8/12/2019 Transient Myeloproliferative Disorder: What’s Eosinophilia Got to Do With It?
http://slidepdf.com/reader/full/transient-myeloproliferative-disorder-whats-eosinophilia-got-to-do-with 1/1
Transient Myeloproliferative Disorder: What’s Eosinophilia Got to Do With It?
Wade L. Schulz, PhD1, Malini B. DeSilva, MD2 and R. Scott Velders, MD3 University of Minnesota 1Medical Scientist Training Program and 2Departments of Internal Medicine and Pediatrics; 3Hennepin County Medical Center Pediatrics
References1. Gamis, A. S., & Smith, F. O. ( 2012). Transient myeloproliferative disorder in children with Down syndrome: clarityto this enigmatic disorder.British journal of haematology , 159(3), 277 –87.
2. Ishigaki, H., Miyauchi, J., Yokoe, A., Nakayama, M., et al . (2011). Expression of megakaryocytic and myeloid markers in blasts of transient abnormal myelopoiesis in a stillbirth with Down syndrome: report of histopathological findi ngs of an autopsy case. Human pathology , 42 (1), 141 –5.
3. Kawase, K., Azuma, E., Ohshita, H., Tanaka, T., et al . (2012). Risk factors for early death in transient myeloproliferative disorder without phenotypic features of Down syndrome: a case report and literature review.Journal of pediatric hematology/oncology , 34(6),475 –9.
4. Moiz, B., & Shafiq, M. (2012). Transient myeloproliferative disorder.Blood , 120 (24), 4672 –4672.
5. Seewald, L., Taub, J. W., Maloney, K. W., & McCabe, E. R. B. (2012). Acute leukemias in children with Down syndrome. Molecular genetics and metabolism, 107 (1-2), 25 –30.
6. Shimizu, R., & Yamamoto, M. (2012).Contribution of GATA1 dysfunctionto multi-step leukemogenesis.Cancer science, 103(12), 2039 –44.
7. Suda, J., Eguchi, M., Akiyama, Y., Iwama, Y., et al . (1987). Differentiationof blast cells from a Down’s syndrome patient with transient myeloproliferative disorder. Blood , 69(2), 508 –12.
8. Webb, D., Roberts, I., & Vyas, P. (2007). Haematologyof Down syndrome. Archives of disease in childhood. Fetal and neonatal edition, 92 (6), F503 –7.
9. Zon, L. I., Yamaguchi, Y., Yee, K., Albee, E. a, Kimura, a, Bennett, J. C., Orkin, S. H., et al. (1993). Expression of mRNAf or the GATA-binding proteins in human eosinophils and basophils: potential role in gene transcription. Blood , 81(12), 3234 –41.
Transient Myeloproliferative Disorder
• Occurs in 10% of newborns with Down syndrome
• Often asymptomatic and found incidentally
• In severe cases, TMD can cause respiratory
distress, cardiovascular compromise, and
liver failure
• Peripheral blood characterized by circulating blasts
• Case reports have also described basophilia
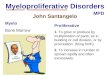
Typical peripheral blood smear in a patient with
transient myeloproliferative disorder. Note the
predominance of blasts with a deeply basophilic
cytoplasm.
Genetics and Differentiation • Proliferation due to mutation in GATA-1 that
accompanies trisomy 21
• No documented cases of eosinophilia
• Monocytes, eosinophils, and megakaryocytes derivedfrom common myeloid progenitor
• Recent studies have shown GATA-1 also regulates
eosinophil differentiation
Case Follow Up and Discussion• Patient remained asymptomatic over hospital course
• Patient’s white cell count continued to decrease spontaneously
• Discharged on 6th day of life with close follow-up by PCP at outside facility
Documented cases of TMD have shown circulating blasts or basophils in the peripheral
blood; however, this case had an unusual presentation. Recent evidence has shown that
the GATA-1 gene product implicated in the development of TMD also controls eosinophil
differentiation. In patients with suspected TMD, the presence of eosinophilia is likely
consistent and may not require additional workup for an infectious cause. While initially
concerning to providers and parents, TMD is normally asymptomatic and spontaneously
resolves, but demands close follow-up due to the increased risk of leukemia.
Initial Presentation• Full-term female infant born to mother of advanced maternal age by C-section
• Physical characteristics of Down syndrome, karyotype revealed 47,XX,+21
• By 30 hours of life, patient developed hyperbilirubinemia and hepatosplenomegaly which
prompted the need for phototherapy and further evaluation
• CBC revealed WBC count of 35.2x109 cells/L with 44% eosinophils
Management and Treatment • Majority of cases resolve spontaneously within weeks
• Treatment with cytarabine (Ara-C) used for symptomatic cases
• Long-term follow-up with CBC every 3-6 months for the first few years of life
due to increased risk of AML (30% of cases by 3 years of age)
• American Academy of Pediatrics recommends counseling parents on signs of
leukemia, including easy bruising, petechiae, increased lethargy, and
changes in feeding
Learning Objectives• Understand the presentation of transient myeloproliferative disorder (TMD)
• Demonstrate variations in the presentation of TMD
• Understand the genetic basis of TMD and cell differentiation
• Recognize findings of TMD that require treatment and potential long-term effects of TMD
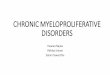
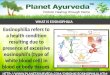
Peripheral Morphology
• Anisopoikilocytosis with evidence of increased red cell regeneration
• Moderate absolute eosinophilia with a subset of immature neutrophils
• Immature subset lacked nuclear segmentation
• Characterized by basophilic and eosinophilic granules
• Platelet count normal with rare circulating megakaryocyte nuclei
Hospital Course• Infant was afebrile, but due to a failed hearing screen she was evaluated for
infectious causes of eosinophilia; CMV and toxoplasma found to be negative
• WBC count declined to 22.5x109 cells/L and eosinophilia resolved by day five of life
• Hyperbilirubinemia resolved, thought to be physiologic jaundice of the newborn
• Final pathology diagnosis of transient myeloproliferative disorder (TMD)
Recommended