 2Q 2021 decreased by 42% compared to Q1 2020
Average Monthly Cash Used in Operations$, millions
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*Excluding restructuring costs. 18
3Q 2021 Financial Results
EMA Review Continues
EQUAL, STAMP Protocol Finalization
UPCOMING CATALYSTS
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.
October 2021
2H 2021
2H 2021
19

DBV CONTACTS
Investor RelationsAnne Pollak+1 [email protected]
Public Relations and MediaAngela Marcucci+1 [email protected]
Partnering and Licensing [email protected]
Clinical Trial [email protected]
Medical Information +1 855-DBV-TECH (US and Canada)www.dbv-technologies.com/contact-us/medical-form/
20

APPENDIX: CLINICAL TRIAL DATA FOR VIASKIN PEANUT

KEY PUBLICATIONS
Dioszeghy V, Mondoulet L, Dhelft V, et al. Epicutaneous immunotherapy results in rapid allergen uptake by dendritic cells through intact skin and downregulates the allergen-specific response in sensitized mice. J Immunol. 2011;186(10):5629-5637.
Mondoulet L, Dioszeghy V, Puteaux E, et al. Intact skin and not stripped skin is crucial for the safety and efficacy of peanut epicutaneous immunotherapy (EPIT) in mice. Clin Transl Allergy. 2012;2(1):22.
Mondoulet L, Dioszeghy V, Thébault C, Benhamou PH, Dupont C. Epicutaneous immunotherapy for food allergy as a novel pathway for oral tolerance induction. Immunotherapy. 2015;7(12):1293-1305.
Sampson HA, Shreffler WG, Yang WH, et al. Effect of Varying Doses of Epicutaneous Immunotherapy vs Placebo on Reaction to Peanut Protein Exposure Among Patients With Peanut Sensitivity: A Randomized Clinical Trial. JAMA. 2017;318(18):1798-1809.
Remington BC, Krone T, Koppelman SJ. Quantitative risk reduction through peanut immunotherapy: Safety benefits of an increased threshold in Europe. Pediatr Allergy Immunol. 2018;29(7):762-772.
Baumert JL, Taylor SL, Koppelman SJ. Quantitative Assessment of the Safety Benefits Associated with Increasing Clinical Peanut Thresholds Through Immunotherapy. J Allergy Clin Immunol Pract. 2018;6(2):457-465.e4.
Fleischer DM, Greenhawt M, Sussman G, et al. Effect of Epicutaneous Immunotherapy vs Placebo on Reaction to Peanut Protein Ingestion Among Children With Peanut Allergy: The PEPITES Randomized Clinical Trial. JAMA. 2019;321(10):946-955.
Fleischer DM, Shreffler WG, Campbell DE, et al. Long-term, open-label extension study of the efficacy and safety of epicutaneous immunotherapy for peanut allergy in children: PEOPLE 3-year results. J Allergy Clin Immunol. 2020;146(4):863-874.
Fleischer DM, Chinthrajah S, Scurlock AM, et al. An evaluation of factors influencing response to epicutaneous immunotherapy for peanut allergy in the PEPITES trial. Allergy Asthma Proc. 2020;41(5):326-335.
22

PEPITES AND ITS 5-YEAR, OPEN-LABEL EXTENSION, PEOPLE, IS THE LONGEST-TERM PEANUT IMMUNOTHERAPY TRIAL
M0
Placebo (n=118)
VP 250 µg (n=238)
n=100
n=198
PEPITES (Viaskin™ Peanut 250 µg vs Placebo)1 PEOPLE (Viaskin Peanut 250 µg)2
Efficacy Endpoints• Treatment responder definition (assessed using DBPCFC)
– M0 ED ≤10 mg: responder if ED ≥300 mg at M12– M0 ED >10 mg: responder if ED ≥1,000 mg at M12
• Key secondary endpoints– Changes in ED, CRD, peanut sIgE and sIgG4
Efficacy Measurements• Percentage of patients reaching an ED ≥1,000 mg after 24
months of additional treatment with VP 250 µg• Changes in ED, CRD, peanut sIgE and sIgG4• Sustained unresponsiveness† at month 38 after 2 months
without treatment
356 patients• 4–11 years old• Confirmed peanut allergy*
n=107
n=213
DBPCFC
M12 M24Rollover to VP 250 µg
184 148
91 83
M12
M36 M48 M60
M24 M36 M38 M60
M38
M48
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.CRD=cumulative reactive dose; DBPCFC=double-blind, placebo-controlled food challenge; ED=eliciting dose; PEOPLE=PEPITES Open-Label Extension Study; PEPITES=Peanut EPIT™ Efficacy and Safety Study;sIgE=specific immunoglobulin E; sIgG4= specific immunoglobulin G4; VP=Viaskin Peanut. *Peanut allergy confirmed by specific immunoglobulin E (slgE) levels >0.7 kUA/L and skin prick test (SPT) results ( ≥6 mm for 4- to 5-year-olds or ≥8 mm for 6- to-11-year-olds).†Sustained unresponsiveness defined as no objective symptoms to ≥1000 mg ED during the M38 DBPCFC. Participants who reached an ED ≥1000 mg at Month 36 in PEOPLE were eligible, but not required, to continue for 2 additional months without treatment and were required to maintain a peanut-free diet. 1. Fleischer DM, et al. JAMA. 2019;321:946-955. 2. Fleischer DM, et al. J Allergy Clin Immunol. 2020;146:863-874. 23

