Transcatheter Aortic Valve Replacement(TAVR)
NCVH - 2016 Update
Rodney Reeves, MD

• Disclosures: none

3
Current State of TAVR - 2016
» ~350 US Centers performing TAVR » WKHS currently only local institution
performing TAVR(2 ICs, 2 cardiac surgeons) » 2 valve options are currently FDA
approved(Edwards, Medtronic) » Numerous other valves in pipeline/
approval process

4
Current FDA Approved Valves
» Edwards Sapien 3 - balloon expandable » Medtronic Corevalve Evolut R- self-
expanding » Both are excellent valves!!! Both are
reasonable options for the majority of patients.
» Advantages and disadvantages to each….we are still learning best way to individualize choice for each patient

5
» Meet the patient and family(discuss goals/expectations)
» CT » RHC/LHC » Assess risk(PFTs, frailty index,
comorbidities, STS score, etc.) » Surgical Consultation
Pre TAVR workup

6
Day of TAVR
» Team Approach - heart surgeon and interventional cardiologist work together on procedure, both scrubbed
» Lots of help and support!!!(cath lab RNs, rad techs, OR staff, perfusionist on standby, etc.)
» Typically ~ 1 hr, most still general anesthesia, extubate in OR

7
Post-op till Discharge
» Early ambulation » Lines out quickly » Avoidance of sedatives/narcotics » Aspirin/Plavix

Cohesive, Multi-disciplinary Approach Embodies ▪ Optimal patient centric care ▪ Dedication across medical specialties ▪ Collaborative treatment decision
TAVR Heart Team Concept
8
InterventionalCardiologist
CardiologistSurgeon
Valve Clinic Coordinator
CardiacCATH Lab
and O.R. Staff
Anesthe-siologist
ReferringCardiologist
Imaging Specialists TAVR
Heart Team
National Coverage Determination18
The patient (preoperatively and postoperatively) is under
the care of a heart team
2014 Valvular Disease
Guidelines
AHA / ACC
18. National Coverage Determination (NCD) for Transcatheter Aortic Valve Replacement (TAVR). 2012.

Pre-screening Review of Records
Clinical Evaluation
Gated CTA (Chest / Abdomen / Pelvis)
RHC / LHC Coronary Angiography
Functional Status Assessment (Cognitive Function, Frailty, etc.)
STS Score Calculation
Treatment Plan
TAVR Evaluation Pathway
9
Note: The above is a suggested flow for the patient screening process, however, the order in which screening tests are conducted varies depending on the patient’s profile and should be at the discretion of the Heart Team.

TAVR Patients May Present with Some of the Following
Characteristics of a TAVR Patient19
10
Old age
Reduced EF
Prior CABG
History of stroke/CVA
History of AFib
Prior chest radiation
Prior open chest surgery
Heavily calcified aorta
History of CAD
History of COPD
History of renal insufficiency
Frailty
History of syncope
Fatigue, slow gait
Peripheral vascular disease Diabetes and hypertension
Severe, Symptomatic Native Aortic Valve Stenosis
19. Leon M et al. New England Journal of Medicine 2010 October 21;363(17):1597-1607.

11
Alain Cribier: First Human TranscatheterValve Replacement (2002)

What Causes Aortic Stenosis in Adults?
More CommonLess Common
12
Images courtesy of John Webb, MD at St. Paul’s Hospital and Renu Virmani, MD at the CVPath Institute
Age-Related Calcific Aortic
StenosisCongenital
AbnormalityRheumatic
Fever

Population at Risk for Aortic Stenosis is Increasing
13
▪ Aortic Stenosis is estimated to be prevalent with 12.4% of the population over the age of 75.2
▪ The elderly population will more than double between now and the year 2050, to 80 million.3
▪ 80% of adults with symptomatic aortic stenosis are male4
Approx. 2.5 Million People in the U.S. Over the Age of 75 suffer from this
disease.1
ELDERLY AVERAGE ANNUAL GROWTH RATE: 1910 to 2030
0.0%
4.0%
1910-1930 1950-1970 1990-2010
2.8%
1.3%
2.2%2.4%
3.1%
2.6%
1. U.S. Census Bureau, Population Division. June 2015; 2. Ruben L.J.et al. Heart. 2000;84:211-21; 3. U.S. Census Bureau Statistical Brief. May 1995; 4. Ramaraj R, Sorrell VL. Br Med J 2008;336: 550–5.

