Topical drug delivery• Skin anatomy
• Functions of skin
• Five main target regions in dermatological therapy
• Sunscreen on skin surface
• Acne to target hair follicles and pilosebaceous unites
• Delivery of macromolecules via the hair follicles
• Contact dermatitis and viable epidermis and dermis

Skin anatomy• Epidermis --0.8 to 0.006 mm. --stratum corneum: 10 m when dry, horny
layer (10-20% moisture)
• Dermis --3-5 mm --a matrix of connective tissues woven fibrous
proteins --Nerves, blood vessels (< 0.2 mm deep),
lymphatics
• Subcutaneous tissue --mechanical cushion, thermal barrier, energy
storage
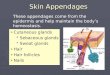
• Appendages --Sweat glands --hair follicles --Sebaceous glands --Nails

Functions of skin
• Mechanical function -- mainly from the dermis and s.c. tissues -- epidermis (minor) • Protective function -- Microbiological barrier -- Chemical barrier -- Radiation barrier -- Heat barrier/temperature regulation -- Immune response


Stages on percutaneous absorption from a suspension ointment

Five main target regions in dermatology
• Surface treatment -- Camouflage, protective layer, insect repellent,
antimicrobial/antifungal, Sunscreen• Stratum corneum -- Emollient, keratosis• Skin appendage -- Acne, antibiotics, depilatory, antiperspirant, vaccine• Viable epidermis/dermis -- antiinflammation, anesthetics, antihistamine,
antipruritic• Systemic treatment -- transdermal

Sunlight, sunscreen, suntan
UVA: suntan, and PUVA treatment of psoriasis (psoralen + UVA),
photosensitivity, photoaging, photodermatoses, and augment cancerous effects of UVB.
UVB: Vitamin D synthesis
Cause sunburn, skin cancers
UVC

UV spectrum
Factors affecting exposure to UVR
Time of the day, Altitude, environmental factors, and predisposed factors.

Suntan and sunburn• Sun tanning: a result of two processes -- Oxidation of melanin/immediate darkening -- Stimulation of melanocytes/delayed tanning Tanning increases tolerance to additional sun light.
• Sunburn: a superficial burn involving the epidermis.
-- Normal sequence -- Erythema, 20-30 min, oxidation of melanin and dilation of dermal
venules -- True sunburn erythema, 2-8 h -- Localized edema and pain, 14-20 h, last 1-3 days
• Other reactions to UVR -- actinic keratosis, squamous cell carcinoma, basal cell carcinoma,
melanoma.

Sunscreen agents• SPF: Minimal, 2-12; Moderate, 12-30
high, > 30
SPF is the minimal erythema dose (MED) of protected skin over the MED of unprotected skin. MED is the amount of solar radiation needed to produce minimal skin redness.
• Types of sunscreens Physical sun blockers Titanium dioxide, Zinc oxide, Red
petrolatum
Chemical sun absorbers (1) PABA (2) Cinnamates (3) Salicylates (4) Benzophenones (5) Avobenzone (Parsol 1789)
Physical blockers are opaque formulations that reflect and scatter up to 99% of light in both VR and vis ranges.
Less cosmetically acceptable/greasy.
Sunscreens just need to bind and remain on the skin for sufficient time.


Dihydroxyacetone (DHA)
ErythruloseCoppertone
DHA is a chemical agent that darkens the skin by reacting with keratin in the stratum corneum to produce artificial suntan. It provides no protection against UV rays, and may not be natural looking. The Eryhtrulose is also in some products. It can be in lotion, gel, spray, solution, etc.

Acne• Acne vulgaris is a disorder of the pilosebaceous units.• A plug of the pilosebaceous duct and follicle opening. • Drugs have to get into the hair follicles and pilosabaceous units
http://www.skincarephysicians.com/acnenet/acne.html


Etiology• Increased sebum production Androgens regulate sebum production. Testosterone converted to DHT,
which induces sebaceous glands to increase in size and activity, resulting in
increased amount of sebum. • Abnormal clumping of epithelial horny cells in
the pilosebaceous unit Horny cells usually sloughed off from epithelial lining of the pilosebaceous
duct. Retention hyperkeratosis (increased adherence and production of follicular
epithelial cells)
• Presence of Propionibacterium acnes P. acnes lipases break triglyceride to fatty acids, which are irritating, cause
comedones, and result in inflammation.

