Transcatheter Aortic Valve Replacement with a 34–mm Repositionable Self-Expanding Bioprosthesis
Tanvir Bajwa, MDSt. Luke’s Medical Center/ Aurora Health Care, Milwaukee, WIFor the Evolut R 34 mm US Investigators

BACKGROUND
• Transcatheter aortic valve (TAV) selection depends on industry guidance on valve dimensions and aortic annuli measurements.
• Insufficient sizing of either self-expanding1 or balloon expandable transcatheter valves2 has been associated with more paravalvular leak (PVL).
• 8.5% of patients treated with the 31–mm CoreValve self-expanding valve were implanted in annuli > maximum range1, which implies the need for even larger valve sizes.
• We evaluated a new 34–mm self-expanding, repositionable valve for native aortic annuli 26 – 30 mm in diameter (perimeters 81.7 –94.2 mm).
2
1 Popma JJ, et al. Circ Cardiovasc Interv 2016; doi: 10.1161/CIRCINTERVENTIONS.115.003282. 2Yang TH et al. J Am Coll Cardiol Intv2015;8:462–71.

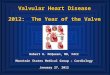
EVOLUT R VALVE SIZES
Evolut R 26 mm Evolut R 29 mm
Diameter, mm 18 – 20 20 – 23 23 – 26 26 – 30
Perimeter, mm 56.5 – 62.8 62.8 – 72.3 72.3 – 81.7 81.7 – 94.2
Evolut R 23 mm Evolut R 34 mm
3
Annular

EVOLUT R 34 MM METHODS
• 60 Patients implanted at 10 sites in the US• CT-measured perimeter-derived annulus sizing• CT-measured sinus of Valsalva dimension requirements
– Heights (aortic annular plane to the tallest point in each sinus) ≥ 15 mm
– Diameters (for each commissure) ≥ 29 mm• Device annulus ratio = [valve perimeter-annulus perimeter)/
annular perimeter] x 100• Independent echocardiographic assessment (Mayo
Echocardiographic Core Laboratory, Rochester, MN)• VARC-2 endpoint definitions.
4

Characteristic, mean± SD or % N = 60Age, years 81.8 ± 8.2Male 96.7BSA, m2 2.1 ± 0.2STS PROM, % 5.5 ± 2.8New York Heart Association class III or IV 63.3Frailty 61.0Chronic lung disease (COPD) 44.8Peripheral vascular disease 43.3Diabetes 41.7Atrial fibrillation / atrial flutter 36.7Coronary artery bypass grafting 30.0Left ventricular ejection fraction, %* 55.9 ± 13.2Pre-existing permanent pacemaker 11.7
EVOLUT R 34 MM PATIENT CHARACTERISTICS
5
*Site-reported.

EVOLUT R 34 MM PROCEDURAL CHARACTERISTICS
% or mean ± SD N=60General anesthesia 56.7
Transfemoral access 100
InLine Sheath used 63.3
Pre-TAVR balloon dilation 62.7
Resheath or recapture 33.3
Post-implant dilation 36.7
Multiple valve (≥ 2 implanted) 1.7
Mean sinus of Valsalva height, mm 23.5 ± 4.4
Coronary obstruction 0.0
Perimeter > 91.1 mm 13.3
Device annular ratio 22.2 ± 4.9
Device annular ratio ≥ 15% 91.7
6

% 1–7 DaysN = 60
Absence of procedural mortality 98.3
Correct positioning of 1 valve in proper anatomical location 98.3
Intended performance of the prosthetic valve 83.0
Absence of patient prosthesis mismatch 83.3
Mean gradient < 20 mm Hg or peak velocity < 3 m/sec 100
Absence of ≥ moderate prosthetic regurgitation 100
EVOLUT R 34 MM VARC-2 OUTCOMES
7

EVOLUT R 34 MM VALVE PERFORMANCE
8
Gradient 60 59 58 52
EOA 52 54 53 48

EVOLUT R 34 MM PARAVALVULAR LEAK
Independent core-lab adjudication
9

Event, No. of patients (K-M rates as %)30 DaysN = 60
6 MonthsN = 60
All-cause mortality 1 (1.7) 5 (8.3)
Cardiovascular mortality 1 (1.7) 4 ( 6.7)
Disabling stroke 0.0 (0) 1 (1.7)
Major vascular complication 1 (1.7) 1 (1.7)
Life-threatening/disabling bleeding 1 (1.7) 2 (3.4)
Acute kidney injury 0 (0.0 0 (0.0)
Valve thrombosis 0 (0.0) 0 (0.0)
Embolization 1 (1.7) 1 (1.7)
Pacemaker 11 (18.4) 13 (21.8)
EVOLUT R 34 MM SAFETY OUTCOMES
10

EVOLUT R 34 MM NEW YORK HEART ASSOCIATION
86.8% of Survivors Improved NYHA Class at 6 Months
11

• Patients with a broader range of aortic annuli can now be treated with TAVR
• Proper sizing in patients with large aortic annuli suggests low rates of PVL
• Vascular complications and bleeding rates were low in this primarily male patient cohort.
• The 34–mm Evolut R valve showed excellent hemodynamics consistent with other Evolut R valves.
EVOLUT R 34 MM SUMMARY
12
Recommended