
Workshop 2012 – Oxygen Safety 1
The Safe Use and Prescription of Medical Oxygen
Luke HowardConsultant Respiratory Physician
Imperial College Healthcare NHS Trust&
Co-Chair, British Thoracic Society Emergency Oxygen Guideline Group

Workshop 2012 – Oxygen Safety 2
Topics to be covered
• Oxygen physiology– How is oxygen delivered and utilised– How is carbon dioxide cleared– How can oxygen delivery be optimised
• Dangers of oxygen• BTS Guidelines
– Monitoring– Delivery

Workshop 2012 – Oxygen Safety 3
“The Oxygen Cascade ”

Workshop 2012 – Oxygen Safety 4
“The Oxygen Cascade ”
Workshop 2012 – Oxygen Safety 5
O2
O2O2
ATP
O2
O2The Oxygen Cascade

Workshop 2012 – Oxygen Safety 6
ATP
O2
O2
What can change?
Gas exchange
FiO2
•Oxygen carrying & buffering capacity•Flow
Oxygen utilisation

Workshop 2012 – Oxygen Safety 7
Oxygen Delivery
DO2 = Q x {[SaO2/100 x Hb x 1.3]+ [PaO2 x 0.003 x 10]}
Stagnant Hypoxia Anaemic
HypoxiaHypoxaemicHypoxia
Cytopathic HypoxiaCytopathic Hypoxia

Workshop 2012 – Oxygen Safety 8
Resting oxygen consumption remains constant until PaO2falls below 23 mmHg (~3kPa) Anesthesiology 2001;95:A1123
↑Cardiac output↑O2 extraction
↑Cardiac output↑O2 extraction

Workshop 2012 – Oxygen Safety 9
O
7
VO
2(m
l/kg/
min
)
OPaO2 (mmHg)
100
14Increased metabolic
demand
Impaired cardiac reserve
AnaemiaTissue oedema
Mitochondrial dysfunction

Workshop 2012 – Oxygen Safety 10
“The Oxygen Cascade ”
Workshop 2012 – Oxygen Safety 11
Dangers of Oxygen Therapy
Workshop 2012 – Oxygen Safety 12
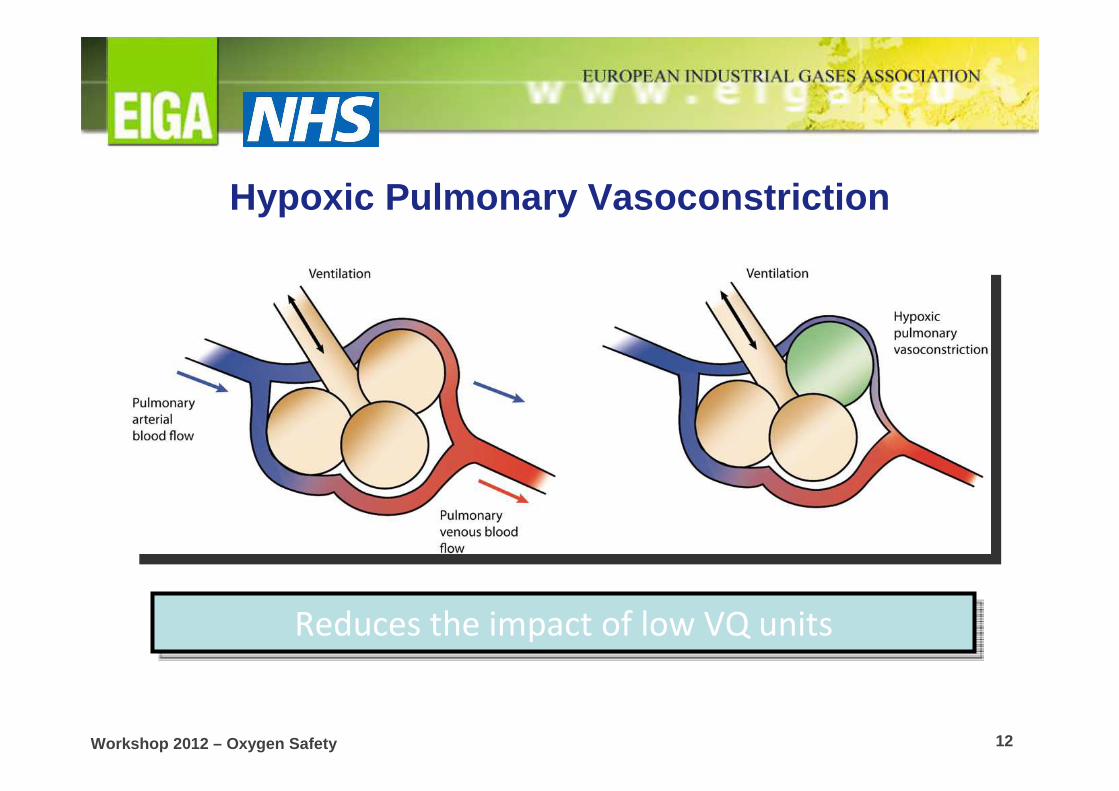
Hypoxic Pulmonary Vasoconstriction
Reduces the impact of low VQ unitsReduces the impact of low VQ units

