Treatment of STEMI in 2011:Treatment of STEMI in 2011:Management of PatientsManagement of Patients
Presenting to NonPresenting to Non--PCI CentersPCI Centers
Stephen G. Ellis, M.D.Professor of Medicine
Director Invasive ServicesCo-Director Cardiac Gene Bank

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
How do you tell?How do you tell?
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
Which one?Which one?
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
How highHow highrisk?risk?
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
Who shouldWho shouldget lytics?get lytics?
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
--Less emphasis on difference between DTN Less emphasis on difference between DTN and DTB per seand DTB per seA b l l ti f t ti < 90 iA b l l ti f t ti < 90 i--Ambulance lytics for presentation < 90 minAmbulance lytics for presentation < 90 min
--Otherwise PCI except for high risk, early presentingOtherwise PCI except for high risk, early presentingpts with long DTB delay and low risk of bleedingpts with long DTB delay and low risk of bleeding--Keep decision tree simple (thinkingKeep decision tree simple (thinking-->delays)>delays)p p ( gp p ( g y )y )
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
Which one?Which one?
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

PCI After Lytics/GPIPCI After Lytics/GPIyy
Facilitated PCI/RationaleFacilitated PCI/RationaleFacilitated PCI/RationaleFacilitated PCI/Rationale
•• Early reperfusion salvages myocardiumEarly reperfusion salvages myocardium•• Early reperfusion salvages myocardiumEarly reperfusion salvages myocardium
•• In many areas, door to balloon times exceed In many areas, door to balloon times exceed ACC d d 90 iACC d d 90 iACC recommended <90 minACC recommended <90 min
•• Some combination of antiplatelet + lyticSome combination of antiplatelet + lyticSome combination of antiplatelet lytic Some combination of antiplatelet lytic treatment can open IRA before PCI in many treatment can open IRA before PCI in many casescases
SGE / jd 02_06

ASSENT IV ASSENT IV -- Trial DesignTrial DesignggASSENT IV Study DesignASSENT IV Study Design
STEMI patients < 6 hrs, PCI within 1-3 hrsN=4000
Randomization 1:1, Open Label
UFH (60IU/kg) and Aspirin UFH (70IU/kg) and AspirinUFH (60IU/kg) and Aspirin UFH (70IU/kg) and Aspirin
Clopidogrel only after angiogram when decision for stent implantation is made
Primary PCIIIb/IIIa investigator discretion
Pre-treatment with Full Dose TNK followed by Primary PCI
Primary Endpoint * : Composite of Death or Cardiogenic Shock or Congestive Heart
(clopidogrel if stent)IIb/IIIa bail out only* (clopidogrel if stent)
Failure within 90 Days
* * Used in only 9.6%Used in only 9.6%

Stopped on Basis of Mortality at 30 DaysStopped on Basis of Mortality at 30 Dayspp y ypp y yASSENT IV Preliminary DataASSENT IV Preliminary Data
1010
Mortality (%)Mortality (%)TNK + PCITNK + PCIPCI alonePCI alone
66
88
6
PCI alonePCI alone
P = 0.04P = 0.04
44
66 6
3.8
0
22
50/82850/828 32/83532/83500
6.7 vs 5.0% (p=.14) at 90 days6.7 vs 5.0% (p=.14) at 90 days
Van de Werf ESC 2005
18.8 vs 13.7% (p=.006) MACE at 90 days18.8 vs 13.7% (p=.006) MACE at 90 days

Acute MIAcute MI
Platelet Activation by FibrinolyticsPlatelet Activation by Fibrinolytics
Normalized Maximal Aggregation RateNormalized Maximal Aggregation Ratet-PA
1.51.5
t-PASK
1.01.0
0.50.5
Time (min)Time (min)00 5050 100100 150150 200200 250250
Rudd and Loscalzo, CircRes ‘90Rudd and Loscalzo, CircRes ‘90Rabbit model, .05mM ADP as agonistRabbit model, .05mM ADP as agonistSGE; 0802-3, 22

