The Importance of the INTERACT™ 4.0 Quality Improvement Program-
Today’s Post Acute Care Environment
1
INTERACT
Lisa Thomson, Chief Strategy and Marketing Officer Sue LaGrange, Director of Education Pathway Health
Objectives
• Describe the current landscape of health care reform and funding that make the INTERACT™ 4.0 Quality Improvement Program an essential QI initiative for long-term care organizations.
• Articulate the key strategies that form the foundation of the INTERACT™ 4.0 Quality Improvement Program.
• Identify 3 key strategies facilities can implement to improve both quality and reduction of unnecessary hospitalizations
2

© FLORIDA ATLANTIC UNIVERSITY WITH PERMISSION FROM PATHWAY HEALTH, INC. -- ALL RIGHTS RESERVED. COPY WITH PERMISSION ONLY. 3

© Florida Atlantic University with permission from Pathway Health, Inc. -- All Rights Reserved. Copy with permission only. 4

5 © Florida Atlantic University with permission from Pathway Health, Inc. -- All Rights Reserved. Copy with permission only.
6
CMS Objective
• Passive – FFS
• Active – VBP
• Quality

CMS Goal
7

LEGISLATIVE
VBP Initiatives & Regulations
8
Legislative Initiatives
9
Affordable Care Act IMPACT Act
Protecting Access to Medicare Act
(PAMA)
Value-Based Purchasing (SNFVBP)
Quality Reporting Program (QRP)
Requirements of Participation
National Quality Strategies
CMS State Operations Manual: Appendix PP
10
https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/som107ap_pp_guidelines_ltcf.pdf
11
Website has changed: http://www.pathway-interact.com/
“Interventions to Reduce Acute Care Transfers (INTERACT) is a program with several resources aimed at improving staff competencies in this area https://interact2.net/tools_v4.html.” “Staff may inform surveyors of the tools they use to help show evidence of the required competencies. However, merely stating or referencing the tools is not enough on its own to verify compliance. Staff must also demonstrate that they possess the competency to use the tools in a manner that accomplishes their purpose, of aiding to effectively identify and address resident changes in condition.”
https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/som107ap_pp_guidelines_ltcf.pdf
CMS State Operations Manual: Appendix PP
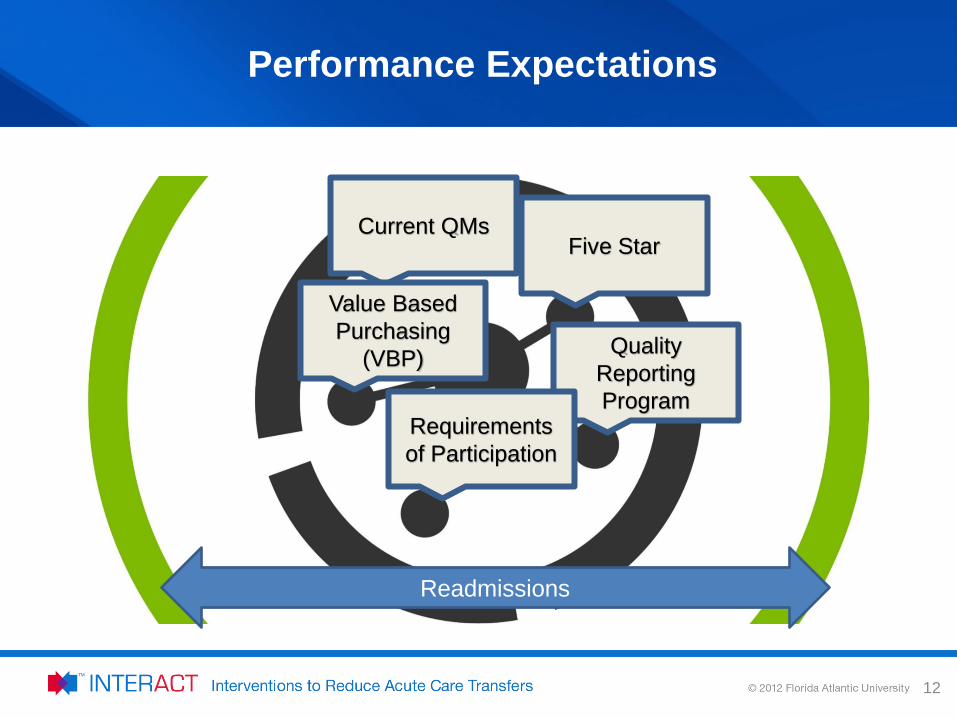
Performance Expectations
12
Current QMs
Value Based Purchasing
(VBP) Quality Reporting Program
Requirements of Participation
Five Star
Readmissions

13
Readmission Focus © FLORIDA ATLANTIC UNIVERSITY WITH PERMISSION FROM PATHWAY HEALTH, INC. -- ALL RIGHTS RESERVED. COPY WITH PERMISSION ONLY. 14
Quality Measure
Numerous Readmission Measures
SNFVBP - SNFRM SNFQRP- SNFPPR Five Star-Short Stay Readmission and ED
IMPROVE OUTCOMES
Evidenced Based
16
Overview of the INTERACT™ QIP
Is a quality improvement program designed to improve the care of nursing home residents with
acute changes in condition
http://www.pathway-interact.com
17
Where it all began…
Joseph G. Ouslander, M.D. is Professor and Senior Associate Dean for Geriatric Programs at the Charles E. Schmidt College of Medicine, and Professor at the Christine E. Lynn College of Nursing of Florida Atlantic University in Boca Raton Florida. He is a past-President of the American Geriatrics Society and is the Executive Editor of the society's Journal. He is a co-author of Essentials of Clinical Geriatrics and Medical Care in the Nursing Home, and an editor of Hazzard's Textbook of Geriatric Medicine and Gerontology.
Dr. Ouslander’s work is now focused on improving the quality of care and quality of life for older people, and reducing unnecessary health care expenditures through programs such as INTERACT.
