Topical Session 01
HIDDEN DRIVERS OF PAIN: PSYCHOLOGICAL / PSYCHIATRIC
PERSPECTIVES
CARL GRAHAM
Fremantle Hospital, WA
NEWMAN L. HARRIS Royal North Shore Hospital, NSW

THIS PRESENTATION MAY MAKE REFERENCE TO SOME “OFF-LABEL” USES OF MEDICATIONS WHICH ARE
INCLUDED ONLY FOR ACADEMIC COMPLETENESS.
ATTENDEES SHOULD NOT INFER ANY ENCOURAGEMENT TO BREECH PRESCRIBING REGULATIONS.

DISCLOSURES
Speakers Bureau• Boehringer Ingelheim • Eli Lilly• GlaxoSmithKline• Medtronics• Pfizer• Solvay• Wyeth
Advisory Boards• Boehringer Ingelheim • Eli Lilly• Pfizer
Conference Sponsorship• Boehringer Ingelheim • Eli Lilly• GlaxoSmithKline• Pfizer• Wyeth

What about the 10% who cost us 90% -

What about the 10% who cost us 90% - Another hedgehog
maybe?

Return to Work After Lumbar Return to Work After Lumbar Discectomy (Discectomy (Schade et al 1999Schade et al 1999) )
• Correlates with depression and workplace stress,
• not with indices of organicity.

Biopsychosocial considerationBiopsychosocial consideration
Parsons (1951) – The Sick RoleMechanic (1961) – Illness BehaviourPilowsky (1969) - Abnormal Illness
BehaviourEngel (1977) – “Biopsychosocial”

WHAT IS PAIN ?WHAT IS PAIN ?• “An unpleasant sensory or emotional
experience associated with actual or potential tissue damage, or described in terms of such damage.” (IASP 1979)
• Pain is always subjective• Definition doesn’t tie pain to a stimulus• Nociception is NOT equivalent to pain

The Multidisciplinary Approach The Multidisciplinary Approach (Presley and Cousins 1992)(Presley and Cousins 1992)
• Holistic biopsychosocial assessment• Rationalised organic treatment plan• Psychological and social interventions
A paradigm shift from traditional medical approach is required.

INTERACTIONS WITH ENVIRONMENT
PAIN BEHAVIOURS
SUFFERING
COGNITIONS ATTITUDES
BELIEFS
PAIN PERCEPTION
NOCICEPTION NEUROPATHY
Fordyce and Loeser’sformulation

Descending Pathway
AscendingPathway
DescendingPathway

Dr M K Nicholas, PM&RC

Psychiatric Disorder in the Psychiatric Disorder in the Pain ClinicPain Clinic
• 90% of pain clinic attendees suffer at least one psychiatric disorder (Large 1980)
• Over 60% satisfy criteria for more than one (Fishbain et al 1986)

Psychiatric Disorder in the Psychiatric Disorder in the Pain ClinicPain Clinic
• Anxiety Disorders• Depression• Somatoform Disorders• Substance Problems• Psychotic Illness

Comorbid Mood Disorder in Primary Comorbid Mood Disorder in Primary Care Setting :Care Setting :
–34% of Joint & Limb Pain–38% of Back Pain–40% of Headache–46% of Chest pain –43% of Abdo Pain
Kroenke & Price 1993

DepressionDepression
–Higher levels of pain reported–More pronounced pain
behaviour–Pain settles with Rx of mood–Depression implicated in
transition to chronicity along with somatisation & distress

Risk of Suicide in Depression Risk of Suicide in Depression & Chronic Abdominal Pain& Chronic Abdominal Pain
0%
10%
20%
30%
40%
50%
60%
No Pain orDepression
(n=3941)
Pain, NoDepression
(n=189)
Depression, NoPain (n=734)
Pain andDepression
(n=100)
Wanting to Die Suicidal Ideation Suicide Attempt
Magni et al. Pain 1998.