FINESSE: Study DesignFINESSE: Study Designy gy gAcute ST Elevation MI (or New LBBB*) within 6h pain onsetAcute ST Elevation MI (or New LBBB*) within 6h pain onset
Presenting at Hub or Spoke with estimated time to PCI between 1 and 4 hoursPresenting at Hub or Spoke with estimated time to PCI between 1 and 4 hours
Randomize 1:1:1N=3000 *Only 5U if ≥75
*LocalizedIMI excluded
PlaceboPlacebo
Reteplase (5U+5U)*Abciximab
PlaceboAbciximab
Transfer To Cath LabASA, unfractionated heparin 40U/kg (max 3000u)
or enoxaparin (0 5 mg/kg IV + 0 3 mg/kg SC) – substudy only
Abciximab Placebo Placebo
or enoxaparin (0.5 mg/kg IV + 0.3 mg/kg SC) – substudy only
Primary PCI with Abciximab Infusion (12 h)
Primary endpoint at 90 days: All-cause mortality, resuscitated VFoccurring > 48H, cardiogenic shock, or readmission/ED visit for CHF

All Cause Mortality Through 1 YearAll Cause Mortality Through 1 Yeary gy g
7 0%7.4%
6.3%7.0%

FINESSE: 1 Year Mortality by FINESSE: 1 Year Mortality by Infarct LocationInfarct LocationInfarct LocationInfarct Location
All Cause Mortality Through 1 Year
20%
25%
9.9% 10.0%
15%
rcen
tage p=.093
4.6%
9.9%
4.9% 6.1% 6.5%
5%
10%Per
0%Nonanterior (n=1279) Anterior (n=1173)
Primary PCI with In Lab AbciximabAbciximab Facililated PCIAbciximab/Reteplase Facilitated PCI

HORIZONS: ThreeHORIZONS: Three--Year AllYear All--Cause MortalityCause Mortality
)) 99
1010 Bivalirudin alone (n=1800)Bivalirudin alone (n=1800)Heparin + GPIIb/IIIa (n=1802)Heparin + GPIIb/IIIa (n=1802)
5 9%5 9%
7.7%7.7%al
ity (%
)al
ity (%
) 99
77
88
33--yr HR [95%CI]=yr HR [95%CI]=
5.9%5.9%
se M
orta
se M
orta
44
55
66 4.8%
P=0.03P=0.030.75 [0.58, 0.97]0.75 [0.58, 0.97]
All
All--
Cau
sC
aus
11
22
33
0 71 [0 51 0 98]0 71 [0 51 0 98]11--yr HR [95%CI]=yr HR [95%CI]=
3.4%
AA
00
11
00 1212 1515 1818 2121 2424 2727 3030 3333 363633 66 99
0.71 [0.51, 0.98]0.71 [0.51, 0.98]P=0.04P=0.04
1611161115681568
166016601689168916701670
18001800Bivalirudin aloneBivalirudin alone 1098109818021802 16431643
MonthsMonthsNumber at riskNumber at risk
Heparin+GPIIb/IIIaHeparin+GPIIb/IIIa1633163315931593
1574157415251525 10431043

Impact of PreImpact of Pre--randomization Heparin in randomization Heparin in the HORIZONSthe HORIZONS AMI TrialAMI Trialthe HORIZONSthe HORIZONS--AMI TrialAMI Trial
30 Day Major Bleeding30 Day Major Bleeding
30 Day MACE30 Day MACE
88
101030 Day Major Bleeding30 Day Major Bleeding
8.5
BivalirudinHeparin + GP IIb/IIa
88
101030 Day MACE30 Day MACE
66
88
5 2
7.5
66
88
5.6
7.2
5 2
444.8 5.2
444.6
5.2
00
22
00
22
Pre-treatment(N=2553)
Pre-treatment(N=2553)
NoPre-treatment
(N=1042)
NoPre-treatment
(N=1042)
00
Pre-treatment(N=2553)
Pre-treatment(N=2553)
NoPre-treatment
(N=1042)
NoPre-treatment
(N=1042)
00
Astroulakis Z, Hill JM, Eur Heart J Suppl 2009;11:C13Astroulakis Z, Hill JM, Eur Heart J Suppl 2009;11:C13--C18C18SGE; 0310-3, 71
(N=2553)(N 2553) (N=1042)(N 1042)(N=2553)(N 2553) (N=1042)(N 1042)