18
Overview of the INTERACT™ QIP
The INTERACT Interdisciplinary Team Joseph G. Ouslander, MD Florida Atlantic University Jill Shutes, GNP Florida Atlantic University Ruth Tappen, EdD, RN, FAAN Florida Atlantic University Gabriellla Engstrom, PhD, RN Florida Atlantic University Nancy Henry, PhD, GNP Florida Atlantic University Maria Rojido, MD Florida Atlantic University David Wolf, Ph.D., CNHA Florida Atlantic University Sanya Diaz, MD Florida Atlantic University Laurie Herndon, MSN, GNP-BC Mass Senior Care Foundation Alice Bonner, PhD, GNP Northeastern University Jo Taylor, RN, MPH Carolinas Center for Medical Excellence Gerri Lamb, PhD, RN, FAAN Arizona State University Annie Rahman, PhD, MSW USC Davis School of Gerontology Dan Osterweil, MD California Association of LTC Medicine Amy E. Boutwell, MD, MPP Collaborative Healthcare Strategies Adrienne Mihelic, PhD Colorado Foundation for Medical Care Mary Perloe, GNP Georgia Medical Care Foundation John Schnelle, PhD Vanderbilt University
In collaboration with many participating LTC professionals and facilities
19
Acknowledgement
20
The INTERACT™ Program and Tools were initially developed by: Joseph G. Ouslander, MD and Mary Perloe, MS, GNP at the Georgia Medical Care Foundation with the support of a contract from the Centers for Medicare & Medicaid Services (CMS).
HISTORY of INTERACT
Implementation Model in the Commonwealth Fund Grant Collaborative:
• On site training
• Facility-based champion
• Collaborative phone calls
• Completion and faxing of QI Review
(c) Pathway Health Services, Inc. - All Rights Reserved. Copy with Permission Only 21
Ouslander et al, J Am Geriatr Soc 59:745–753, 2011
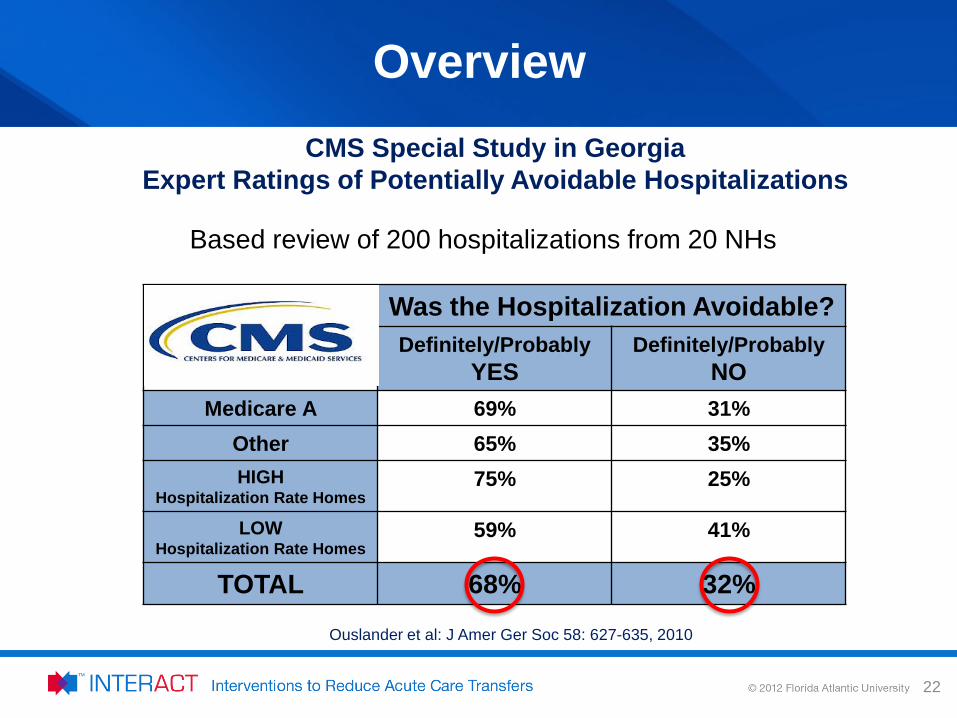
Overview
Was the Hospitalization Avoidable? Definitely/Probably
YES Definitely/Probably
NO Medicare A 69% 31%
Other 65% 35% HIGH
Hospitalization Rate Homes 75% 25%
LOW Hospitalization Rate Homes
59% 41%
TOTAL 68% 32%
CMS Special Study in Georgia Expert Ratings of Potentially Avoidable Hospitalizations