▪ Shortness of breath ▪ Angina ▪ Fatigue ▪ Syncope or Presyncope ▪ Other ▪ Rapid or irregular heartbeat ▪ Palpitations
Symptoms of Aortic Stenosis
14
The symptoms of aortic disease are commonly misunderstood by patients as ‘normal’ signs of aging.5 Many patients initially appear asymptomatic, but on closer examination up to37% exhibit symptoms.6
Sandy Severe Aortic Stenosis
(Actual Patient)
5. Das P. European Heart Journal. 2005;26:1309-1313; 6 . Lester SJ et al. CHEST 1998;113(4):1109-1114.

After the onset of symptoms, patients with severe aortic stenosis have a survival rate as low as 50% at2 years and 20%at 5 years without aortic valve replacement7
Severe Aortic Stenosis is Life Threateningand Treatment is Critical6
15
50% of patients died within 1 year without valve replacementPer the Inoperable Cohort of the PARTNER Trial
100%
80%
60%
40%
20%
00 40 50 60 70
Age, Years
Sur
viva
l, %
Onset Severe Symptoms
Average Survival, y
Angina
Syncope
Failure
0 2 4 6
Latent Period(Increasing Obstruction, Myocardial Overload)
ADULTS AVERAGE COURSE WITH VALVULAR AORTIC STENOSIS
6. Lester SJ et al. CHEST 1998;113(4):1109-1114; 7. Otto CM. Heart. 2000:84:211-218.

5-YEAR SURVIVAL(Distant Metastasis)8
Sur
viva
l, %
16
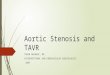
Worse Prognosis than Many Metastatic Cancers
5 year survival of breast cancer, lung cancer, prostate cancer, ovarian cancer and severe inoperable aortic stenosis
0
5
10
15
20
25
30
35
Breast Cancer Lung Cancer Colorectal Cancer Prostate Cancer Ovarian Cancer Severe Inoperable AS*
3
2830
12
4
23
*Using constant hazard ratio. Data on file, Edwards Lifesciences LLC. Analysis courtesy of Murat Tuczu, MD, Cleveland Clinic
8. National Institutes of Health. http://seer.cancer.gov/statfacts/. Accessed Nov. 2010.

▪ In the absence of serious comorbid conditions, aortic valve replacement (AVR) is indicated in the majority of symptomatic patients with severe aortic stenosis
▪ Consultation with or referral to a Heart Valve Center of Excellence is reasonable when discussing treatment options for: ▪ Asymptomatic patients with severe valvular heart disease ▪ Patients with multiple comorbidities for whom valve intervention
is considered ▪ Because of the risk of sudden death, replacing the aortic
valve should be performed promptly after the onset of symptoms
▪ Age is not a contraindication to surgery
Timely Intervention is Critical for Patients with Symptoms9
17
2014 Valvular Disease
Guidelines
AHA / ACC
9. Nishimura RA et al. JACC. 2014. doi: 10.1016/j.jacc.2014.02.537.

Definition Valve Hemodynamics
High-gradient severe aortic stenosis
▪ Aortic jet velocity ≥ 4 m/s or mean gradient ≥ 40 mmHg ▪ Or aortic valve area index ≤ 0.6 cm2/m2
Low-flow/low-gradient with reduced left ventricular ejection fraction
▪ Resting aortic jet velocity < 4m/s or mean gradient < 40 mmHg ▪ Dobutamine stress echocardiography shows aortic valve area ≤ 1.0
cm2 with aortic jet velocity ≥ 4m/s at any flow rate ▪ Left ventricular ejection fraction < 50%
Low-gradient with normal left ventricular ejection fraction or paradoxical low-flow
▪ Aortic jet velocity < 4m/s or mean gradient < 40 mmHg ▪ Indexed aortic valve area ≤ 0.6 cm2/m2
▪ Stroke volume index < 35 mL/m2 measured when patient is normotensive (systolic blood pressure < 140 mmHg)
▪ Left ventricular ejection fraction ≥ 50%
Patients with severe aortic stenosis typicallyhave an aortic valve area ≤ 1.0 cm2
Symptoms: Dyspnea or decreased exercise tolerance, heart failure, angina, syncope and presyncope
Definition of Severe Aortic Stenosis9
18
2014 Valvular Disease
Guidelines
AHA / ACC
9. Nishimura RA et al. JACC. 2014. doi: 10.1016/j.jacc.2014.02.537.