VIASKIN™ PEANUT TREATMENT EFFECT AFTER 12 MONTHS1
Placebon=118
Viaskin Peanut 250 µgn=238
Response Rate After 12 Months*
33.9%
6.7%
38.1%
30.7%
28.0%
62.6%
0%
20%
40%
60%
80%
100%
Perc
ent o
f Sub
ject
s
Change in Eliciting Dose After 12 Months†
Placebon=118
Viaskin Peanut 250 µgn=238
13.6%
35.3%
0%
10%
20%
30%
40% P<0.001
Δ= 21.7%(95% CI: 12.4, 29.8)
The prespecified 15% lower bound of the 95% CI of the difference between treatment groups was not met.
• The clinical relevance of this is not known1
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*Based on ITT population. Response defined as ED of ≥300 mg at Month 12, if baseline ED was ≤10 mg or ED of ≥1,000 mg at Month 12 if baseline ED was >10 mg. †Based on ITT population; missing data calculated using mBOCF. CI=confidence interval; ED=eliciting dose; ITT=intention to treat; mBOCF=modified baseline observation carried forward.1. Fleischer DM, et al. JAMA. 2019;321:946-955.
ED IncreaseED StableED Decrease
24

CHANGE IN CUMULATIVE REACTIVE DOSE (CRD) AND ELICITING DOSE WITH LONG-TERM VIASKIN™ PEANUT TREATMENT1
223.8
1120.4
1768.8
0
500
1,000
1,500
2,000
2,500
3,000
Baseline Month 12 Month 36
144444
944
Cumulative Reactive Dose (mg)Mean, Median (-)
PEOPLE Per Protocol (N=141)
75.9% of subjects demonstrated an increase in ED from baseline to Month 36
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*Tolerated=passed the double-blind, placebo-controlled food challenge without meeting PRACTALL stopping criteria.1. Fleischer DM, et al. J Allergy Clin Immunol. 2020;146:863-874.
51.8% of subjects reached an ED of ≥1,000 mg at Month 36, compared to 40.4% at Month 12
13.5% of subjects were able to tolerate* the full DBPCFC of 5,444 mg (equivalent to ~18 peanuts) at Month 36
25
144

MOST COMMONLY REPORTED TREATMENT-RELATED ADVERSE EVENTS
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*Immune System Disorders include anaphylactic reactions and non-anaphylactic hypersensitivity reactions.AE=adverse event; TEAE=treatment-emergent adverse event.1. Fleischer DM, et al. JAMA. 2019;321:946-955.
34.7%27.1%
8.5%0.8%
59.7% 57.6%
5.5% 5.0%
0%
20%
40%
60%
80%
100%
Any Treatment-related TEAE Administration Site
Skin and Subcutaneous Tissue Immune System Disorders*
% S
ubje
cts
PEPITES: Treatment-related TEAEs(occurring in ≥5% of subjects in 12 months)1
Viaskin™ Peanut 250 µg, n=238Placebo, n=118
No treatment-related gastrointestinal AEs observed
26