Workshop 2012 – Oxygen Safety 13
Impaired respiratory mechanics, eg, COPDImpaired respiratory mechanics, eg, COPD
Acidosis
Coma
Acidosis
Coma
Alveolar hypoventilation Hypercapnia
Workshop 2012 – Oxygen Safety 14
Ventilation -perfusion matching and oxygen administration
• Diverts blood flow away from diseased lung• Uses low oxygen levels in diseased lung to
“signal” to divert blood away• Administering oxygen masks this signal• Diseased lung is less efficient at clearing carbon
dioxide• When respiratory mechanics are impaired, eg
COPD, this inefficiency cannot be compensated for by increasing overall ventilation and carbon dioxide retention occurs

Workshop 2012 – Oxygen Safety 15
Plant et al., Thorax 2000
• 47% of 982 patients with exacerbation of COPD were hypercapnic on arrival in hospital
• 20% had Respiratory Acidosis (pH < 7.35)
• 5% had pH < 7.25 (and were likely to need ICU care)

Workshop 2012 – Oxygen Safety 16
Risk of Oxygenation in COPD
<7.3
7.3-
10 10-
13.3>
13.3
Plant et al., Thorax 2000, 55: 550-4
Increased risk
of intubation

Workshop 2012 – Oxygen Safety 17

Workshop 2012 – Oxygen Safety 18
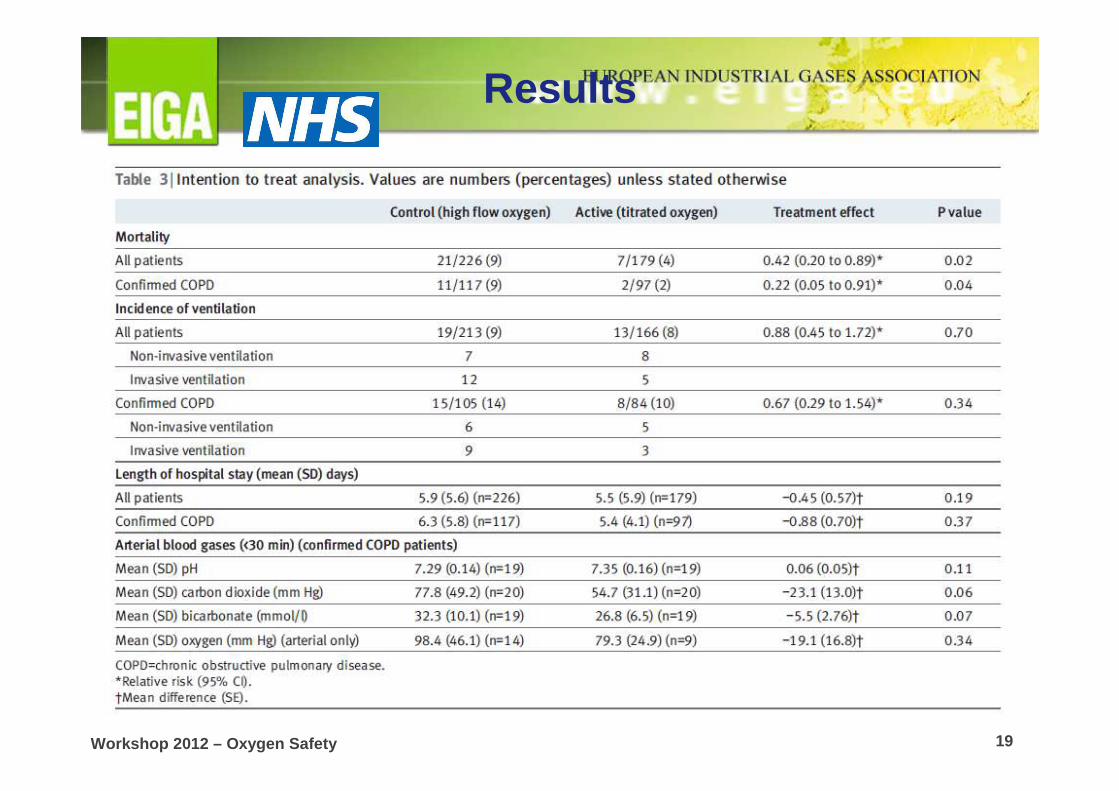
Randomised Controlled Trial of Titrated vsHigh -Flow Oxygen
• Pre-hospital setting• Tasmania• 405 patients with presumed exacerbation of COPD• Titrated arm:
– Nasal prongs to achieve SpO2 88-92%• High-Flow arm:
– 8-10 l/min non-rebreathing mask
Austin et al., BMJ 2010
Workshop 2012 – Oxygen Safety 19
Results

Workshop 2012 – Oxygen Safety 20
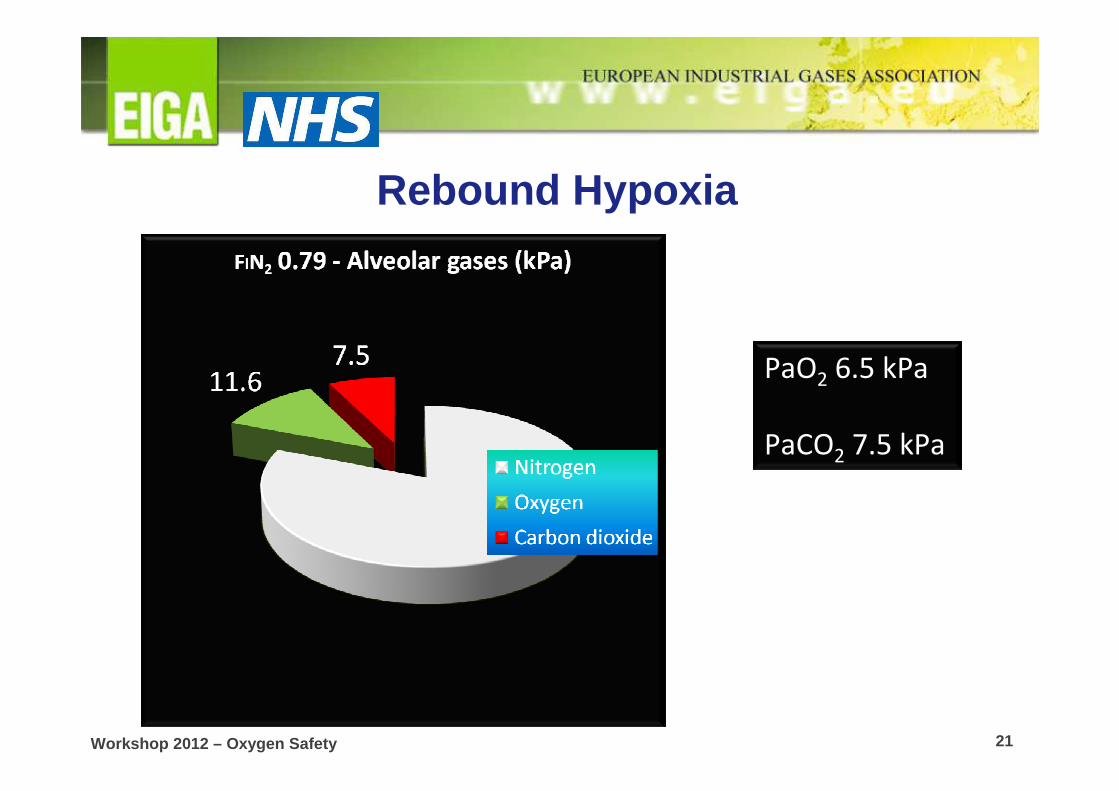
Danger 2: Alveolar Gas Equation and “Rebound Hypoxia”
• PAO2 = PIO2 – PaCO2/RER
• PAO2 = (100 - PIN2) – PaCO2/RER
• Case study:– COPD exacerbation at home - on air– Seen by ambulance crew – given high flow
oxygen– Brought to ER – oxygen removed
Workshop 2012 – Oxygen Safety 21
PaO2 6.5 kPa
PaCO2 7.5 kPa
Rebound Hypoxia

