
Trauma ServicesTrauma ServicesBackboard Removal Project Backboard Removal Project

First off, we need a volunteer First off, we need a volunteer please……please……

What is a backboard? What is a backboard?
Backboards are frequently used by Pre-hospital to immobilize or extricate patients.
They are hard, non-flexible devices
Used to keep patients immobile when there is concern for spinal injury.

Assess-Are back boards Assess-Are back boards necessary?necessary?
Immediate Concerns with inability to properly assess the patients neck and back
Skin break down, which can happen in a matter of minutes.

Assess-How does this effect Long Assess-How does this effect Long term patient care? term patient care?
“Skin breakdown and the development of pressure ulcers in the Intensive Care Unit (ICU) effect 33% to 56% of critically ill patients and can result in a longer length of stay (LOS), morbidity, and increases costs to health care organizations.”

Why did we look at this process? Why did we look at this process?
CASE REVIEW:Jane was the unrestrained passenger involved in a single auto rollover crash. She was ejected and came to rest under the guard rail when the vehicle rolled over a single time. (At highway speed)
1320 - She was extricated and placed in full spinal immobilization by EMS.
1343 - Arrival to the ED on the back board and she was noted to have no movement of her lower extremities on exam. She was noted to be critically injured.

Her ED Course:
full trauma resuscitation which included Full body x-raysRSI (Rapid Sequence Induction and Intubation)Unsuccessful IV attempts IO placementCentral line placementAdministration of blood products
Her injuries included bilateral rib fractures with a right flail segment, bilateral hemothorax, T9-T10
spine fracture with neuro deficits, and an unstable pelvis fracture.
1640 –Patient was transferred by helicopter to a Level I trauma center in full spinal immobilization. Emergency Department length of stay 2 hours 56 minutes. The patient had a complicated hospital stay at the receiving facility.

Synthesize the Process…. Synthesize the Process….
Review of literature for national trauma standards and best practice:
Society of Trauma Nurses, EAST, ENA, and ATLS all provide evidence based information – standard is to have the patient off of the backboard < 20 minutes.
Evaluate the process in the Emergency Department (ED) for the removal of patients from back boards. The information had to be assessed to know if there a problem or was the occurrence isolated.
Trauma began to educate the staff regarding the need to document the removal of the patients from the backboard. Concurrent review of charts provided the opportunity for timely communication with the ED staff regarding documentation.
The information was entered and tracked through the LUH trauma registry for 6 months.

N= 134 Collection period: January 1st – June 30, 2012
*134 charts were reviewed for length of time the patient remained on the backboard from ED arrival.
* National trauma standard or goal is to remove the backboard < 20 minutes of patient arrival.
52% compliance with standard. Average time to removal - 34 minutesMinimum - on patient arrival- 0 minutes
Maximum - 165 minutes