Ouslander et al: J Amer Ger Soc 58: 627-635, 2010
Based review of 200 hospitalizations from 20 NHs
22
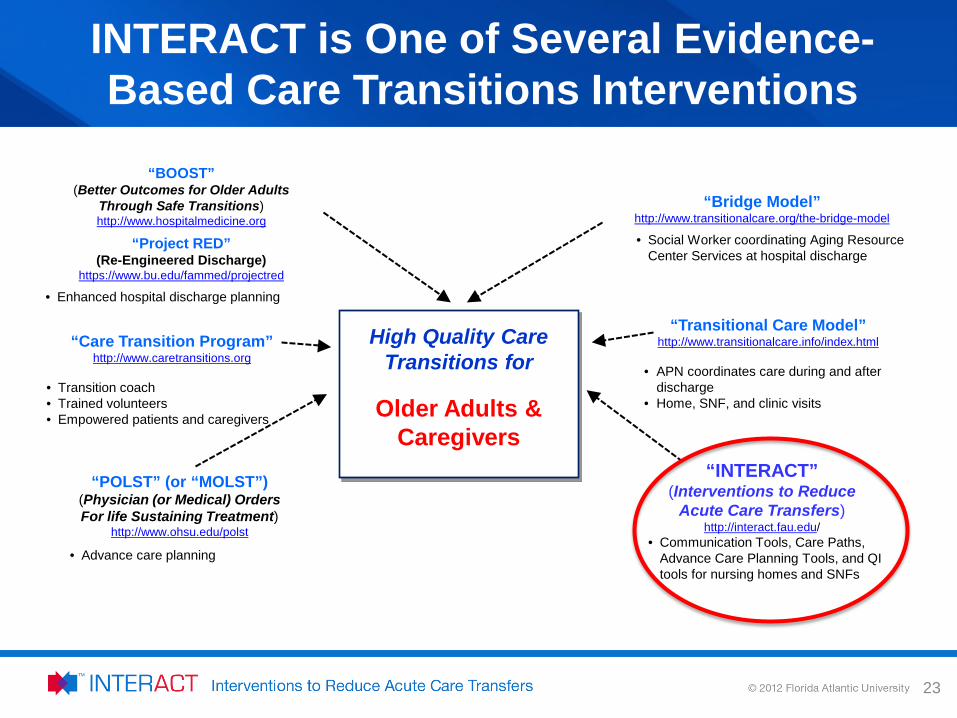
“BOOST” (Better Outcomes for Older Adults
Through Safe Transitions) http://www.hospitalmedicine.org
“Project RED” (Re-Engineered Discharge)
https://www.bu.edu/fammed/projectred
• Enhanced hospital discharge planning
“Care Transition Program” http://www.caretransitions.org
• Transition coach • Trained volunteers • Empowered patients and caregivers
“POLST” (or “MOLST”) (Physician (or Medical) Orders For life Sustaining Treatment)
http://www.ohsu.edu/polst
• Advance care planning
“Bridge Model” http://www.transitionalcare.org/the-bridge-model
• Social Worker coordinating Aging Resource Center Services at hospital discharge
“Transitional Care Model” http://www.transitionalcare.info/index.html
• APN coordinates care during and after
discharge • Home, SNF, and clinic visits
“INTERACT” (Interventions to Reduce
Acute Care Transfers) http://interact.fau.edu/