Impact of PreImpact of Pre--randomization Heparin in randomization Heparin in the HORIZONSthe HORIZONS AMI TrialAMI Trialthe HORIZONSthe HORIZONS--AMI TrialAMI Trial
30 Day Major Bleeding30 Day Major Bleeding
30 Day MACE30 Day MACE
88
101030 Day Major Bleeding30 Day Major Bleeding
8.5
BivalirudinHeparin + GP IIb/IIa
88
101030 Day MACE30 Day MACE
66
88
5 2
7.5
66
88
5.6
7.2
5 2
444.8 5.2
444.6
5.2
00
22
00
22
Pre-treatment(N=2553)
Pre-treatment(N=2553)
NoPre-treatment
(N=1042)
NoPre-treatment
(N=1042)
00
Pre-treatment(N=2553)
Pre-treatment(N=2553)
NoPre-treatment
(N=1042)
NoPre-treatment
(N=1042)
00
Astroulakis Z, Hill JM, Eur Heart J Suppl 2009;11:C13Astroulakis Z, Hill JM, Eur Heart J Suppl 2009;11:C13--C18C18SGE; 0310-3, 71
(N=2553)(N 2553) (N=1042)(N 1042)(N=2553)(N 2553) (N=1042)(N 1042)

STEMISTEMIImportance of Early Heparin Administrative/HorizonsImportance of Early Heparin Administrative/Horizons
3.03.02 6 Y
P = 0.006P = 0.006
Pre Randomization HeparinPre Randomization Heparin
2.02.0
2.52.52.6 Yes
No
1 01 0
1.51.5%%
0 9
P = 0.02P = 0.02AcuteAcuteStentStent
ThrombosisThrombosis
0.50.5
1.01.0 0.9
0 1
0.8
BivalirudinBivalirudin RandomizedHeparin + GP IRandomized
Heparin + GP I
0.00.00.1
Heparin GP Iepa G
Dangas, ACC 2009Dangas, ACC 2009SGE; 0310-3, 72

Triton TIMI 38 STEMITriton TIMI 38 STEMI
All ACS/PCIAll ACS/PCIpatientspatientsN=13,608N=13,608 2 patients were missing data2 patients were missing data
for primary or secondaryfor primary or secondaryUA/NSTEMIUA/NSTEMIti tti t
STEMI patientsSTEMI patientsN 3 534N 3 534
patientspatientsN=10,074N=10,074
Within 14Within 14days fordays for
N=3,534N=3,534
STEMISTEMI<12 hrs<12 hrs
ongoing orongoing orrecurrentrecurrentischemiaischemia
Secondary PCISecondary PCIN=1,094 (31%)*N=1,094 (31%)*
Primary PCIPrimary PCIN=2,438 (69%)N=2,438 (69%)
PrasugrelPrasugrelClopidogrelClopidogrelPrasugrelPrasugrelClopidogrelClopidogrelN=564N=564N=530N=530N=1,203N=1,203N=1,235N=1,235
Montalescot G et al. Lancet 2009;373:723Montalescot G et al. Lancet 2009;373:723––3131 SGE; 0411-1, 8

STEMI CohortSTEMI CohortN=3534N=3534TRITON TIMITRITON TIMI--3838
15CV Death / MI / Stroke
N 3534N 3534
12.4%ClopidogrelCV Death / MI / Stroke
10
nt (%
) 9.5%
6 5%
10.0%HR 0.79
(0.65-0.97)Prasugrel
5
Perc
en 6.5%
HR 0.68(0 54-0 87)
(0.65 0.97)P=0.02PrasugrelNNT = 42
5 (0.54-0.87)P=0.002 TIMI Major
NonCABG Bleeds Prasugrel 2.42 1
00 30 60 90 180 270 360 450
Clopidogrel2.1
0 30 60 90 180 270 360 450Days From RandomizationMontalescot et al Lancet 2008.Adapted with permission
from Antman EM.SGE; 0410-8, 31

Triton TIMI 38: Stent Thrombosis: Triton TIMI 38: Stent Thrombosis: Definite/ProbableDefinite/ProbableDefinite/ProbableDefinite/Probable
3.03.0Stent Thrombosis (%)Stent Thrombosis (%)
2.8%
2.4%
2.02.0
p=0.02RRR=42%p=0.008
RRR=51%
1.01.0
1.6%1.2%
1.01.0
ClopidogrelPrasugrel
HR=0.58 (0.36–0.93)NNT=83
Time (Days)
0.0
Time (Days)
0.00 450300 350 40025020015050 1000 450300 350 40025020015050 100
Montalescot G et al. Lancet 2009;373:723Montalescot G et al. Lancet 2009;373:723––3131SGE; 0411-1, 10

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
ASA, Prasugrel*,ASA, Prasugrel*,heparin, BB, statinsheparin, BB, statins
*May give with PCI*May give with PCI(clopidogrel needs(clopidogrel needsloading)loading)g)g)
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
How highHow highrisk?risk?
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