Yellow FlagsYellow Flags• Attitudes and Beliefs• • Belief that pain is harmful or disabling resulting in fear-
avoidance behaviour• • Belief all pain must be abolished before return to work or
normal activity• • Catastrophising, thinking the worst, misinterpreting bodily
symptoms
• Behaviours• • Use of extended rest, disproportionate downtime • • Reduced activity, significant withdrawal from activities of daily
living• • Report of extremely high intensity of pain on VAS• • Sleep quality reduced since onset of back pain
• https://www.cebp.nl/media/m24.pdf

Yellow FlagsYellow Flags• Compensation Issues• • Lack of financial incentive to return to work• • Delay in accessing income support and treatment cost,
disputes over eligibility• • History of extended time off work due to injury or other pain
problem
• Diagnosis and Treatment• • Experience of conflicting diagnoses or explanations for back
pain• • Dramatisation of back pain by HP's, dependency on
treatments, passive treatment• • Expectation of a techno-fix, eg, requests to treat as if body
were a machine • https://www.cebp.nl/media/m24.pdf

Yellow FlagsYellow Flags• Emotions• • Fear of increased pain with activity or work• • Depression (especially long-term low mood), loss of sense of enjoyment• • Anxiety about and heightened awareness of body sensations (includes
sympathetic nervous system arousal)• • Feeling under stress and unable to maintain sense of control
• Family• • Over-protective or solicitous partner, emphasising fear of harm or
catastrophising• • Socially punitive responses from spouse (eg ignoring, expressing frustration)• • Extent to which family members support any attempt to return to work• • Lack of support person to talk to about problems
• https://www.cebp.nl/media/m24.pdf

Yellow FlagsYellow Flags
• Work• • Frequent job changes, stress at work, job dissatisfaction, • • Poor relationships with peers or supervisors...• • Belief that work is harmful; that it will do damage or be dangerous• • Unsupportive or unhappy current work environment
•
• https://www.cebp.nl/media/m24.pdf

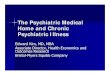
Yellow FlagsYellow FlagsWhy would psychosocial variables influence pain and disability?
• Catastrophising directly influences pain intensity & pain-related disability (Turner, et al (2002) Pain; 98, 127-134)
• Psychological or social variables which function as threats, or are experienced as a loss of control, access standard sickness responses resulting in increased inflammation (Brydon, et al (2009)Brain, Behavior & Immunity 23; 217-224)
• Inflammatory proteins can have an exacerbatory role in pain (Wieseler-Frank, Maier, Watkins (2005) Neurosignals;14:166–174)
• Cycle - Cognitive & emotional responses during the experience of pain shaped pro-inflammatory immune system responses via interleukin-6 (Edwards, et al (2008) Pain; 140, 135-144)

4/10/10 Mayer, et al 2009
6 wee
ks
3 m
onth
s
6 m
onth
s
9 m
onth
s
1 ye
ar
Cum
ulat
ive
prob
abili
ty o
fre
mai
ning
unr
ecov
ered
0.2
0.4
0.6
0.8
1.0
4 yellow flags3 yellow flags2 yellow flags1 yellow flags0 yellow flags
5 yellow flags
6 yellow flags

Remaining at Work
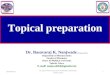
20 public health workers at risk for developing chronic pain (taking sick days for pain probs)
10 TAU vs 10 CBT (4 x 1 hrs ACT)
Dahl, Nilsson & Wilson, Behavior Therapy, 2004Dahl, Nilsson & Wilson, Behavior Therapy, 2004

Cumulative Sick Leave
0
10
20
30
40
50
60
70
80
BL mo 1
BL mo 3
BL mo 5
Inte
rven
tion
FU mo 2
FU mo 4
FU mo 6
Ave
rag
e T
ota
l # S
ick
Day
s
ACT
TAU
Cohen’s d at follow-up =
1.00

Case 1: Case 1: TIM 44 y.o. software geniusTIM 44 y.o. software genius
•Referred by Rehabilitation Physician•In context of escalating workplace pressue, gradual onset of neck, bilat. shoulder and arm (RSI-like) pain•Pain began in context of escalating workplace stressors•Workplace critical / unsupportive•20 months on WorkCover

Over prior 18 months he had been off work, receiving
•1:1 physiotherapy input•1:1 exercise physiologist instruction•1:1 generalist psychology input

Investigations
•C. Spine MRI•Brain MRI •L Shoulder MRI•Bilat nerve conductions•Rheumatological screen•Bone scan

Reason for referral:
•Failure to progress:•Tolerances / capacities unchanged •Rigid pain focus entrenched

Findings of Team Assessment•Nil organic aetiology identified•Marked physical deconditioning•Exaggerated somatic preoccupation a/w
ritualised safety behaviours•High depression and anxiety scores•Marked obsessionality•Fear avoidance•Poor self efficacy•Oversolicitous partner•Substances - 2 different benzos, 2 OTC analgesics, 2 types anti-inflammatory & EtOH

Recommendations from Team Assessment
•Reassurance•Substance rationalisation•Self-help text “Manage Your Pain”•1:1 psychology and physiotherapy – •3 sessions of each over 6 weeks

Progress
Liked the book – he understood and felt inspired – but couldn’t progress
Psychiatric assessment requested.

