-
Transseptal Transcatheter Mitral Valve
Replacement
Howard C. Herrmann, MD, FACC, MSCAI
John Bryfogle Professor of Cardiovascular Medicine and
Surgery
Health System Director for Interventional Cardiology
Director, Cardiac Cath Labs, Hospital of the Univ of PA
Perelman School of Medicine
University of Pennsylvania
Philadelphia
-
Disclosure Statement of Financial Interest
Within the past 12 months, I or my spouse/partner have had a
financial interest/arrangement or affiliation with the
organization(s) listed below.
➢ Discussion may include unapproved and off-label devices,
procedures, and indications
Equity
MicrointerventionalDevices
Consulting Fees/Honoraria
Edwards LifesciencesBayerWells FargoLeering
Grant/Research Support
Abbott Vascular
Edwards Lifesciences
St. Jude Medical
Medtronic
Gore
Siemens
Bayer
Boston Sci
Corvia
Cardiokinetx
Univ Laval
-
TMVR Devices in US EFS
CardiAQ-Edwards
Intrepid
(Medtronic)
Tendyne (Abbott)
Tiara
(Neovasc)Caisson
-
510/17/2017
Caisson transseptal TMVR system
-
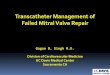
The CardiAQ-EdwardsTM Transcatheter Mitral Valve
Bovine Pericardial Leaflets
Intra-annular Sealing Skirt
Left Atrial Anchors
Left Ventricular Anchors
Tapered Outflow
Open Frame Cells• ONE VALVE, MULTIPLE DELIVERY SYSTEMS• TS –
Transseptal approach
• TA – Transapical approach
• ANCHORING MECHANISM• Preserves chords and utilizes native
leaflets
• Promotes load distribution among annulus, leaflets and
chords
• DESIGNED TO PROMOTE PHYSIOLOGIC FLOW
• Eliminate mitral regurgitation
• Supra-annular position and tapered outflow to minimize risk of
LVOT obstruction
• Intra-annular sealing skirt to minimize PV leak
• Open frame cells to promote atrial flow
-
• FIH Compassionate use experience– Early learning
experience
• Two device iterations, mix of TA and TS access• Enrollment
spanning several years across 6 sites in Europe and Canada
– Very sick compassionate use population with a high burden of
comorbidities – 30 day mortality
• 2/14 procedure related• 4/14 non device or procedure related
(3 multi-organ failure and 1
pneumonia)
• Patient screening for The RELIEF Trial is underway in Europe
and Canada • US EFS trial enrolling: high risk patients• Future
Pipeline
– Reduced delivery profile– Additional valve sizes – Proven
valve tissue – the same bovine pericardial tissue and processes
as
Edwards surgical valves– Delivery system improvements
• Technical improvements expected to make this procedure
easier
The CardiAQ-EdwardsTM TMVRClinical Program Status
Controlled Articulation
-
HPI
89 yo with fatigue and DOE (NYHA class III)
PH: Chronic AF (on warfarin)
s/p PPM
DM
PE: 134/66, 76 irreg irreg, BMI 23 kg/M2
JVD to 10 cm H2O, III/VI HSM at apex
Echo: LV EF 55%
Mild AS (mean grad 6 mmHg, AVA 1.5 cm2)
Severe (4+) MR: EROA 0.48 cm2, RV 61 cc, VC 0.65 cm
Mild-mod RV dysfunction, PASP 36 mmHg
TEE: Failure of leaflet coaptation with mult jets of MR along
the entire line of
coaptation, cleft between P2/P3, RV 85 cc, EROA 0.78 cm2
STS PROM for MV Replacement: 8.2%
Enrolled in the EFS of the CardiAQ TMVI System
-
Imaging
-
CTA Cardiac:
Annulus Diameter and LA Height
-
CTA Cardiac
LVOT Analysis
-
Procedure
• GA and TEE
• Transseptal with septal dilation to 12 mm
• Amplatz super stiff wire curled in the LV apex (A 12 F Reliant
balloon was
passed over the wire to insure no evidence of chordal
entrapment)
• A #40 CardiAQ-Edwards prosthesis was advanced over the wire
and
deployed under TEE and fluoroscopic guidance
• A 20 mm AGA ASO was deployed to close the septostomy
-
Transseptal TMVR with CardiAQ-Edwards
Insertion Positioning
-
Transseptal TMVR with CardiAQ-Edwards
LV Anchor Release
-
Transseptal TMVR with CardiAQ-Edwards
LA Anchor Release Device Release
-
Transseptal TMVR with CardiAQ-Edwards