Therapy ofInflammatory Bowel
Diseases2013
Gastroenterology Department
Division of Medicine
Eran Israeli MD

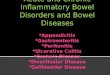
Cosnes J et al. Inflamm Bowel Dis 2002;8:244-50.
24022821620419218016815614413212010896847260483624120
0
20
40
60
80
100
%C
um
ula
tive
Pro
bab
ilit
y
Patients at riskMonths
2002 552 229 95 37N=
Penetrating
StricturingInflammatory
Long Term Evolution of Disease Behavior in CD

Goals of Treatment
Remission
Maintenance

Goals of therapy
Induce and maintain remissionAmeliorate symptomsImprove pts. quality of lifeAdequate nutritionPrevent complication of both the disease
and medicationsMucosal healing


Therapeutic PyramidTherapeutic Pyramidfor Active IBDfor Active IBD
SevereSevere
ModerateModerate
Aminosalicylates/AntibioticsAminosalicylates/Antibiotics
CorticosteroidsCorticosteroids
ImmunomodulatorsImmunomodulators
SurgerySurgery
InfliximabInfliximab
??((PrednisonePrednisone))
MildMild
((BudesonideBudesonide))

5-aminosalicylates
The mainstay treatment of mild to moderately active UC and CD (colitis).
5-ASA may act by blocking the production of prostaglandins and
leukotrienes, inhibiting bacterial peptide–induced
neutrophil chemotaxis and adenosine-induced secretion,
scavenging reactive oxygen metabolites

Sulphasalazine first agent discovered
Group now includes: Pentasa (mesalazine) Asacol (mesalazine) Rafassal (mesalazine) Salazopyrin-EN
(sulphasalazine) Work locally on the lining
of the gut to reduce inflammation
5-aminosalycylates

Highly effective for the induction of remission in patients with active disease
Short-term response rates (12–16 weeks) range from 70–90%
Not effective in maintenance of remission
Topical corticosteroids can be used as an alternative to 5-ASA in ulcerative proctitis or distal UC.
Corticosteroids
Enter cells and bind to and activate specific cytoplasmic receptors
Steroid-receptor dimers enter cell nucleusactivate steroid-responsive elements in DNA
Gene repression or induction anti-inflammatory effects
Anti-inflammatory effects take several hours

IV -for patients who are sufficiently ill to require hospitalization; the majority will have a response within 7 to 10 days
Budesonide: less side effects, its use is limited to patients with distal ileal and right-
sided colonic disease
Corticosteroids

Corticosteroids
-Acne“-Moon” face-Hair growth
“-Buffalo” hump
-Obesity-Purple / red streaks(striae)
-Bone thinning
-Bruising
-Muscle weakness
Cataract

Immunomodulators
Drugs include: Azathioprine 6-mercaptopurine Methotrexate
Interfere with inflammatory pathway Effective- up to 75% of patients brought into
remission Slow- optimal effect often not seen until after 12
weeks of treatment Need close monitoring for toxicity Safety- Methotrexate not to be used in pregnancy
• Inhibit ribonucleotide synthesis; • Induce T cell apoptosis by modulating cell )Rac1( signalling• Metabolised to mercaptopurine

Azathioprine
6-Mercaptopurine
6-TGN 6-MMPN
TPMT
Azathioprine Metabolism
TPMT = thiopurine methyltransferase6-TGN = 6-thioguanine nucleotide6-MMPN = 6-methylmercaptopurine ribonucleotide


TPMT Tested before initiating therapy Low TPMT activity related to high 6-TGN
levels, increasing risk of toxicity
6-TGN Used to monitor therapy Levels above 230 associated with better effect Levels above 480 associated with more side
effects

Biological therapyanti-TNF
Infliximab
Neutralisation of soluble
TNF
TNF producing
macrophages of activated T
cells
Neutralisation of transmembrane TNF
van Deventer SJH. Gut 1997: 40; 443–8.Scallon BJ et al. Cytokine 1995: 7; 251–9.Feldmann M et al. Adv Immunol 1997; 64: 283–350.

Chimeric monoclonal antibody (75% human
IgG1 isotype)
InfliximabInfliximab
IgGIgG11
MouseMouse HumanHuman
PEG, polyethylene glycolPEG, polyethylene glycol..
Humanized Fab’fragment (95% human
IgG1 isotype)
Certolizumab PegolCertolizumab Pegol
PEGPEG
PEGPEG
VHVHVLVL
CCHH11
No FcNo Fc
Human recombinant antibody (100% human
IgG1 isotype)
AdalimumabAdalimumab
IgGIgG11
Construct of Anti-TNF-α Biologic Agents
Construct of Anti-TNF-α Biologic Agents

Anti-TNF safety
Hypersensitivity Allergic reaction at time of infusion – 5%
Autoimmune syndromes Lupus like illness – rare and recovers on stopping on therapy
Infection Profound immunosuppression occurs Opportunistic infections can occur Tuberculosis high risk Hepatitis B can be reactivated
Cancer Recent data suggests that overall cancer rates may be reduced Hepatosplenic T-cell lymphomas – 1 in 20000 patients

Integrins
MAdCAM-1
VCAM-1
Gut-homingT-cell
Integrin
Integrin
Recommended