CHANGE IN FREQUENCY AND SEVERITY OF LOCAL ADMINISTRATION SITE REACTIONS AFTER MONTH 1
Local Administration Site Reactions in the Viaskin™ Peanut 250 µg Group Over Time1*
In the extension study period between 12 and 36 months2:
The most commonly reported treatment-related AEs were mild to moderate skin reactions
Treatment-related local administration site reactions were observed in 77.8% (154/198) of patients
Site reactions decreased to 29.9% (55/198) in Year 3 of treatment
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*Includes all administration site reactions irrespective of treatment relatedness.†Reaction definitions: Grade 1: only erythema, or erythema + infiltration; Grade 2: erythema, few papules; Grade 3: erythema, many or spreading papules; Grade 4: erythema, vesicles.1. Fleischer DM, et al. JAMA. 2019;321:946-955. 2. Fleischer DM, et al. J Allergy Clin Immunol. 2020;146:863-874.
0%
20%
40%
60%
80%
100%
% S
ubje
cts
49.2%
72.6%
83.4% 82.3%76.9%
68.2% 67.7%59.2%
Grade 4 Grade 3 Grade 2 Grade 1†
Day 1 Day 8 M1 M3 M6 M9 M12 M12 +1 Week
27

0.8%
2.9%
0%
2%
4%
6%
8%
10%
Placebo (n=118) Viaskin Peanut 250 µg(n=238)
RATES OF TREATMENT-RELATED ANAPHYLAXIS* AND EPINEPHRINE USE1,2
8 (3.4%) Viaskin™ Peanut participants experienced 10 events of treatment-related anaphylaxis* in 12 months of treatment
– All were graded as mild or moderate without evidence of cardiovascular, neurologic, or respiratory compromise
– 6 of 10 events were treated with injectable epinephrine (one dose each)
– None treated with supplemental oxygen– 5 of the 8 participants continued in the study
No treatment-related epinephrine use was observed in the PEOPLE study (Months 12–36)
– 1 patient experienced 1 possibly related mild anaphylaxis that resolved without treatment
Treatment-related TEAEs leading to epinephrine use from M0–M12
% S
ubje
cts
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*Anaphylaxis was defined according to NIAID, which has been shown to be highly sensitive but moderately specific, in an attempt to capture as many reactions as possible. Severe anaphylaxis was defined by the presence of cyanosis, hypoxia, hypotension, confusion, loss of consciousness, or incontinence. M=month; TEAE=treatment-emergent adverse event.1. Fleischer DM, et al. JAMA. 2019;321:946-955. 2. Fleischer DM, et al. J Allergy Clin Immunol. 2020;146:863-874. 28
TREATMENT ADHERENCE AND DISCONTINUATION RATES WITH VIASKIN™ PEANUT OBSERVED OVER 12, 36 MONTHS
98.5% treatment compliance at 12 months, comparable between Viaskin Peanut and placebo groups
A mean compliance of 98% was observed over 3 years of treatment
89.9% of all subjects completed the 12-month study, with similar discontinuation rates observed between treatment groups (10.5% in Viaskin Peanut group, 9.3% in placebo group)
50 patients discontinued* between the start of PEOPLE and Month 36– 27 patients discontinued between Months 30 and 36, with 22 of the 27 identifying food challenge
fright/distaste as the reason for consent withdrawal
TEAEs leading to permanent discontinuation occurred in:– 1.7% of patients treated with Viaskin Peanut vs 0% with placebo from M0–M12– 2% of patients treated with Viaskin Peanut from M12–M36
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*Includes those who discontinued prior to or during the Month 36 double-blind, placebo-controlled food challenge (DBPCFC).M=month; TEAE=treatment-emergent adverse event. 1. Fleischer DM, et al. JAMA. 2019;321:946-955. 2. Fleischer DM, et al. J Allergy Clin Immunol. 2020;146:863-874. 29

CLINICAL RELEVANCE OF INCREASING A PATIENT’S ELICITING DOSE THROUGH ALLERGEN IMMUNOTHERAPY
30ED=eliciting dose.1. Baumert JL, et al. J Allergy Clin Immunol Pract. 2018;6:457-465. 2. Parrish CP. Am J Manag Care. 2018;24(19 Suppl):S419-S427. 3. Deschildre A, et al. Clin Exp Allergy. 2016;46(4):610-20.
Highest risk Lowest risk
Decrease in risk of reaction as a function of increasing eliciting dose1
(example: ice cream) A single peanut kernel contains ~250 to 300 mg of peanut protein2
The median ED for peanut-allergic children is 67.3 mg (<1/3 of a peanut kernel)3
The median amount of peanut protein associated with real-life accidental exposure reactions is 125 mg3
Base
line
ED
(mg
pean
ut p
rote
in)
Post-immunotherapy ED (mg peanut protein)
1 3 10 30 100 300 1000
1 0% 22.7% 46.8% 68.7% 90.4% 99.5% 99.9%
3 0% 31.1% 59.5% 87.6% 99.4% 99.9%
10 0% 41.2% 82.0% 99.1% 99.9%
30 0% 69.5% 98.5% 99.9%
100 0% 94.9% 99.9%
300 0% 98.6%
1000 0%

