
11/21/2016
1
Identifying and managing cognitive
and behavioral effects of CNS
cancers
Michael Feuerstein, PhD, MPHMiami Neuro Nursing Symposium
Baptist Health Neuroscience Center
December 1-3, 2016
The Biltmore Hotel
Coral Gables, Florida
Speaker Disclosure
There are no relevant commercial
relationships to disclose
M. Feuerstein, PhD., MPH
Learning Goals
• Major cognitive problems, clinical correlates and bio-behavioral mechanisms in prevalent CNS cancers
• Approaches used to assess cognitive problems and distress in CNS cancer survivors
• Interventions to manage cognitive problems in CNS cancer survivors

11/21/2016
2
Long term and late effects Brain Tumors
• Sensory – Hearing
– Sight
– Taste
• Fatigue
• Depression/Anxiety/Fear
• Health Behavior changes (activity, diet, weight gain, smoking)
• Work
• Financial strain
• Health seeking skills (health care literacy)
• Co-morbidity
Caregiver Concerns Brain Tumors
Cognitive Problems BT Survivors
Cognitive processing speed
Attention
Cognitive control and flexibility
Organization
Verbal learning
Working memory
Planning and foresight
Gerke, et al. J. Neurooncology, 2013

11/21/2016
3
Cog Impairment Healthy Older AdultsCNS Meds
N=2737
Biobehavioral Plausability
• Brain slower
• Brain works
harder
Clinical Assessment
• Cognitive Function – Neuropsych testing
• https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4356068/pdf/fonc-05-00056.pdf
– Patient-Reported Outcomes (PROMISE)• https://commonfund.nih.gov/promis/index
– Cognitive challenges at work (CSC Work)• https://www.ncbi.nlm.nih.gov/pubmed/24270293
• Distress – Distress Thermometer (DT)
• https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4585197/pdf/fonc-05-00203.pdf
• Unmet needs- Post Treatment
– Cancer Survivor Profile (CSPro)
• https://www.ncbi.nlm.nih.gov/pubmed/25820913
11/21/2016
4
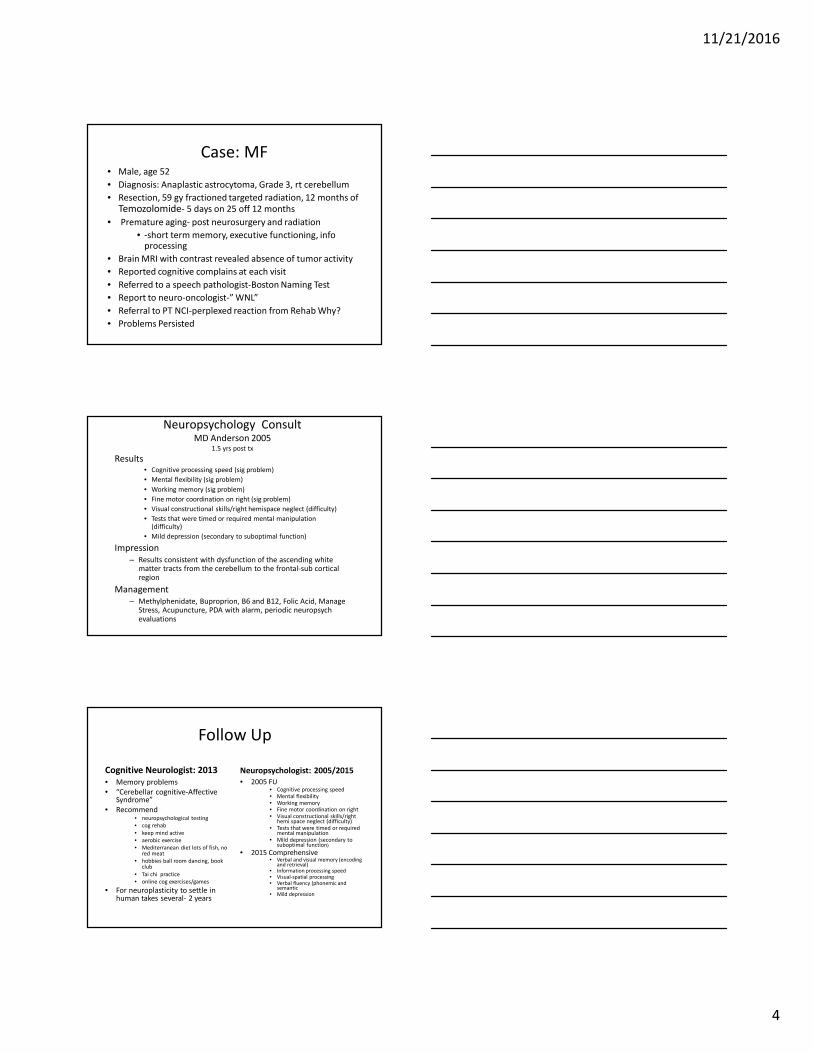
Case: MF• Male, age 52
• Diagnosis: Anaplastic astrocytoma, Grade 3, rt cerebellum
• Resection, 59 gy fractioned targeted radiation, 12 months of
Temozolomide- 5 days on 25 off 12 months
• Premature aging- post neurosurgery and radiation
• -short term memory, executive functioning, info processing
• Brain MRI with contrast revealed absence of tumor activity
• Reported cognitive complains at each visit
• Referred to a speech pathologist-Boston Naming Test
• Report to neuro-oncologist-” WNL”
• Referral to PT NCI-perplexed reaction from Rehab Why?
• Problems Persisted
Neuropsychology ConsultMD Anderson 2005
1.5 yrs post tx
Results • Cognitive processing speed (sig problem)
• Mental flexibility (sig problem)
• Working memory (sig problem)
• Fine motor coordination on right (sig problem)
• Visual constructional skills/right hemispace neglect (difficulty)
• Tests that were timed or required mental manipulation (difficulty)
• Mild depression (secondary to suboptimal function)
Impression
– Results consistent with dysfunction of the ascending white matter tracts from the cerebellum to the frontal-sub cortical region
Management
– Methylphenidate, Buproprion, B6 and B12, Folic Acid, Manage Stress, Acupuncture, PDA with alarm, periodic neuropsychevaluations
Follow Up
Cognitive Neurologist: 2013
• Memory problems
• “Cerebellar cognitive-Affective Syndrome”
• Recommend • neuropsychological testing
• cog rehab
• keep mind active
• aerobic exercise
• Mediterranean diet lots of fish, no red meat
• hobbies ball room dancing, book club
• Tai chi practice
• online cog exercises/games
• For neuroplasticity to settle in human takes several- 2 years
Neuropsychologist: 2005/2015
• 2005 FU• Cognitive processing speed • Mental flexibility • Working memory • Fine motor coordination on right• Visual constructional skills/right
hemi space neglect (difficulty)• Tests that were timed or required
mental manipulation• Mild depression (secondary to
suboptimal function)
• 2015 Comprehensive• Verbal and visual memory (encoding
and retrieval)• Information processing speed• Visual-spatial processing• Verbal fluency (phonemic and
semantic • Mild depression