Workshop 2012 – Oxygen Safety 22
PaO2 32 kPa
PaCO2 10 kPa
Rebound Hypoxia

Workshop 2012 – Oxygen Safety 23
PaO2 3.5 kPa
PaCO2 10 kPa
Rebound Hypoxia
Workshop 2012 – Oxygen Safety 24
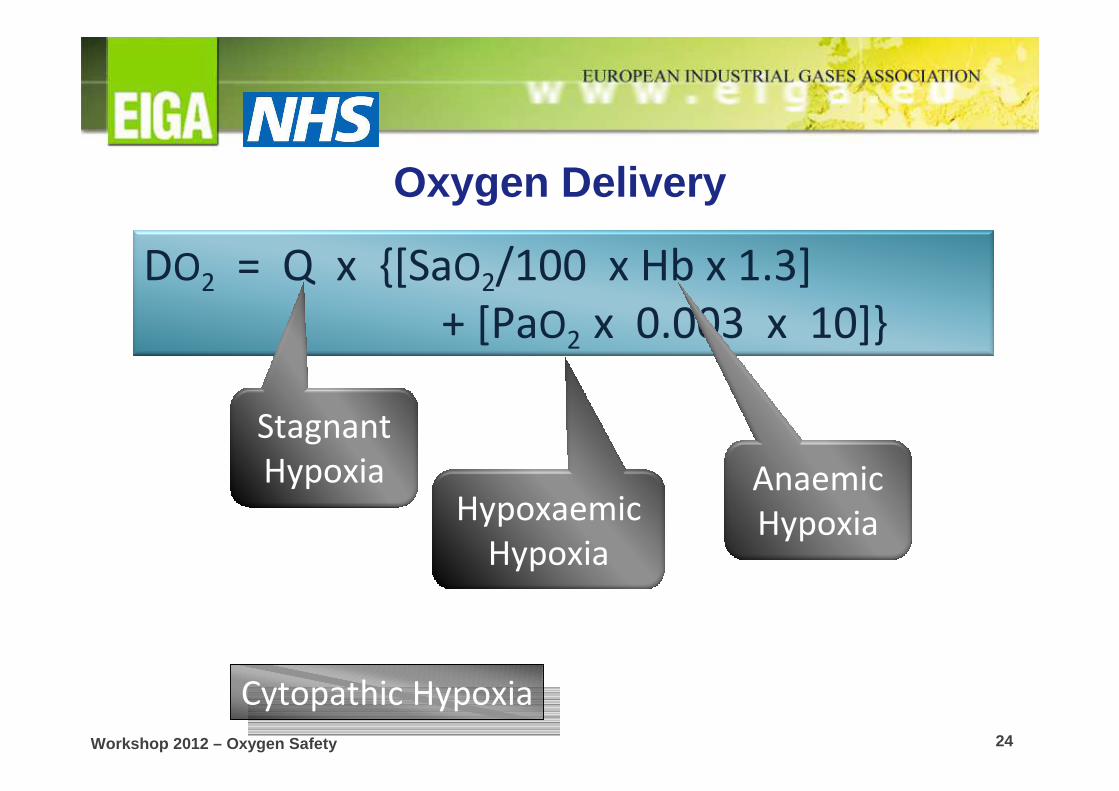
Oxygen Delivery
DO2 = Q x {[SaO2/100 x Hb x 1.3]
+ [PaO2 x 0.003 x 10]}
Stagnant
Hypoxia Anaemic
HypoxiaHypoxaemic
Hypoxia
Cytopathic Hypoxia