▪ Dobutamine stress echocardiography canbe used to differentiate between true and pseudo severe aortic stenosis ▪ Better define the severity of the aortic stenosis ▪ Accurately assess contractile / pump reserve
▪ Some patients with severe aortic stenosis based on valve area have a lower than expected gradient (e.g. mean gradient < 30 mmHg) despite preserved LV ejection fraction (e.g. EF > 50%) ▪ Up to 35% of patients with severe aortic
stenosis present with low flow, low gradient ▪ These low gradients often lead to an under
estimation of the severity of the disease,so many of these patients do not undergo surgical aortic valve replacement
Paradoxical Low Flow and/or Low GradientSevere Aortic Stenosis10
19
Dobutamine stress in low gradient, low ejection fractionAS Chambers, Heart. 2006 April; 92(4): 554–558
10. Dumesnil et al. European Heart Journal 2010; 31, 281-289.

20
UNDERTREATEMENT OF AORTIC STENOSIS
Pat
ient
s, %
Studies show that patients with severe aortic stenosis are under-diagnosed and under-treated
0%
20%
40%
60%
80%
100%
Bouma 1999 Pellikka 2005 Charison 2006 Varadarajan 2006 January 2009 Bach 2009 Freed 2010
69%52%
74%61%60%43%54%
31%48%
26%39%40%57%46%
Aortic Valve Replacement (AVR) No AVR
At Least 40% of Patients Who Need Valve Replacement Do Not Get Treatment11-17
11. Bouma BJ et al. Heart. 1999;82:143-148; 12. Pellikka PA et al. Circulation. 2005;111:3290-3295; 13. Charlson E et al. J Heart Valve Dis. 2006;15:312-321; 14. Varadarajan P et al. Ann Thorac Surg. 2006;82:2111-2115; 15. Jan F et al. Circulation. 2009;120;S753; 16. Bach DS et al. Circ Cardiovasc Qual Outcomes. 2009;2:533-539; 17. Freed BH et al. Am J Cardiol. 2010;105:1339-1342.

▪ Despite frequent BAV, standard therapy did not alter the dismal course of disease for inoperable patients in the PARTNER Trial ▪ 51% died within 1 year ▪ 94% died within 5 years
21
T H E P A R T N E R T R I A L
* In an age and gender matched US population without comorbidities, the mortality at 5 years is 40.5%.
All-
Cau
se M
orta
lity
(%)
Months
HR [95% CI] = 0.50 [0.39, 0.65] p (log rank) < 0.0001
Control Group (Med Rx and BAV) (n = 179)
50.7%
68.0%
87.5%80.9%
93.6%
Medical Management and BAV are Inadequate Therapies for Inoperable Patients

Therapy
Low- to Moderate-Risk
High Risk
Greater Risk
Transcatheter Aortic Valve Replacement
(TAVR)
Open-Heart Surgery (AVR)
Options for Aortic Valve Replacement per Guidelines9
Transcatheter Heart Valve
Surgical Heart Valve
22
Severe Aortic Stenosis is Defined as: Valve Area < 1.0 cm2
Mean Gradient > 40 mmHg OR Jet Velocity > 4.0 m/s
High Risk Patients Defined by STS Risk
Score > 8%
9. Nishimura RA et al. JACC. 2014. doi: 10.1016/j.jacc.2014.02.537.