11/21/2016
5
“
Female Marine’s Story “Golf-ball-sized brain tumor called an astrocytoma”
Brain surgery Sept. 25, 2006. Left leg was paralyzed from the surgery. Given a walker
released from hospital after five days. Highly motivated to recover, used walker right
away upon arriving home. Walking on her own by Thanksgiving. April 2007, started
taking Temodar. Temporary Disability Retired List for five years. Was angry and
devastated . Never thought this would happen.
Eventually began seeing a counselor who helped her deal with her emotions. June 1,
2007, medically retired. Later in June, family moved back to Virginia her husband had
been transferred there. Over the next few years, received an MRI every three months.
The tumor had shrunk even more due to the radiation and chemotherapy, and while it
was still there, it was at least stable.
Pregnant with second child, husband walked out. Moved in with parents then into
her own house. Started working part-time at a bridal shop supplement her retirement
pay. Toward end of her five-year retirement, decided she wanted to come back on
active duty. Her tumor was stable, feeling healthy. March 2013, re-enlisted. Assigned
to Basic School so she could stay in the area where her family and support system
were located. Promoted to sergeant in January 2014.
Cognitive Problems
BT Survivors
Cognitive processing speed
Attention
Cognitive control and flexibility
Organization
Verbal learning
Working memory
Planning and foresight
Gerke, et al. J. Neurooncology, 2013
Typical Neuropsychological Evaluation
Brain Tumor
• Abstract Reasoning
• Memory
• Attention
• Language
• Verbal Perception
• Executive Functioning

11/21/2016
6
Cognitive Problems at Work
Ottati and Feuerstein
2013
Distress and Unmet Needs

11/21/2016
7
Intervention Options
• Symptom Management
– Pharma
– Non Pharma
• Cognitive Management
– Cog Rehab
– Pharma- assess continuously
– Compensatory strategies
– Lifestyle change
Cognitive Rehab
Back et al 2013
“Trial” of Cognitive Rehab
Back et al 2013

11/21/2016
8
Cognitive Rehab for Gliomas
Interventions
• Neuropsych training software
• Virtual reality and computer assisted cog rehab
• Computer exercises guided by neuropsychologist
• Holistic mnemonic training program
• Cognitive training, compensatory techniques, computerized homework
• Cognitive rehab, problem solving therapy, use of a memory notebook
Outcomes
• Memory, attention, visual
spatial function, language,
reasoning
• Sequential recall, verbal
recall
• Verbal and non verbal
memory
• Creativity
Bergo et al 2016
Exercise and Cognitive Function
Neuro-
Plasticity
K
o
n

11/21/2016
9
Transient PlasticityDraganski et al 2004
Work and Cancer Survivors
AccommodationsStergiou-Kita et al 2016
• 40 semi-structured interviews• cancer survivors=16
• Health/voc providers=16
• Employer=8
• Four types accommodations recommended
– Gradual return to work plans/flexible schedule
– Modification of work duties and expectations
– Retraining and supports at the workplace
– Modification of the physical work environment and/or adaptive aids/technologies
We need a new approach
• Conventional health care model
– Improve the cognitive abilities of the impaired
worker-
–“change to worker to fit the job”
• Public Health model
– Engineer the problem out of the workplace-
– “change the work to fit the person”

11/21/2016
10
Discrimination of Cognitive Demands in Breast Cancer and BT Survivors
Mathan et al., 2010, Conf Proc IEEE Eng Med Biol Soc
Detect and mitigate: Memory, Information Processing Speed, Executive Function,
Attention
Bottom Line: What does the research tell us ?

11/21/2016
11
Thank you
Recommended

