Workshop 2012 – Oxygen Safety 25
DO2 = Q x {[SaO2/100 x Hb x 1.3]
+ [PaO2 x 0.003 x 10]}High flow oxygen:
•Decreased cardiac output
•Decreased coronary flow (~20%)
•Increased systemic vascular resistance
High flow oxygen:
•Decreased cardiac output
•Decreased coronary flow (~20%)
•Increased systemic vascular resistance
Circulatory effects of decreasing
oxygen??
Circulatory effects of decreasing
oxygen??

Workshop 2012 – Oxygen Safety 26
Capillary
PaO2 13 kPa
PmtO2 0.5 – 3.0 kPa
PvO2 6 kPa

Workshop 2012 – Oxygen Safety 27
Dangers 3,4,5....: High -Flow Oxygen?• Coronary vasoconstriction ( ↓flow by <23%)• Increased Systemic Vascular Resistance • Reduced Cardiac Index• Possible reperfusion injury post MI and mild-
moderate stroke• Hypoxic lung injury
Harten JM et al J Cardiothoracic Vasc Anaesth 2005; 19: 173-5
Kaneda T et al. Jpn Circ J 2001; 213-8
Frobert O et al. Cardiovasc Ultrasound 2004; 2: 22
Haque WA et al. J Am Coll Cardiol 1996; 2: 353-7
Thomaon aj ET AL. BMJ 2002; 1406-7
Ronning OM et al. Stroke 1999; 30
McNulty, PH et al. JAP 2007; 102; 2040-45.