Assessment of acne severity
Grade Qualitative description Quantitative description
I Comedonal acne Comedones only, < 10 on face, none on trunk, no scars, non-inflammatory lesion
II Papular 10-25 papules, mild scarring, inflammatory lessoin (< 5 mm)
III Pustule 25 pustules, moderate scarring
IV Pustulocytic acne Nodules or cysts, extensive scarring, inflammatory lessions . 5 mm.
Cytic acne Extensive nodule/cysts
Self treatment with OTC agents is only OK for grade I.

Approaches for treatment
• Increased sebum production
Testosterone converted to DHT, which induces sebaceous glands size and activity.
• Abnormal clumping of epithelial horny cells in the pilosebaceous unitRetenion hyperkeratosis
• Presence of Propionibacterium acnes
P. acnes lipases break triglyceride to fatty acids, which are irritating, causing comedones.
Decreasing the amount of sebum produced
Unblocking the sebaceous ducts
Kill the bacteria

OTC acne product• Benzoyl peroxide -- 2.5% to 10% -- Most effective OTC -- Kill P. acnes and irritant to increase epithelial cell
turnover rate. -- gel, cream, or lotion• Salicylic acid -- 0.5-2%, irritant keratolytic agent, lotion, creams• Sulfur, 3-8% combined with resorcinol 2%, or resorcinol
monacetate 3%. keratolytic and antibacteria, color/odor• Resorcinol -- 1-4%, keratolytic when combined with sulfur

Prescription• Tretinoin (retin-A): • increase the turnover rate of
nonadhering horny cells in follicles.• Cream, gel, topical solution• More effective agent for acne• Increase hair growth
• Others: Adapalene (Differin), Tazarotene gel and cream (Tazorac), antibiotics (tetracyline, erythromycin, clindamycin, etc)
• Isotretinoin (Accutane)• For severe racalcitrant nodulocytic
acnes• Decrease sebum and keratinization• Reduce population of P. acnes• Birth defect

Tretinoin is very effective

Hair follicular cycle
Human: Normally up to 90% of the hair follicles are in anagen phase while, 10–14% are in telogen and 1–2% in catagen.
Rodent: hair follicles are synchronized in the first two cycles.

Hair follicles as a route for drug/vaccine delivery

Macromolecules access skin via hair follicles

Contact dermatitis:Inflammation of the skin
Irritant contact dermatitis
Caused by direct contact with the irritant Absolute primary irritants: acids, alkalis, industrial chemicals, Relative primary irritants: soaps, detergent, benzoyl peroxide, etc)
Allergic contact dermatitis: The result of direct contact with a contact allergen, such as poison
ivy and nickel. Allergic contact dermatitis is considered a T-cell mediated delayed-response immune reaction, because elicitation of an allergic reaction typically takes 48 to 72 hours to occur after reexposure to the same allergen.

Allergic contact dermatitis1. Hapten contacts skin
epidermis
2. Hapten complexes with protein
3. Hapten-protein enters lymphatic systems
4. Generation of specific Th1 CD4+ and CD8+ T cells.
5. Re-exposure
6. Dermatitis responses
Urushiol from poison ivy, poison oak, and sumac.
Hapten = small molecules that are only antigenic when combined with a carrier protein.
http://www.poison-ivy.org/

Treatments
• Severe eruptions: systemic corticosteriods
• Less severe eruptions:
Relieve itching Local anesthetics (benzocaine)
Antihistamines (oral or topical, mainly sedative effect)
Topical hydrocortisone
Treatment Topical hydrocortisone.

Topical corticosteriod preparations

Some brand names of hydrocortisone
Recommended