PREDICTED RISK REDUCTION OF ALLERGIC REACTIONS CAUSED BY PEANUT-CONTAMINATED FOODS WITH VIASKIN™ PEANUT TREATMENT
31Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.1. Remington BC, et al. Ann Allergy Asthma Immunol. 2019;123:488-493.e2. 2. Remington BC, et al. Ann Allergy Asthma Immunol. 2021;126:208-209.
Risk reduction per eating occasion1
Viaskin Peanut 250 µg Placebo
Cookies -77.7% +3.0%
Donuts -76.3% +2.2%
Ice cream -73.2% +0.3%
Salty snacks -78.4% +3.9%
Modeling based on clinical trial data with Viaskin Peanut predicts:
73%–78% reduction in the risk of an allergic reaction following the consumption of prepackaged foods1
86% reduction in the risk of an allergic reaction following the consumption of single-serve meals at restaurants (restaurants cooking peanut sauces and cleaning utensils)2
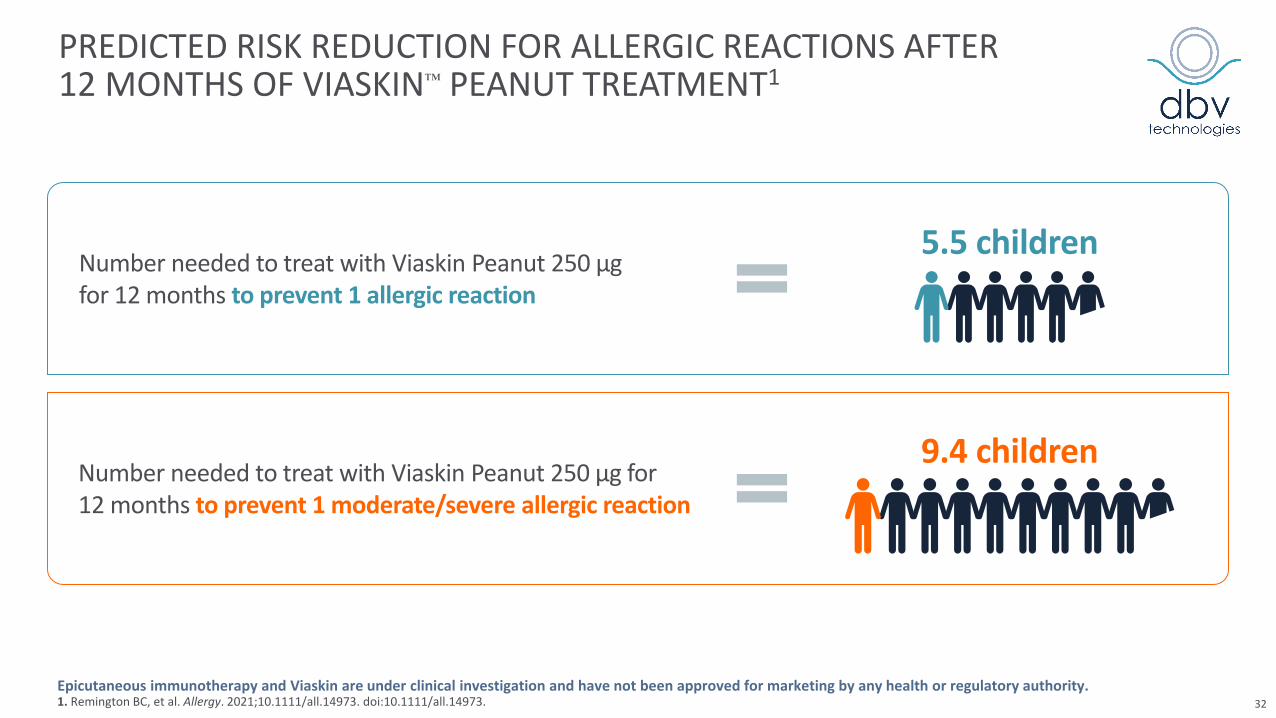
PREDICTED RISK REDUCTION FOR ALLERGIC REACTIONS AFTER 12 MONTHS OF VIASKIN™ PEANUT TREATMENT1
32Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.1. Remington BC, et al. Allergy. 2021;10.1111/all.14973. doi:10.1111/all.14973.
Number needed to treat with Viaskin Peanut 250 µg for 12 months to prevent 1 allergic reaction
5.5 children
Number needed to treat with Viaskin Peanut 250 µg for 12 months to prevent 1 moderate/severe allergic reaction
9.4 children