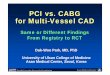
CARESSCARESS--ININ--AMI: DesignAMI: DesignNN gg
•• Designed to address optimum treatment inDesigned to address optimum treatment in•• Designed to address optimum treatment in Designed to address optimum treatment in pts for whom primary PCI not readily pts for whom primary PCI not readily available available a a ab ea a ab e
•• Comparison, after half dose Comparison, after half dose reteplase+abciximab, between routine reteplase+abciximab, between routine etep ase abc ab, bet ee out eetep ase abc ab, bet ee out eimmediate referral for cath/PCI and selective immediate referral for cath/PCI and selective rescue PCI approach in pts who do not rescue PCI approach in pts who do not qualify for primary angioplastyqualify for primary angioplasty
•• High risk patients only (Killip class > 2, EF High risk patients only (Killip class > 2, EF <<35%, ST elevation cumulative > 15 mm)35%, ST elevation cumulative > 15 mm)
Di Mario et al. Lancet 2008;371.559
SGE; 0410-8, 61

CARESSCARESS--ININ--AMI: Primary OutcomeAMI: Primary Outcomeprimary outcome (composite of all cause mortality, reinfarction, & refractory MI within 30 days) occurred significantly less often in the immediate PCI group vs. standard care/rescue PCI group
10.7%
4.4%
HR=0.40 (0.21-0.76)
Di Mario et al. Lancet 2008;371:559.SGE; 0410-8, 64

Transfer AMITransfer AMI
Cath/PCI After Lysis: Routine or Rescue?Cath/PCI After Lysis: Routine or Rescue?
1,059 pts STEMI <12 hrs1,059 pts STEMI <12 hrsand any of: SBP <100, and any of: SBP <100,
Cumulative IncidencePrimary End PointCumulative IncidencePrimary End Point
0.201.01.0
24 - <4824 - <48>48>48
Time from Randomization toCardiac Catherization, (hr)
Time from Randomization toCardiac Catherization, (hr)
HR>100, Killip 2HR>100, Killip 2--3 or3 orRVMl rx’d with TenecteplaseRVMl rx’d with TenecteplaseR R →→routine orroutine or
b d i /PCIb d i /PCI 0 05
0.10
0.15
0 6
0.8
0 6
0.8
9 - <109 - <1010 - <1110 - <1111 - <1211 - <1212 - <2412 - <2424 - <4824 - <48
Routine early PCI
Standard Treatment,(N=463)Standard TreatmentStandard Treatment
Routine early PCI,Routine early PCI,(N=529)(N=529)
rescue based angio/PCIrescue based angio/PCIConcomitant rx:Concomitant rx:
ASA +/ASA +/-- Clopidogrel;Clopidogrel;UF or LMWHUF or LMWH
0 5 10 15 20 25 300.00
0.05
0.4
0.6
0.4
0.6
5 - <65 - <66 - <76 - <77 - <87 - <88 - <98 - <9
9 - <109 <10 Routine early PCI,(N=529)Standard Treatment,Standard Treatment,(N=463)(N=463)
UF or LMWHUF or LMWH11°° endpoint: death, reendpoint: death, re--MI,MI,
rec ischemia, CHF,rec ischemia, CHF,CGS @30 daysCGS @30 days
0.2
Standard TreatmentRoutine early PCI
0.2 p =0.004
1 - <21 - <22 - <32 - <33 - <43 - <44 - <54 - <55 - <65 <6
CGS @30 daysCGS @30 days
Days from Randomization
0.00 5 10 15 20 25 30
0.00 5 10 15 20 25 30
Days from RandomizationN t i kN t i k
No. of Patients0 50 100 150 200
0 - <10 - <11 - <21 <2
0No. of Patients
50 100 150 200
SGE; 0609-6, 29Cantor, NEJM 360:2705, 2009Cantor, NEJM 360:2705, 2009
N at riskN at riskStandardStandard 522522 442442 434434 434434 433433 433433 432432Early PCIEarly PCI 537537 488488 486486 483483 481481 480480 478478