• Communication Tools, Care Paths, Advance Care Planning Tools, and QI tools for nursing homes and SNFs
High Quality Care Transitions for
Older Adults &
Caregivers
INTERACT is One of Several Evidence-Based Care Transitions Interventions
23
Overview of the INTERACT™ QIP
Includes evidence and expert-recommended clinical practice tools, strategies to implement them, and related educational resources
The basic program is located on the internet:
http://www.pathway-interact.com
24
Overview of the INTERACT™ QIP
INTERACT Strategies 1. Prevent conditions from becoming severe enough to require
hospitalization through early identification and evaluation of changes in resident condition
2. Manage some conditions without transfer when this is feasible and safe
3. Improve advance care planning and the use of palliative care plans when appropriate as an alternative to hospitalization for some residents
4. Improve communication and documentation within LTC facilities and programs, and between LTC and acute care
5. Integrate into ongoing QI initiatives (e.g. QAPI)
6. Embed in Health Information Technology across care settings
25
Quality Improvement Tools
Communication Tools
Decision Support Tools
Advance Care Planning Tools
Overview of the INTERACT™ QIP
26
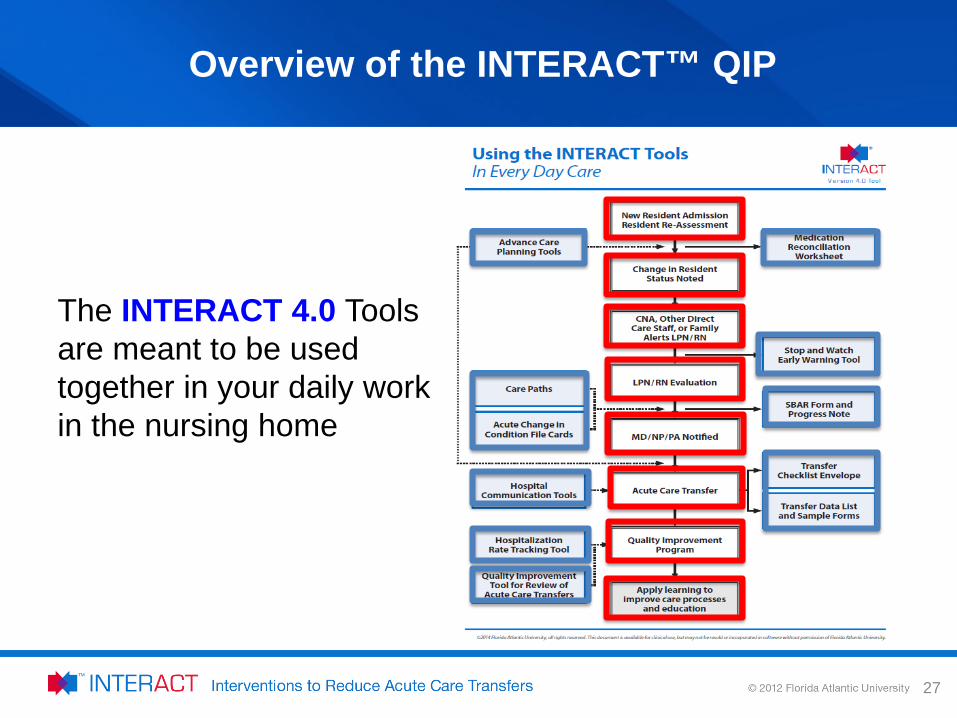
Overview of the INTERACT™ QIP
The INTERACT 4.0 Tools are meant to be used together in your daily work in the nursing home
27

ADVANCED CARE PLANNING TOOLS
28

Advanced Care Planning Tools-Examples
29

COMMUNICATION TOOLS
30
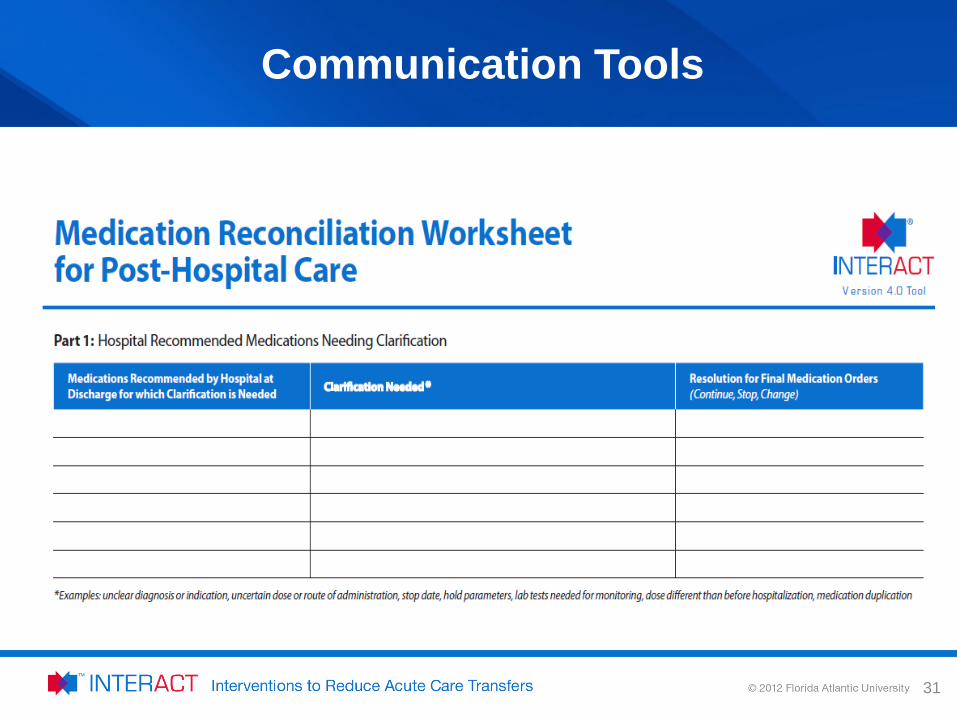
Communication Tools
31
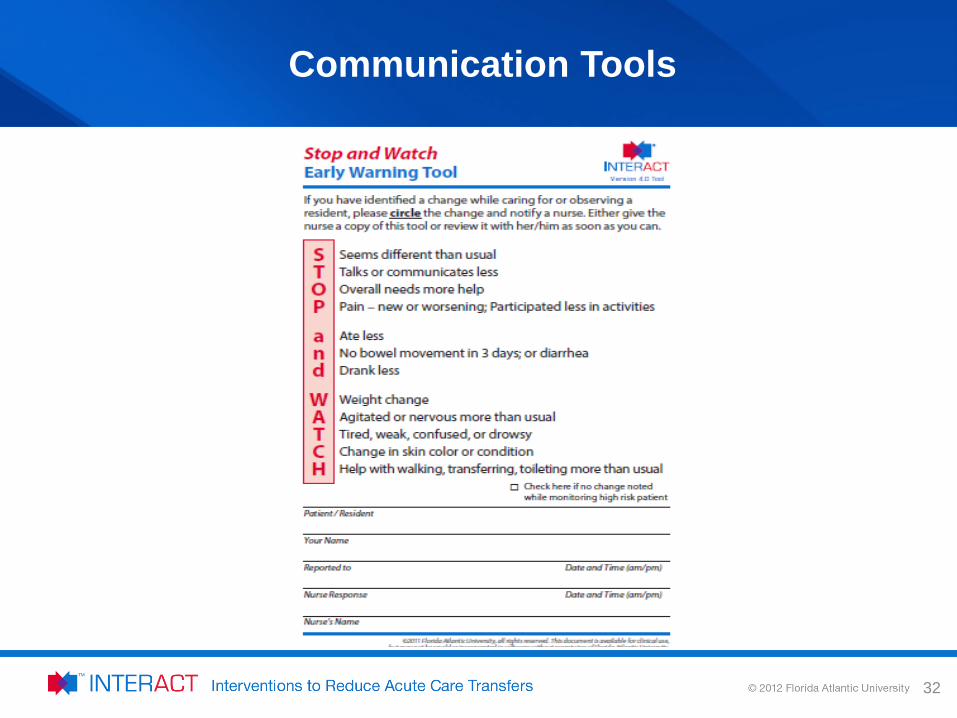
Communication Tools
32
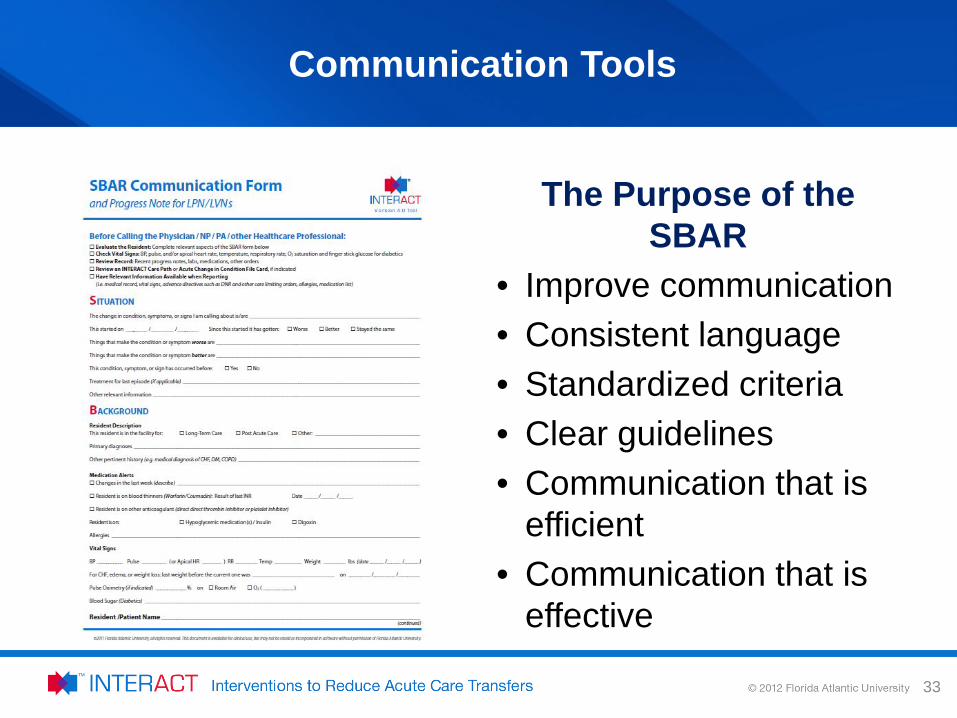
The Purpose of the SBAR
• Improve communication • Consistent language • Standardized criteria • Clear guidelines • Communication that is
efficient • Communication that is
effective
33
Communication Tools
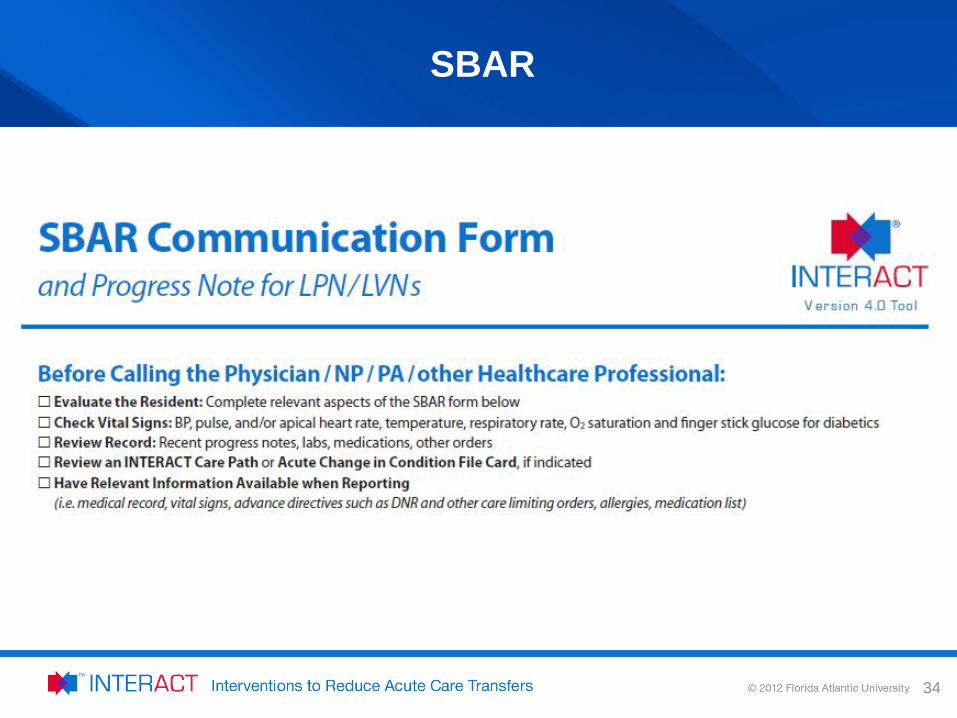
SBAR
34

DECISION SUPPORT
INTERACT™ 4.0 Quality Improvement Program
35