Psychiatry assessment
• Ritualised safety behaviours – gyration of shoulder girdles multiple pillows / braces
• Melancholia (EMW, anhedonia, ruminations, low energy, cognitive poor, anorexia)
• Controlling / demanding / obsessional• 2 different benzos, 2 OTC analgesics, 2 types
anti-inflammatory• 60 g EtoH

What next?
• Education re integrated activity of limbic and other brain centres with pain circuitry
• Discussion re neuroplastic exacerbatory processes
• Discouraged benzos• Offered SNRI - declined• Pregabalin commenced

Case 2 : SomatisationCase 2 : Somatisation
• Long history of complaints• High utilisers of health services• Biomedical focus• Excessive illness behaviour c.f. pathology
• Outcome issues - poor prognosis

Is chronic pain associated with Is chronic pain associated with somatization/hypochondriasissomatization/hypochondriasis
. • An evidence-based structured review (57
studies)• Somatisation and hypochondriasis were both
consistently associated with chronic pain • Study evidence indicated a correlation
between pain intensity and presence of somatisation and hypochondriasis
• Pain treatment improved somatisation and hypochondriasis
Fishbain et al. Pain Pract. 2009 Nov-Dec;9(6):449-67

Case 2 : Pam 62 yo
• Referred by Pain Specialist
• Multiple morbidities including OA in hips, hands, neck and low back, haemochromatosis, osteoporosis (with compression fractures x2), macular degeneration, chronic constipation, stress incontinence, hypertension.
• Slim and frail-looking

- Powerful biomedical focus- Multiple practitioners – 2-3 specialists /12

• Morphine sulphate SR 20 mg bd• “Digesic” • Diazepam 2.5 – 5 mg up to qid• Aperients• Nutritional supplements
• Procedures / “blocks” every 6-12 weeks

Reason for referral:
• Assistance sought with her distress - as demonstrated through her seeking of advice and reassurance via frequent phone calls (2-3 per week)

Background
• Younger of two daughters from wealthy family
• Sickly child – multiple hospitalisations for asthma
• Father was caring but busy• Mother was just busy• Teen years: Sister strong, successful and
popular. Pam polite, unassertive, “a worrier”

Lots to worry about :
• Three adult offspring – 2 unwell (1 Alcoholic)• 1 son-in-law unwell (Colitis)• Seven grandchildren• Very aging mother• Fit but aging husband
….and of course herself too!

Case 3 : Brian 48 yo SurveyorCase 3 : Brian 48 yo Surveyor• Previously fit, very active professional man• Actively involved with church• Perfect family • Perfectionist
• MBA 3 years ago• Multiple orthopaedic (and visceral) injuries• 6 weeks in hospital and 5 operations• 8 weeks inpatient rehabilitation

Inpatient treatment
• Decompression/fusion L2/3• ORIF R. tibia/fibula• ORIF R. humerus• ORIF L. radius (distal)• Repair hepatic laceration and bladder/ureter
damage

Complaints• Pain distracts him – can’t stop ruminating about
pain and the idiot who caused it• Cranky• Impaired workplace function
• Exacerbation of (premorbid trait of) relative inflexibility.
• Had become intolerant• Always tired• Memory impaired

Reason for Referral
• Referred due to persistent pain (and his responses to it) causing disruption to interpersonal and workplace function –fear of losing job.

Assessment findings
• Team assessment identified nociceptive and neuropathic drivers, obsessional personality, excess pain focus, all-or-none behaviour
• Self damning / catastrophic cognitions• Physical deconditioning

• Not happy to take medication, fearing further compromise.
• Unable to obtain benefit from 1:1 CBT - Couldn’t focus- Too busy ruminating / distracting- Too sleepy- Neither time nor energy for
behavioural tasks

Progress
• Brain MRI NAD ; neuropsych testing equivocal for ABI.
• Agreed to trial Nortriptilline 10 mg – unable to tolerate – sleep better BUT daytime compromise and exacerbated hesitancy
• Not making progress after 6 sessions Clin. Psych plus physio. instruction

• Problems inherent with a big C approach to CBT
• Don't give more verbal rules to perfectionists!
• Behavioural change not enhanced significantly by cognitive intervention
Jacobson, et al (2000) Journal of Consulting & Clinical Psychology; 64, 2, 295-304
Longmore, Worrell (2007) Clinical Psychology Review 27; 173-187
Dimidjian, et al(2006) Journal of Consulting & Clinical Psychology; 74, 4, 658-670

Recommended