Intervention After FibrinolysisIntervention After Fibrinolysisyy
GRACIA I
Probability of death, non-fatal reinfarction, or ischemia-driven revascularization
30GRACIA I
500 Patients
0 5-12 hrs of sx 10
20
30
Conservative
intervention0.5 12 hrs of sx
ST elevation in ≥ 2 leads
Excluded: shock or pressor Number at riskTime since randomization (months)
0 2 4 6 8 10 120
10
Excluded: shock or pressor dependency
Randomized to either routine cath ± PCI within 24 hrs or
Intervention 248 230 228 226 223 222 221Conservative 251 225 217 211 208 202 195
Probability of death, non-fatal reinfarction
30cath ± PCI within 24 hrs or
Ischemia only driven cath (20% crossover)
10
20
Conservative
1° end pt: death, MI or ischemia reg revasc at 12 months
Number at riskTime since randomization (months)
0 2 4 6 8 10 120
intervention
SGE; 0411-11, 1
Fernandez-Aviles Lancet ‘04Intervention 248 236 235 232 229 228 227Conservative 251 235 230 226 225 221 217

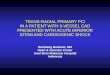
Clinical Outcome at 30 Days Clinical Outcome at 30 Days NORDISTEMINORDISTEMINORDISTEMINORDISTEMI
2020
2525conservative21%21% RR 0.49 (0.27RR 0.49 (0.27--0.89)0.89)
1515
2020 invasiveP=0.03P=0.03
RR 0.45 (0.18RR 0.45 (0.18--1.16)1.16)
1010 10%10% 9.8%9.8%
RR 0.45 (0.18RR 0.45 (0.18 1.16)1.16)P=0.14P=0.14(%)(%)
00
55 4.5%4.5%2.3%2.3% 2.2%2.2%
00Death, reDeath, re--MI, MI, stroke, new stroke, new
ischemiaischemia
Death, reDeath, re--MI, MI, strokestroke
DeathDeath
SGE; 0410-1, 13
Bohmer E. JACC 55:102, 2010 n=266 patients > 90 min from FMCBohmer E. JACC 55:102, 2010 n=266 patients > 90 min from FMC-->PCI, rx’d with >PCI, rx’d with tenecteplase (not selected for high risk) Invasivetenecteplase (not selected for high risk) Invasive-- PCI (89%) 163 min, Cons (71%) PCI (89%) 163 min, Cons (71%) 3 days after TNK3 days after TNK

2009 ACC Guidelines: Triage and Transfer for PCI2009 ACC Guidelines: Triage and Transfer for PCI
All but veryAll but veryLow riskLow risk
SGE; 0410-1, 48FJ Kushner et al., 2009 STEMI Guideline UpdatesFJ Kushner et al., 2009 STEMI Guideline Updates

STEMI: Summary + ConclusionsSTEMI: Summary + Conclusionsyy
•• PCI trumps primary lytics exceptPCI trumps primary lytics excepty yy ysx < 90 min if lytics given quickly (ambulance)sx < 90 min if lytics given quickly (ambulance)very long transfer times (time depends on very long transfer times (time depends on
ti t i k fil )ti t i k fil )patient risk profile)patient risk profile)•• No role for routine facilitated PCINo role for routine facilitated PCI•• If lytics are given moderate and high risk patientsIf lytics are given moderate and high risk patients•• If lytics are given, moderate and high risk patients If lytics are given, moderate and high risk patients
should be transferred for cath/PCI immediately => should be transferred for cath/PCI immediately => “pharmaco“pharmaco--invasive strategy” with adequate antiinvasive strategy” with adequate anti--
l t l t thl t l t thplatelet therapyplatelet therapy•• DAP with prasugrel (except when contraindicated), DAP with prasugrel (except when contraindicated),
early BB, ACEearly BB, ACE--I, statins are also importantI, statins are also importantearly BB, ACEearly BB, ACE I, statins are also importantI, statins are also important
SGE; 1109-9, 32

STEMI Triage for Non Cath Lab HospitalsSTEMI Triage for Non Cath Lab Hospitals
Final WordFinal Word
•• Have protocol for patient transfer in good weather Have protocol for patient transfer in good weather and bad (eg helicopter, ground transport) worked out and bad (eg helicopter, ground transport) worked out with receiving hospital(s)with receiving hospital(s)
P t t i t l i th EDP t t i t l i th ED•• Post triage protocol in the EDPost triage protocol in the ED-- should be relatively simpleshould be relatively simple
should include drugs (minimize iv drips favor drugshould include drugs (minimize iv drips favor drug-- should include drugs (minimize iv drips, favor drug should include drugs (minimize iv drips, favor drug that can be given iv push)that can be given iv push)
•• Post contraindications to lytics alsoPost contraindications to lytics also
SGE; 1109-9, 32
Recommended