Workshop 2012 – Oxygen Safety 28
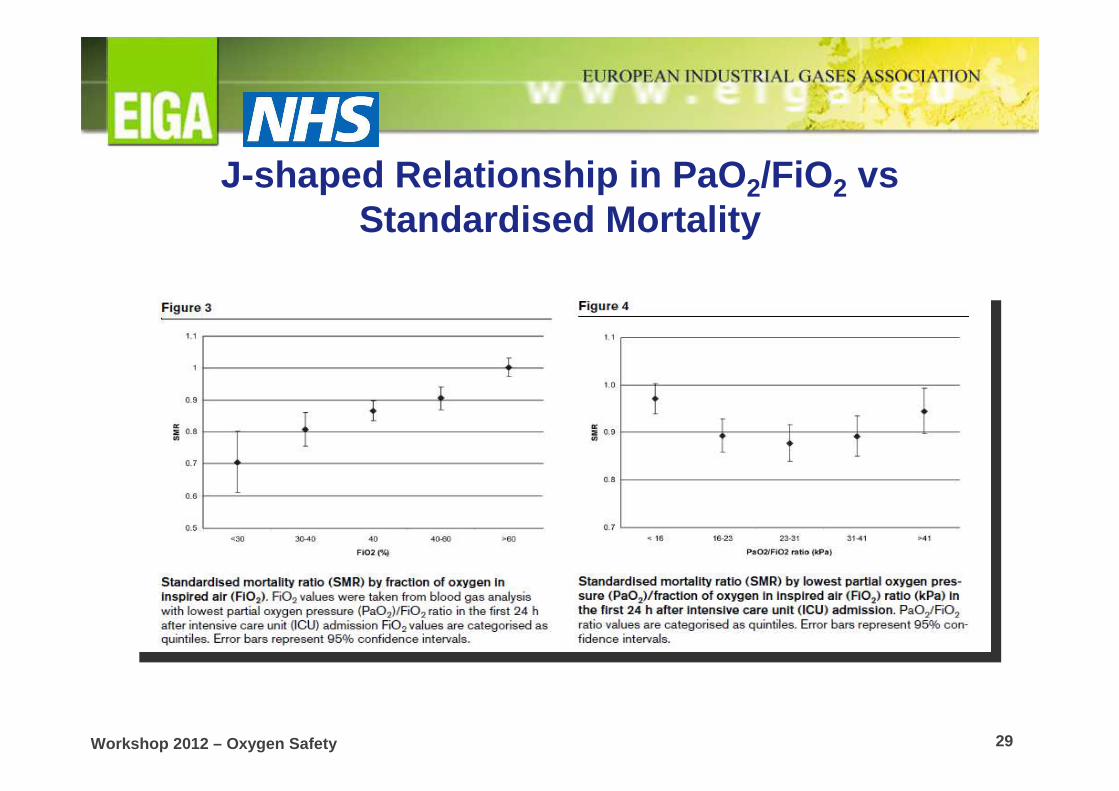
Retrospective analysis of ICU mortality• 36,307 patients
in 50 Dutch ICUs
De Jonge et al., CritCare 2008
Workshop 2012 – Oxygen Safety 29
J-shaped Relationship in PaO 2/FiO2 vsStandardised Mortality
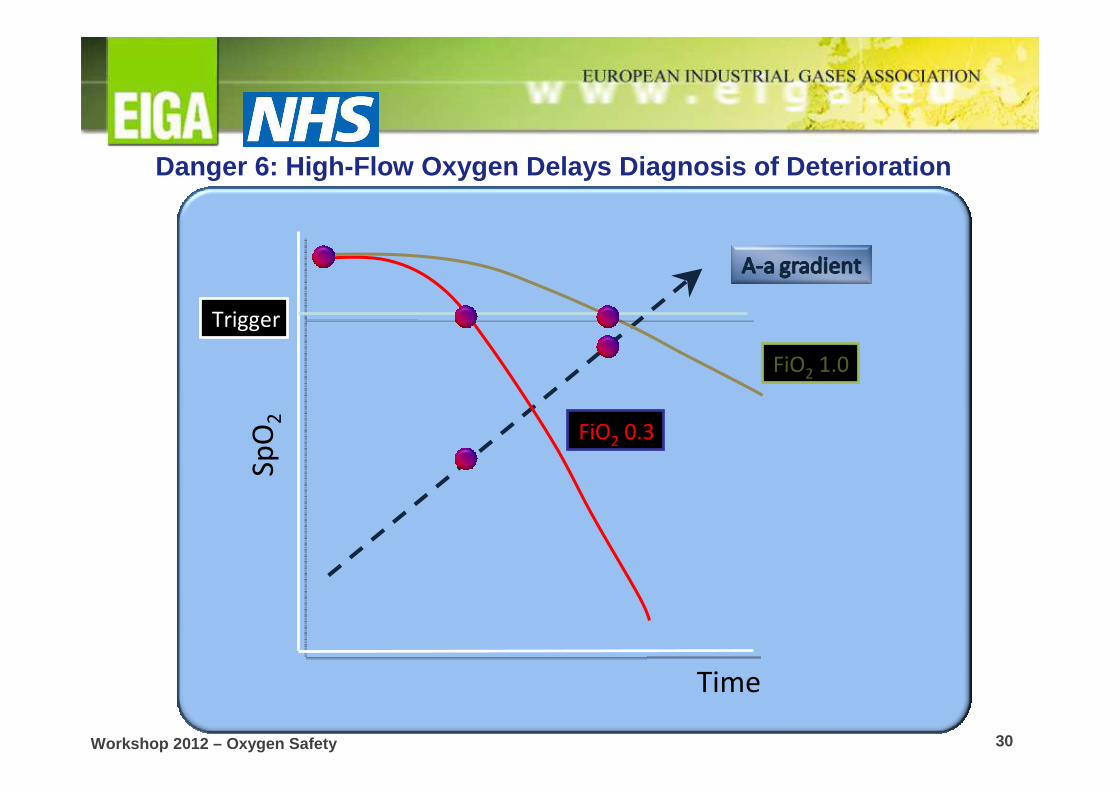
Workshop 2012 – Oxygen Safety 30
Time
Sp
O2
FiO2 0.3
FiO2 1.0
Trigger
Danger 6: High-Flow Oxygen Delays Diagnosis of Deteri oration

