
VIDEOS
‘‘Triangle of safety’’: anatomic considerations in transvaginalnatural orifice surgery
Kurt Roberts • Daniel Solomon • Robert Bell •
Andrew Duffy
Received: 12 September 2012 / Accepted: 19 October 2012 / Published online: 4 May 2013
� Springer Science+Business Media New York 2013
Abstract
Background The introduction of transvaginal (TV) natu-
ral orifice transluminal endoscopic surgery (NOTES)
brings the loss of traditionally used cutaneous landmarks
for safe peritoneal access. This video describes the use of
landmarks within the posterior vaginal fornix to define a
‘‘triangle of safety’’ wherein the peritoneal cavity can be
accessed while minimizing the risk of injury to surrounding
structures.
Methods The triangle of safety is best identified in the
following way. The cervix and posterior fornix are visu-
alized. Then an imaginary clock located at the base of the
cervix is envisioned. The superior two corners of the tri-
angle are represented by the 4 and 8 o’clock positions on
this imaginary clock. Sometimes the cervix needs to be
grasped and elevated anteriorly so that the inferior apex of
the triangle delineated by the center of the rectovaginal
fold is better visualized.
Results During hybrid TV NOTES, the rectovaginal
pouch of Douglas is visualized from the umbilicus, and the
vaginal port can then be safely passed through the center of
the triangle. It is important that the vaginal port should be
angled upward, aiming toward the umbilicus to avoid
injury to the rectum. During pure TV NOTES, the incision
is made with electrocautery from the 5 o’clock position to
the 7 o’clock position within the triangle. The peritoneum
is sharply entered, and the colpotomy is dilated with the
surgeons’ fingers.
Conclusions The triangle of safety defines a set of land-
marks between the base of the cervix and the rectovaginal
fold. It allows for a safe TV access for hybrid and pure TV
NOTES while minimizing the risk of injury to surrounding
structures.
Keywords Complications � Natural orifice surgery �NOTES � Transvaginal
Through an open incision, a surgeon achieves both tactile
feedback and depth perception. Traditional surgical lapa-
roscopy minimizes incisions with the corequisite loss of
tactile feedback and depth. This trade-off is taken one step
further with the introduction of transvaginal (TV) natural
orifice transluminal endoscopic surgery (NOTES) because
the loss of percutaneous incisions brings the loss of cuta-
neous landmarks for safe peritoneal access. This video
illustrates the use of landmarks within the posterior vaginal
fornix to define a ‘‘triangle of safety’’ wherein the perito-
neal cavity can be accessed while minimizing the risk of
injury to surrounding structures.
The utilization of anatomic landmarks to safely define
structures and minimize the risk of injury is part and parcel
to minimally invasive surgery. Introduced in 1994, the
‘‘critical view of safety’’ improved the performance of
laparoscopic cholecystectomy by identifying landmarks
within the absence of tactile and 3D cues to identify the
cystic duct and thereby avoid inadvertent injury to the
common bile duct [1]. Similarly, the ominous ‘‘triangle of
doom’’ delineates the anatomic landmarks that should not
be dissected or tacks placed during a totally extraperitoneal
herniography [2]. The triangle of safety is a similar set of
Electronic supplementary material The online version of thisarticle (doi:10.1007/s00464-013-2864-0) contains supplementarymaterial, which is available to authorized users.
K. Roberts (&) � D. Solomon � R. Bell � A. Duffy
Section of Surgical Gastroenterology, Department of Surgery,
Yale University School of Medicine, 40 Temple Street, Suite 7B,
New Haven, CT 06510, USA
e-mail: [email protected]
123
Surg Endosc (2013) 27:2963–2965
DOI 10.1007/s00464-013-2864-0
and Other Interventional Techniques
landmarks through which a colpotomy can be safely made
into the peritoneum for pure TV NOTES or under visual-
ization from an umbilical port for hybrid TV NOTES.
Methods
Patient positioning
As previously described [3], patients are placed in a low
lithotomy position in Allen stirrups after the induction of
general endotracheal anesthesia. The operating surgeon
stands between the patient’s legs while the scrub nurse
assists from behind with the laparoscopic screen positioned
above the patient’s abdomen. In cases of pure TV NOTES,
the assistant joins the operating surgeon at the foot of the
table. In hybrid TV NOTES, the assistant operates the
transumbilical instruments from the patient’s left side. The
abdomen, pelvis, and vaginal canal are disinfected with the
appropriate surgical disinfectant. With the patient placed in
the steep Trendelenburg position, a weighted speculum is
introduced into the vagina, allowing for visualization of the
cervix. The cervix is then grasped with a single-toothed
tenaculum and retracted anteriorly.