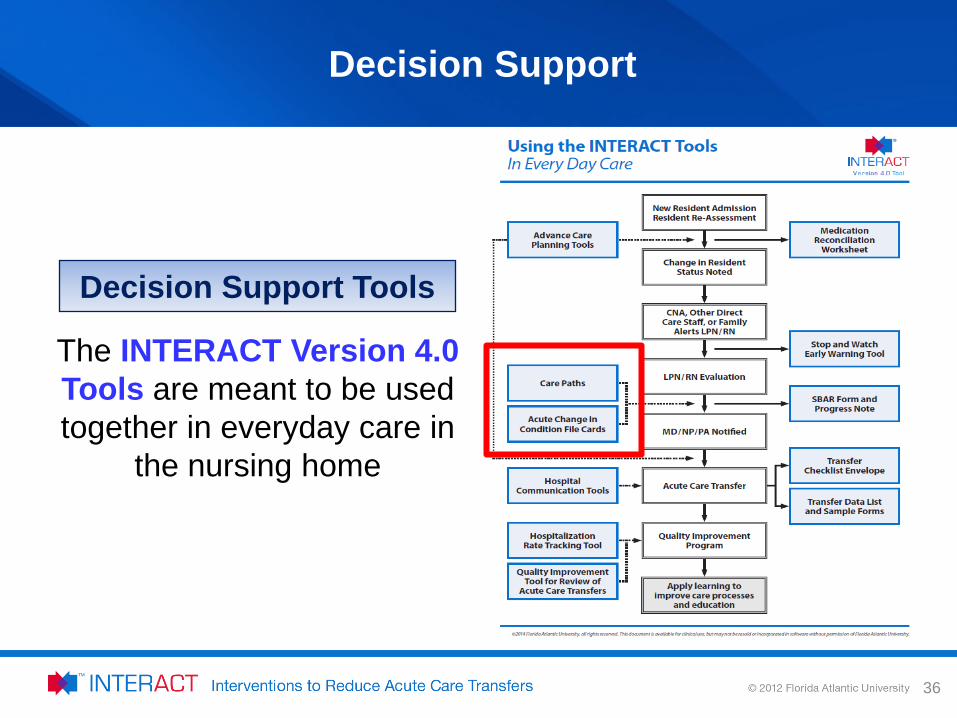
Decision Support Tools
The INTERACT Version 4.0 Tools are meant to be used together in everyday care in
the nursing home
Decision Support
36
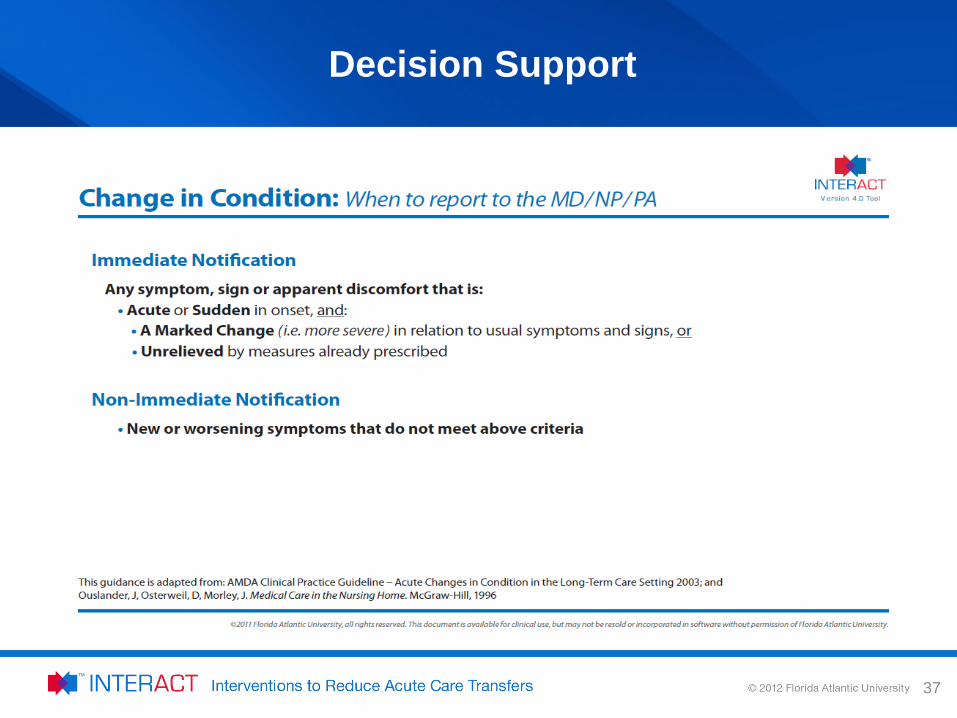
Decision Support
37
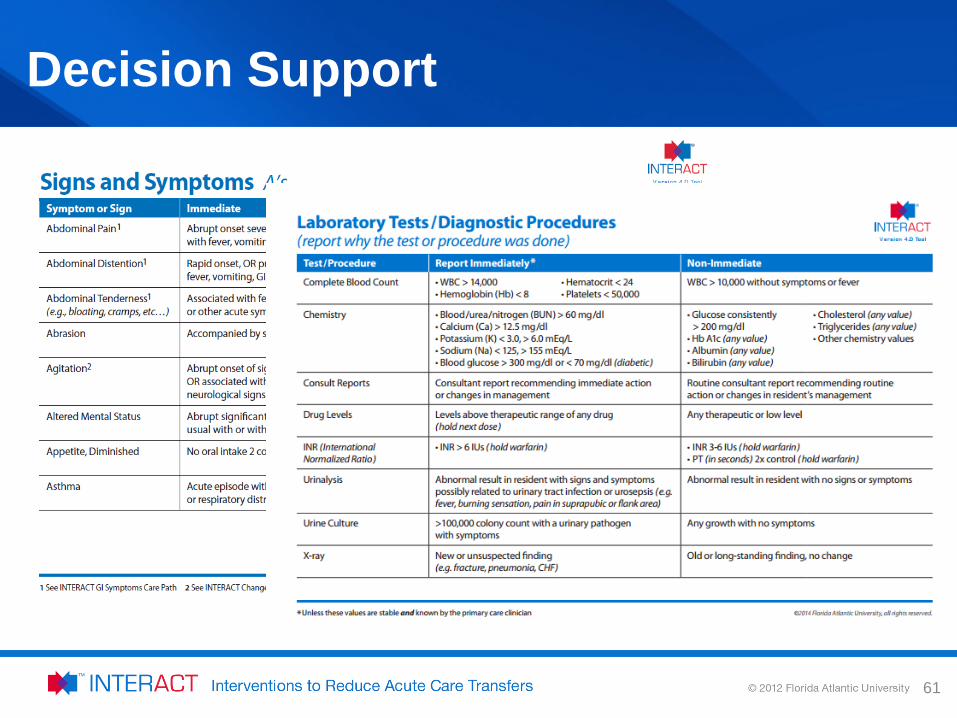
Decision Support
61
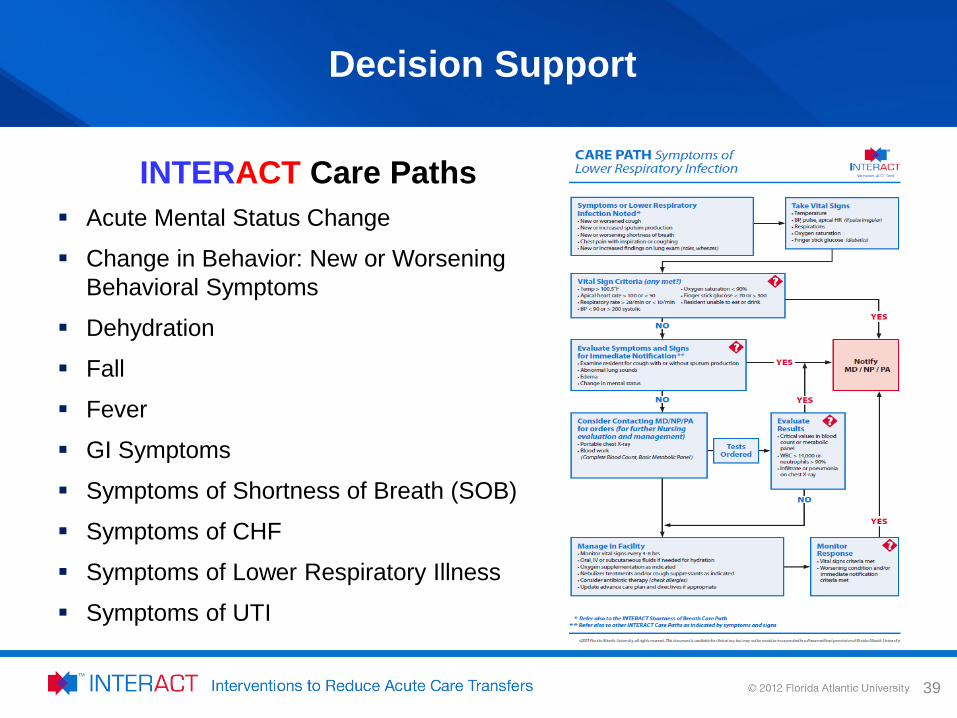
Decision Support
INTERACT Care Paths Acute Mental Status Change
Change in Behavior: New or Worsening Behavioral Symptoms
Dehydration
Fall
Fever
GI Symptoms
Symptoms of Shortness of Breath (SOB)
Symptoms of CHF
Symptoms of Lower Respiratory Illness
Symptoms of UTI
39
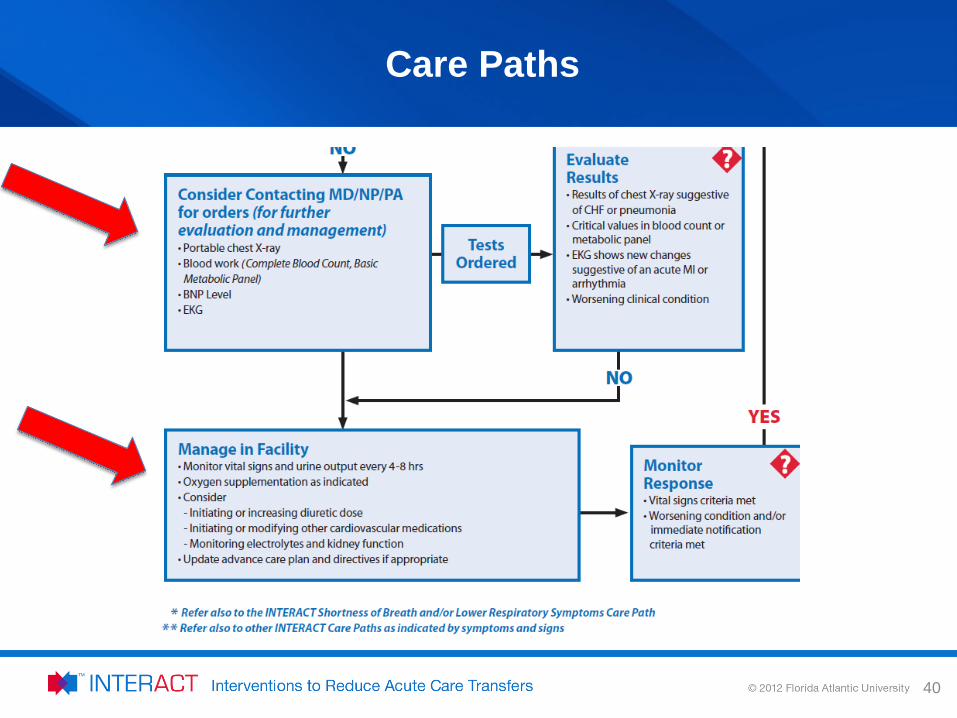
Care Paths
40
ADDITIONAL COMMUNICATION TOOLS
Using the Tools
41
42
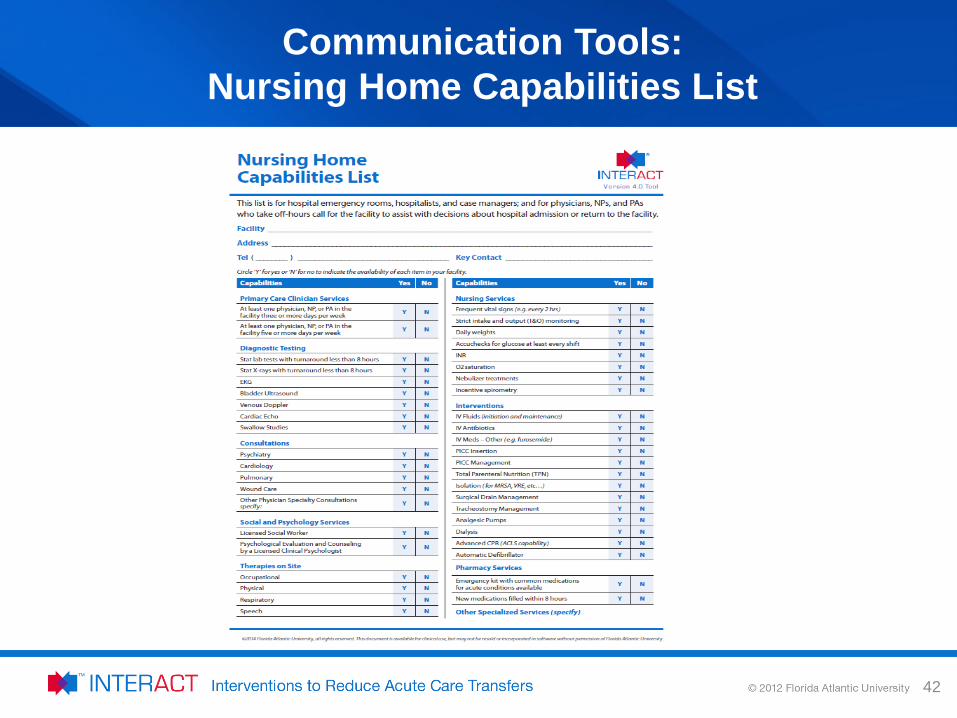
Communication Tools: Nursing Home Capabilities List
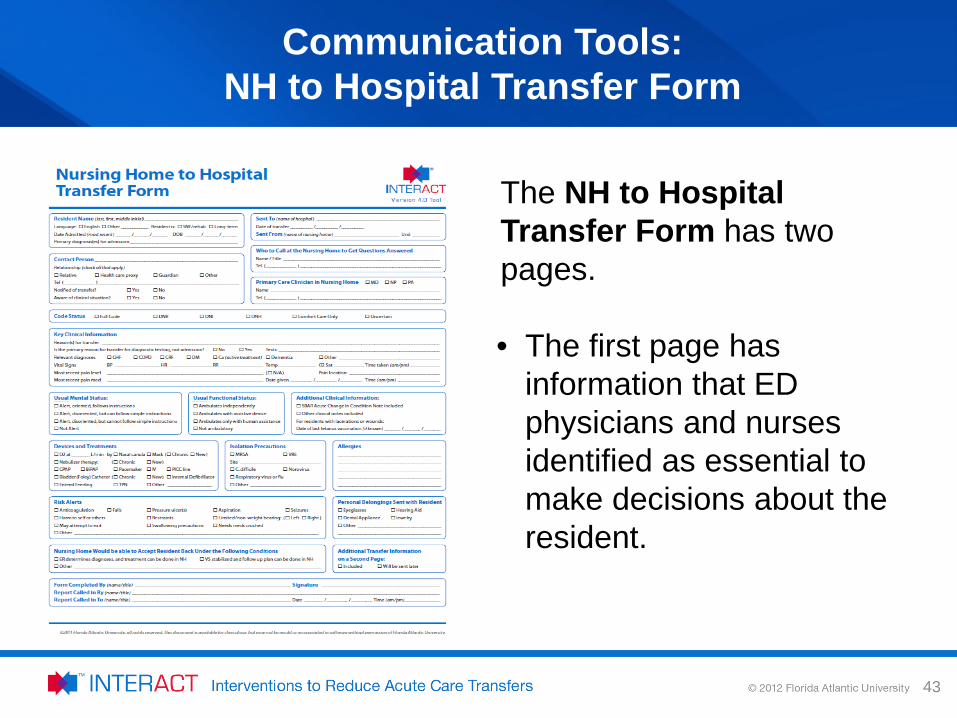
The NH to Hospital Transfer Form has two pages. • The first page has
information that ED physicians and nurses identified as essential to make decisions about the resident.