Society of Thoracic Surgeons operative risk score≥ 8% OR at a ≥ 15% risk of mortality (at 30 days)
For relief of aortic stenosis in patients with ▪ Symptomatic heart disease due to severe native calcific aortic stenosis ▪ Have native anatomy appropriate for the valve delivery system ▪ Evaluated by a Heart Team, including a cardiac surgeon, to be at high or
greater risk for open surgical therapy
Edwards SAPIEN 3 Transcatheter Heart Valve
23

24

25

26

TAVR is Better than Medical Managementfor Inoperable Patients
27
Edwards SAPIEN Valves
Significantly Improve Survival

Edwards SAPIEN is superior to medical management in inoperable patients
TAVR is Better than Medical Managementfor Inoperable Patients
27
TAVR with Edwards SAPIEN valves is a reasonable alternative to surgery
Edwards SAPIEN 3 valve: Transformational design
Edwards SAPIEN Valves
Significantly Improve Survival

Edwards SAPIEN is superior to medical management in inoperable patients
TAVR is Better than Medical Managementfor Inoperable Patients
27
TAVR with Edwards SAPIEN valves is a reasonable alternative to surgery
Edwards SAPIEN 3 valve: Transformational design
TAVR is superior to medical management for Inoperable Patients
Edwards SAPIEN Valves
Significantly Improve Survival

Without treatment 94% of patients in the standard therapy groupdied within
5 years
21.8% absolute reduction in mortality at
5 years
Standard Therapy is an Ineffective Treatmentfor Severe Aortic Stenosis Patients
71.8%
Months
HR [95% CI] = 0.50 [0.39, 0.65] p (log rank) < 0.0001
93.6%
Standard therapy includes medical management and BAV
28
All-
Cau
se M
orta
lity
(%)
0 12 24 36 48 60
100%
80%
60%
40%
20%
0%
Standard Rx (n = 179)TAVR (n = 179)
50.7%
30.7%
A L L - C A U S E M O R T A L I T Y I n o p e r a b l e C o h o r t

87.3% of patients
with standard therapy were rehospitalized
for cardiac issues
39.7% absolute reduction of
rehospitilizationat 5 years
Standard Therapy Patients Were RehospitalizedTwice as Often as TAVR Patients
Standard therapy includes medical management and BAV
29
Months
100%
80%
60%
40%
20%
0%
87.3%
47.6%
Standard Rx (n = 179)
HR [95% CI] = 0.40 [0.29, 0.55] p (log rank) < 0.0001
0 12 24 36 48 60
TAVR (n = 179)
Hos
pita
lity
(%)
R E H O S P I T A L I Z A T I O N I n o p e r a b l e C o h o r t

TAVR with Edwards SAPIEN Valvesis Equivalent to Surgery
30
With the Benefits of a Less Invasive
Procedure

TAVR is superior to medical management for Inoperable Patients
TAVR with Edwards SAPIEN Valvesis Equivalent to Surgery
30
Edwards SAPIEN valve is a reasonable alternative to surgery in high-risk patients
Edwards SAPIEN 3 valve: Transformational design
With the Benefits of a Less Invasive
Procedure

TAVR is superior to medical management for Inoperable Patients
TAVR with Edwards SAPIEN Valvesis Equivalent to Surgery
30
Edwards SAPIEN valve is a reasonable alternative to surgery in high-risk patients
Edwards SAPIEN 3 valve: Transformational design
TAVR with Edwards SAPIEN valves is a reasonable alternative to surgery
With the Benefits of a Less Invasive
Procedure

At 5 Years
Patients that had TAVR with the Edwards SAPIEN
valve showed survival
equivalent to SAVR
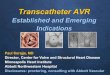
TAVR is Equivalent to Surgery in High-Risk Patients
31
Per ACC / AHA Guidelines, TAVR is a reasonable alternative to surgery in patientswho meet an indication for AVR and who have high surgical risk for surgical AVR9
Error Bars Represent95% Confidence Limits
All-
Cau
se M
orta
lity
(%)
Months Post Randomization0 12 24 36 48 60
100%
80%
60%
40%
20%
0%
SAVRTAVR
HR [95% CI] = 1.04 [0.86, 1.24] p (log rank) = 0.76
67.8%
62.4%
No. at Risk
TAVR 348 262 228 191 154 61SAVR 351 236 210 174 131 64
A L L C A U S E M O R T A L I T Y A t 5 Y e a r s
9. Nishimura RA et al. JACC. 2014. doi: 10.1016/j.jacc.2014.02.537.