CHANGE IN CHILDREN’S QUALITY OF LIFE WITH VIASKIN™ PEANUT OBSERVED AT 2 YEARS1
33
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.*A lower score indicates an improved QOL. †FAQLQ parent form: parent-proxy report of child's QoL (all children); child form: self report for children 8 years and older.FAQLQ=Food Allergy Quality of Life Questionnaire. 1. DunnGalvin A et al. J Allergy Clin Immunol Pract. 2021;9:216-224.e1.
-0.26
-0.85
0.08
-0.39
-1.4
-1.2
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4FAQLQ Parent form (proxy)† FAQLQ Child form
LS Mean Change from Baseline to Year 2 in FAQLQ Total Scores*Viaskin Peanut 250 µg during year 1 Placebo during year 1
LS mean difference: -0.34P=0.008
LS mean difference: -0.46P=0.023
N=175
N=89
N=42
N=91

CHANGE IN SEVERITY OF ALLERGIC REACTIONS WITH VIASKIN™ PEANUT TREATMENT1
34
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.DBPCFC=double-blind, placebo-controlled food challenge; M=month. 1. Bégin P, et al. Presented at AAAAI 2021 Virtual Annual Meeting. https://www.dbv-technologies.com/wp-content/uploads/2021/03/aaaai-2021_severity-pepites_poster-v4_29jan21_final.pdf
31.1%16.5%
16.2% 27.5%
0%
20%
40%
60%
80%
100%
Viaskin Peanut(n=222)
Placebo (n=109)
% S
ubje
cts
DBPCFC at M12
P<0.001
Severe Moderate None or mild
Less severe symptoms with Viaskin Peanut 250 µg at the M12 DBPCFC1
Global score and score of organ systems most likely to indicate a life-threatening response
15.8% 11.0%
38.7% 33.0%
0%
20%
40%
60%
80%
100%
Viaskin Peanut(n=222)
Placebo (n=109)
% S
ubje
cts
DBPCFC at baseline
P=0.931
Global Severity Score

EFFICACY AND SAFETY OF VIASKIN™ PEANUT IN PATIENTS WITH CONCOMITANT ALLERGIC DISEASES AT BASELINE
35
Epicutaneous immunotherapy and Viaskin are under clinical investigation and have not been approved for marketing by any health or regulatory authority.AD=atopic dermatitis; CFA=concomitant food allergies; FEV1=forced expiratory volume in 1 second; SCORAD=SCORing Atopic Dermatitis; TEAE=treatment-emergent adverse event. 1. Davis CM, et al. AAAAI 2019 Annual Meeting (Poster 735). 2. Lange L et al. EAACI 2019 congress (Abstract LBPD 1719). 3. Bégin P et al. EAACI 2020 (Abstract 1362).
Efficacy and safety results similar irrespective of the presence of concomitant food allergies
Efficacy and safety results similar irrespective of the presence of concomitant atopic dermatitis
No change in SCORAD in both groups
Concomitant Food Allergies3
at BaselineConcomitant Atopic Dermatitis1
at BaselineConcomitant Asthma2
at Baseline
Efficacy and safety results similar irrespective of the presence of concomitant asthma
No difference in respiratory TEAE between treatment arms
No change in FEV1 in both groups
PlaceboViaskin Peanut
P<0.001 P<0.001
44%
29%
18%
9%
AD No AD
% R
espo
nder
s at
12
Mon
ths
P=0.002 P=0.004
37%34%
13% 14%
Asthma No Asthma
% R
espo
nder
s at
12
Mon
ths
for interactionacross CFA status
P=0.17
33%38%
17%
9%
CFA No CFA
% R
espo
nder
s at
12
Mon
ths
Recommended