Design: How did we fix the Design: How did we fix the problem? problem?
After the review of data from the trauma registry and literature, it was felt that we had an opportunity. The information was presented to the Emergency Department and Trauma Committee for review and discussion.
It was felt that LUH should change in process from physician order for removal of backboard to nurses removing patients from the backboard on arrival to the ED.
Policy drafted and approved by trauma committee.
Education of the Emergency Department Physicians and staff.
Ongoing concurrent follow-up and education.
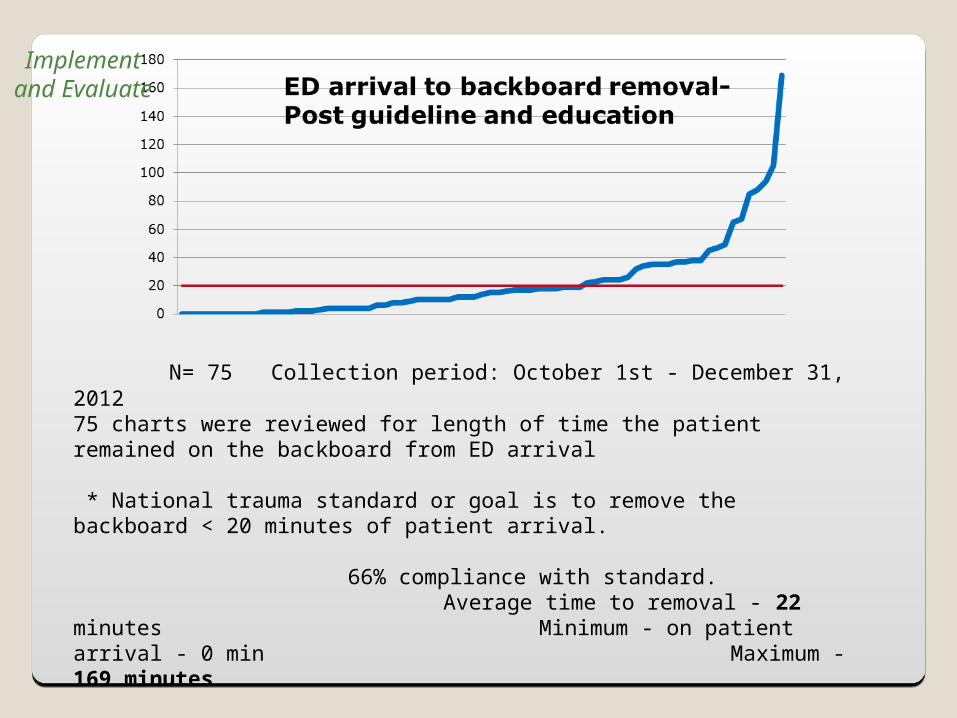
N= 75 Collection period: October 1st - December 31, 2012
75 charts were reviewed for length of time the patient remained on the backboard from ED arrival
* National trauma standard or goal is to remove the backboard < 20 minutes of patient arrival.
66% compliance with standard. Average time to removal - 22 minutes Minimum - on patient arrival - 0 min
Maximum - 169 minutes
Implement and
Evaluate

N= 39Collection period: January 1st - March 31, 2013
* 39 charts were reviewed for length of time the patient remained on the backboard from ED arrival.
* National trauma standard or goal is to remove the
backboard < 20 minutes of patient arrival.
82% compliance with standard. Average time to removal - 13 minutesMinimum - on patient arrival - 0 minMaximum - 65 minutes

Integrate and
Maintain
N= 55Collection period: April 1st- June 30th, 2013
* 55 charts were reviewed for length of time the patient remained on the backboard from ED arrival.
* National trauma standard or goal is to remove the
backboard < 20 minutes of patient arrival.
96% compliance with standard. Average time to removal - 7.8 minutesMinimum - on patient arrival - 0 minMaximum - 62 minutes

What about Pre-Hospital? What about Pre-Hospital?
Decrease the use of Backboards in the Prehospital setting.
June 1st- change in transporting agencies protocols to decrease the use of backboards for transport.

N= 52Collection period: July 1st- Sept 30th, 2013
* 52 charts were reviewed for length of time the patient remained on the backboard from ED arrival.
* National trauma standard or goal is to remove the
backboard < 20 minutes of patient arrival.
98% compliance with standard. Average time to removal - 7.2 minutesMinimum - on patient arrival - 0 minMaximum - 103 minutes

Why does this matter to me? Why does this matter to me?
If we can start reducing the chance of hospital acquired pressure ulcers as early as the Emergency Department our patients may:
Have improved outcomes, and decreased length of stay
Have increased patient satisfaction
Have decreased chance of re-admission

References:
STN: Society of Trauma NursesEAST: Eastern Association for the Surgery of TraumaAmerican College of Surgeons Committee on Trauma. Spine and Spinal Cord Trauma. Advance Trauma Life Support. 7th ed. Chicago IL; American College of Surgeons: 2004:187Centers for Medicare and Medicaid Services, “Hospital Acquired Conditions” dated May 23, 2012 available at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalAcqCond/downloads//HACFactsheet.pdf Annals of Emergency Medicine. Immobilization. 26:1 July, 1995
Recommended

