43
Communication Tools: NH to Hospital Transfer Form
QUALITY IMPROVEMENT TOOLS
44
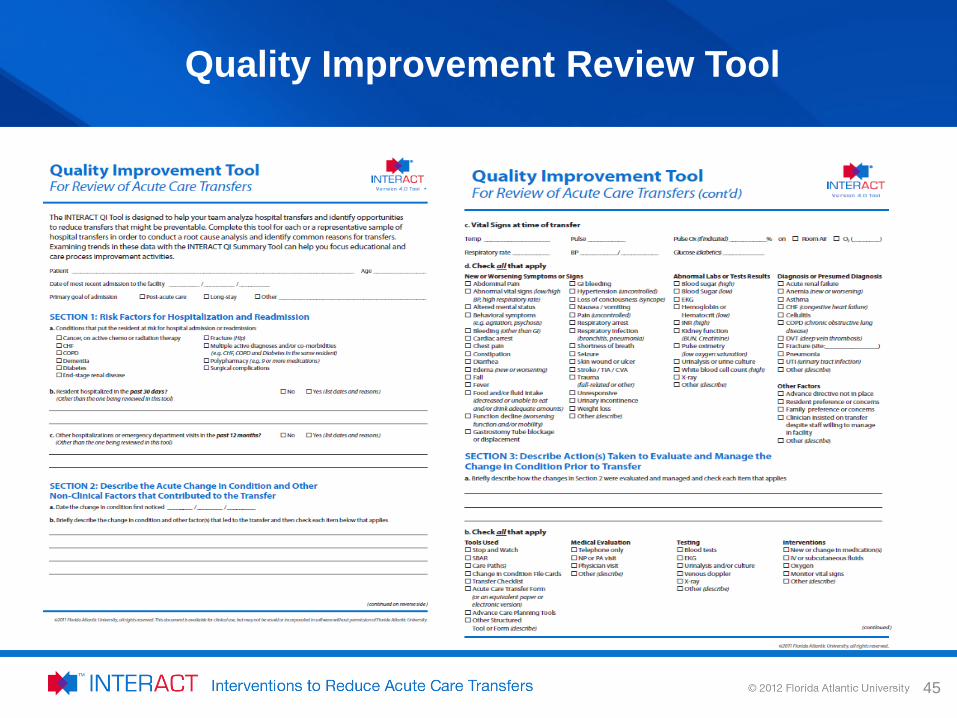
Quality Improvement Review Tool
45
Key Resource
46
http://interact.fau.edu/docs/INTERACT%20Version%204.0%20Tools/INTERACT%20V4%20Implementation_Guide%20Dec%2010.pdf

PREPARE . PLAN . IMPLEMENT Next Steps
47
Prepare
• Assess Organization Systems – Corporate Programs and Outcomes – Facility specific protocols
• Assess need to change • Benchmark internal systems for review
– Current status – Industry standards – Best practice approach
• Identify opportunities
48
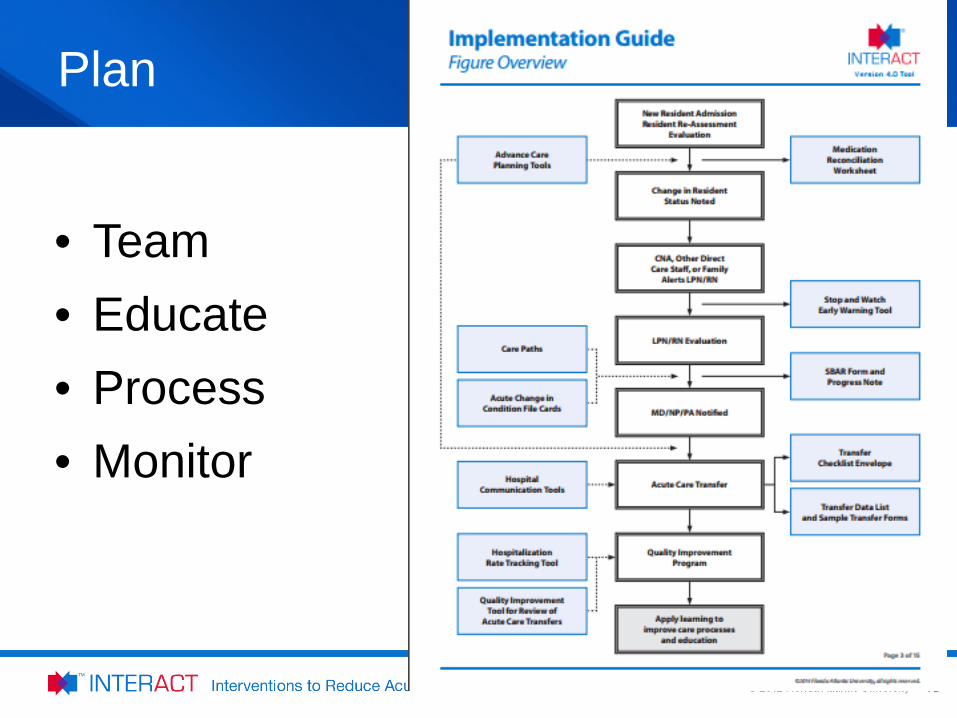
Plan
49
• Team • Educate • Process • Monitor
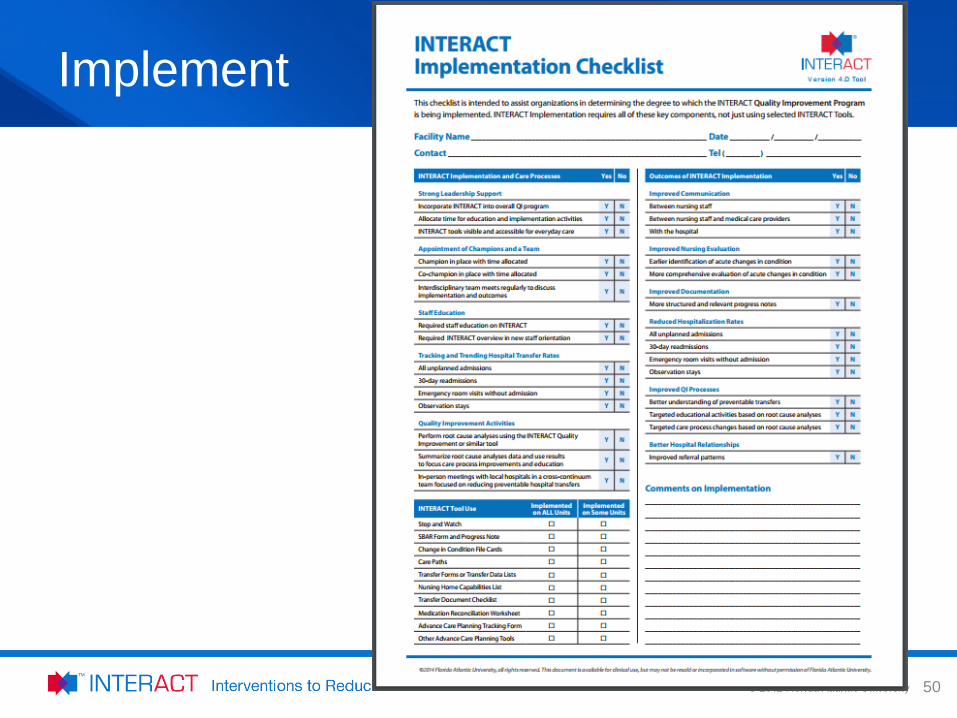
Implement
50
INTERACT Website
Tools, Resources and Information:
http://www.pathway-interact.com/
51
Questions?
52
Thank You!
Lisa Thomson and Sue LaGrange Certified INTERACT Master Trainers
Pathway Health
53
Recommended

