At both 1 year and 5 year follow up, 85% of Patients treated with the Edwards SAPIEN valve were in NYHA Class I or II compared to only 6% at baseline.
TAVR SAVR TAVR SAVR TAVR SAVR TAVR SAVR348 349 250 226 165 145 100 97
Baseline 1 Year 3 Years 5 Years
p = 0.64 p = 0.91 p = 0.35 p = 0.9313%15% 14%100%
80%
60%
40%
20%
0%
19%15%
94%94%
20%P
erce
nt o
f Eva
luab
le E
choe
s
I II III IV
Patients Continued to Show Improved Symptom Relief 5 Years After TAVR
32
NYHA CLASS OVER T IME

Longest Follow-Up in Any TAVR Randomized Study
33
5 YEARS of PROVEN VALVE DURABILITY ▪ Sustained hemodynamic performance ▪ No incidence of structural valve deterioration requiring surgical valve
replacement20 ▪ Significant and sustained improvement in functional heart class
The PARTNER Trial 5-Year Results
TAVR vs. Standard Therapy in Inoperable Patients
▪ Significant mortality benefit ▪ Statistically significant reduction in
hospitalization ▪ NNT is 5 patients to save a life
TAVR vs. Surgical AVR in High-Risk Patients
▪ Equivalent mortality benefit ▪ Persistent symptom relief
20. Lancet. 2015 Jun 20;385(9986):2477-84. doi: 10.1016/S0140-6736(15)60308-7. Epub 2015 Mar 15.

Now Approved: The Edwards SAPIEN 3 Valve
34

TAVR is superior to medical management for inoperable patients
TAVR is a reasonable alternative to surgery for high-risk patients
Transformational advance in valve design: Edwards SAPIEN 3 Valve
Now Approved: The Edwards SAPIEN 3 Valve
34

TAVR is superior to medical management for inoperable patients
TAVR is a reasonable alternative to surgery for high-risk patients
Transformational advance in valve design: Edwards SAPIEN 3 Valve
Now Approved: The Edwards SAPIEN 3 Valve
Edwards SAPIEN 3 valve: Transformational design
34
Unprecedented Clinical
Outcomes

All-Cause Mortality of the 491 patients in the PARTNER II Trial was 1.6% at 30 days
Cardiovascular Mortality was 1.0%
Low Mortality at 30 DaysThe PARTNER II Trial: SAPIEN 3 Valve High-Risk
1%
26%
50%
75%
100%
High-Risk (TF)
1%1.60%
All-Cause Cardiovascular
35
MORTALITY (As Treated Patients)

0%
20%
PARTNER I B (TF) PARTNER I A (All) PARTNER I A (TF) PARTNER II B (TF) PARTNER II B (TF) PARTNER II HR (TF)
2%
4%5%
4%5%
6%
ALL-CAUSE MORTALITY a t 30 DAYS PARTNER I Trial and PARTNER II Trial
All-Cause Mortality Has Decreased Overall
175 344 240 271 282 491
SAPIEN Valve SAPIEN XT Valve SAPIEN 3 Valve
36

Low Stroke at 30 DaysThe PARTNER II Trial: SAPIEN 3 Valve HR
0%
25%
50%
75%
100%
High-Risk (TF)
0.8%
Disabling
37
DISABLING STROKE (As Trea ted Pa t ien ts )
Of the 491 Patients in the PARTNER II Trial: Disabling Stroke was 0.8% at 30 days

Other Clinical Events at 30 Days (as Treated Patients)*
SAPIEN 3 Valve HR TF
Events (%) (n = 491)Major Vascular Comps. 5.3Bleeding – Life Threatening 5.5
*PARTNER II Trial high-risk TF SAPIEN 3 valve cohort 30-day results.

39
Femoral Case Example

40

40

41

41

42

42

43
Transapical Case Example










47
Where is all this going?
» Number and indication for procedure is growing
» Moving towards a “minimalist” approach » Eventually, the great, great majority of
these Aortic Stenosis cases will be done via TAVR(as opposed to traditional surgery)
» Therapies for Mitral and Tricuspid Valves is evolving quickly

48
Case Examples:

49
Valve in Valve with Corevalve Evolut R
» 86 yo male » History of 23mm Medtronic Mosaic Valve ~
15 years ago » Now with bioprosthetic valve stenosis » 3 recent CHF admits » Mean gradient ~35, EF 15%

50

50

51

51

52

52

53
Edwards Sapien 3
» 88 yo WM » NYHA Class III » Good functional capacity

54

54

55

55

56

56

57
Recommended