Triangle of safety
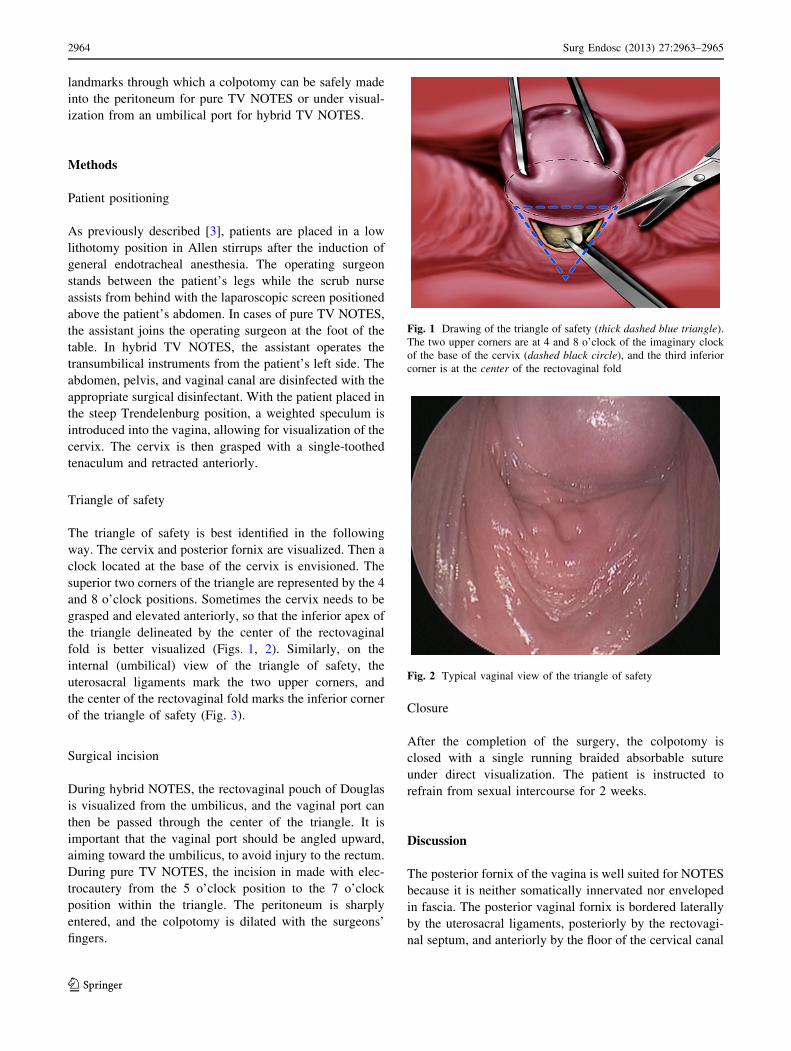
The triangle of safety is best identified in the following
way. The cervix and posterior fornix are visualized. Then a
clock located at the base of the cervix is envisioned. The
superior two corners of the triangle are represented by the 4
and 8 o’clock positions. Sometimes the cervix needs to be
grasped and elevated anteriorly, so that the inferior apex of
the triangle delineated by the center of the rectovaginal
fold is better visualized (Figs. 1, 2). Similarly, on the
internal (umbilical) view of the triangle of safety, the
uterosacral ligaments mark the two upper corners, and
the center of the rectovaginal fold marks the inferior corner
of the triangle of safety (Fig. 3).
Surgical incision
During hybrid NOTES, the rectovaginal pouch of Douglas
is visualized from the umbilicus, and the vaginal port can
then be passed through the center of the triangle. It is
important that the vaginal port should be angled upward,
aiming toward the umbilicus, to avoid injury to the rectum.
During pure TV NOTES, the incision in made with elec-
trocautery from the 5 o’clock position to the 7 o’clock
position within the triangle. The peritoneum is sharply
entered, and the colpotomy is dilated with the surgeons’
fingers.
Closure
After the completion of the surgery, the colpotomy is
closed with a single running braided absorbable suture
under direct visualization. The patient is instructed to
refrain from sexual intercourse for 2 weeks.
Discussion
The posterior fornix of the vagina is well suited for NOTES
because it is neither somatically innervated nor enveloped
in fascia. The posterior vaginal fornix is bordered laterally
by the uterosacral ligaments, posteriorly by the rectovagi-
nal septum, and anteriorly by the floor of the cervical canal
Fig. 1 Drawing of the triangle of safety (thick dashed blue triangle).
The two upper corners are at 4 and 8 o’clock of the imaginary clock
of the base of the cervix (dashed black circle), and the third inferior
corner is at the center of the rectovaginal fold
Fig. 2 Typical vaginal view of the triangle of safety
2964 Surg Endosc (2013) 27:2963–2965
123

[4]. A colpotomy through the triangle of safety minimizes
the risk of injury to the surrounding vital structure,
including the bladder anteriorly, the rectum posteriorly,
and the ureters that travel along the base of the cervix at 3
and 9 o’clock positions of the imaginary clock.
Conclusion
The triangle of safety defines a set of landmarks between
the base of the cervix and the rectovaginal fold that allows
for safe TV access for pure and hybrid TV NOTES while
minimizing the risk of injury to surrounding structures.
Disclosures Dr. Roberts has intellectual property rights and equity
in NovaTract. Drs. Solomon, Bell, and Duffy have no conflicts of
interest or financial ties to disclose.
References
1. Strasberg SM, Hertl M, Soper NJ (1995) An analysis of the
problem of biliary injury during laparoscopic cholecystectomy.
J Am Coll Surg 1:101–125
2. Spaw AT, Ennis BW, Spaw LP (1991) Laparoscopic hernia repair:
the anatomic basis. J Laparoendosc Surg 5:269–277
3. Roberts KE, Solomon D, Mirensky T, Silasi DA, Duffy AJ,
Rutherford T, Longo WE, Bell RL (2012) Pure transvaginal
appendectomy versus traditional laparoscopic appendectomy for
acute appendicitis: a prospective cohort study. Ann Surg 2:266–269
4. Nichols DH, Clynde RL (1989) Vaginal surgery. Williams &
Wilkins, Baltimore
Fig. 3 Umbilical view of port placement within the triangle of safety
(dashed blue triangle)
Surg Endosc (2013) 27:2963–2965 2965
123
Recommended










![Transvaginal Mesh Lawsuits [Data Timeline]](https://img.pdfslide.us/doc/110x75/5884223e1a28ab485c8b5d45/transvaginal-mesh-lawsuits-data-timeline.jpg)