Workshop 2012 – Oxygen Safety 31
BTS Guidelines

Workshop 2012 – Oxygen Safety 32
How to Approach the Patient on ‘100% Oxygen ’in hypercapnic failure
• Patient conscious:– Change to 35% Venturi Device
• Patient drowsy:– Leave the patient on high-flow oxygen then,– Start NIV with Oxygen / call ICU

Workshop 2012 – Oxygen Safety 33
Step up and down through oxygen delivery devicesStep up and down through oxygen delivery devices
To avoid
rebound
hypoxia
In case of
higher
respiratory
rates/flows

Workshop 2012 – Oxygen Safety 34
Step up and down through oxygen delivery devicesStep up and down through oxygen delivery devices
Pre-hospital

Workshop 2012 – Oxygen Safety 35
Step up and down through oxygen delivery devicesStep up and down through oxygen delivery devices
Once
stable
Workshop 2012 – Oxygen Safety 36
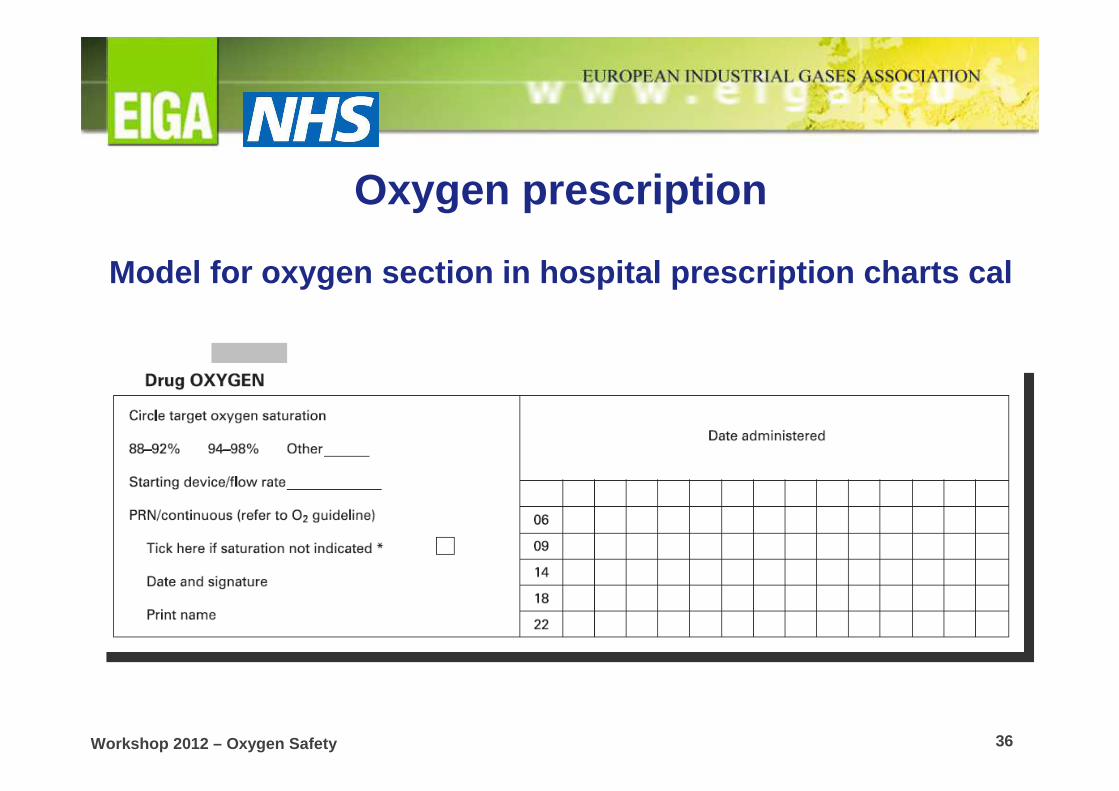
Oxygen prescription
Model for oxygen section in hospital prescription c harts cal
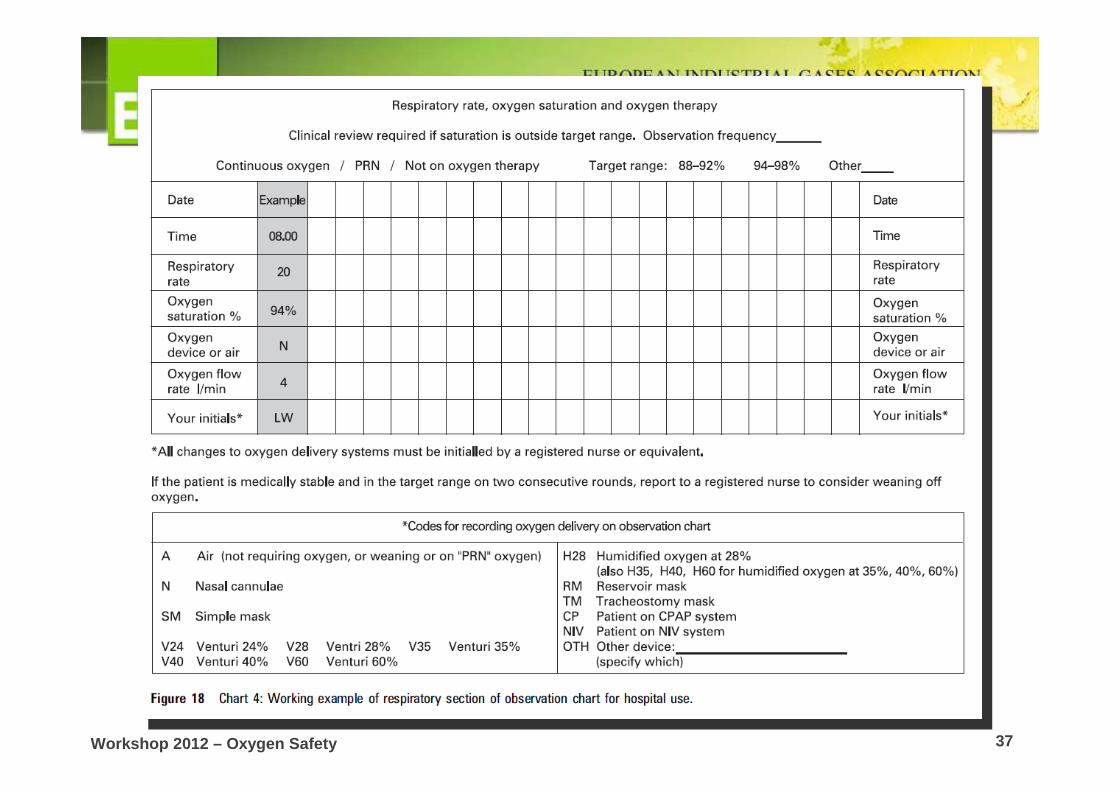
Workshop 2012 – Oxygen Safety 37
Recommended

















