Introduction to Call
Jeff Monteith, M.D.

When am I on call?
• Go to imsumma.org • Click under schedules on the main page • Find your name on the chart and show up ON TIME

The Rules
• Call hour restrictions – Most calls are ~ 1216 hour shifts – Maximum number of consecutive hours in the hospital = 16 hours
– Must have off at least 10 consecutive hours between shifts

Responsibilities

Beep…beep…beep
Pager goes off... • 1st question to ask yourself is whether or not the patient needs to be seen Immediately. ALWAYS GO SEE THE PATIENT • Need to triage patients based on the severity/acuity of the problem if you are evaluating multiple patients at once • Often times, the rapid response team will be evaluating the patient
On the phone
• When you first talk to the nurse make sure you obatin – Patient name, recent vitals, brief overview of the problem, and stability of the patient
– Find out the attending covering the patient. – If the patient is not a Med Team patient (i.e. surgical, FP, or private patient) you do not need to see it, unless it’s an emergency
– Give any phone orders you need to and go see the patient

Always Go See The Patient!!

At the bedside Go see the patient – Quickly review the chart and vitals – Focused history and physical exam – Discuss the case with the senior resident if you are unsure of the appropriate workup/ intervention – Write a note on the chart detailing the specific problem, vitals, physical exam findings, pertinent lab results, and assessment and plan. Also include the name of the senior resident or attending that you discussed the case with if applicable.
Final Advice
• Always go see the patient • Call your senior if you don’t know what do • Be nice to the nurses and hospital staff • Always call the attending if you see one of their patients
• Be an active participant in code blue/stroke teams • Don’t move into the call rooms • And finally…. Have fun and don’t kill anybody
Chest Pain
Jeff Monteith, M.D.

Common Causes
• Cardiac – MI, angina, pericarditis, aortic dissection
• Pulmonary – Pneumonia, pleuritis, pneumothorax, PE, pulm HTN
• GI – GERD, PUD, pancreatitis, esophageal spasm
• Other – Costochondritis, anxiety….
On the phone
• Get the most recent vitals and stability of the patient from the nurse
• Order a Stat EKG and any other tests or medications
• Go see the patient immediately

At the bedside
• Quickly review the chart and vitals • Does the patient have a history of CAD? (if so does the pain resemble previous episodes of chest pain)
• Location/quality/duration/severity/radiation of chest pain
• Change in the quality/severity of chest pain with respiration
• Diaphoresis, N/V, fever
At the bedside
• Any particular precipitating factors/relieving measures
• Any recent procedures (i.e., subclavian line placement)
• Review EKG. Have senior resident review every EKG until you are comfortable interpreting them
Physical Exam
• General: Assess for signs of distress or change in mental staus
• Vitals: hypotensive (alarming sign), tachycardia(i.e., PE, response to pain…), bradycardia (i.e., AV block from inferior MI), take BP in both arms (aortic dissection).
• Chest: chest wall tenderness, murmur/rubs/gallops • Lungs: crackles, absent breath sounds on one side • Abdomen: tenderness, bowel sounds • Extremities: edema, evidence of DVT, B/L pulses in upper and lower extremities (aortic dissection)

Initial Workup
• Labs/Imaging • EKG • Serial cardiac enzymes • Portable CXR • ABG (respiratory distress or low O2 sats) • CTA chest or DDimer • CT chest with contrast or TEE (dissection) • Echocardiogram

Management MI based on EKG and
history – stat cardiology consult and
transfer to CCU – Cardiac monitor, ensure IV
access – ASA, BBlocker, nitrates,
morphine, heparin, antiplatelet agents, reperfusion therapy, O2
– Angina – NTG, telemetry, consider Bblockers, heparin, antiplatelet agents
Dissection – immediate transfer to CCU, nitroprusside or labetalol for BP control, stat vascular/thoracic surgery consult
PE 02, IV heparin, pain control. Consider interventional radiology consult for IVC filter placement if anticoagulation is contraindicated

Management Pneumothorax • Tension pneumothorax (hypotension, tracheal deviation, venous distention, and severe respiratory distress) requires needle decompression (2 nd intercostal space in midclavicular line), followed by chest tube • Other pneumothoraces involving >20% of the lung require chest tube (<20% can usually be treated with O2 and observation) GI • Antacids prn, H2 antagonists, elevate the head of the bed Costochondritis NSAIDs

Shortness of Breath Shortness of Breath
Jon Tomada, MD Jon Tomada, MD

Shortness of Breath Shortness of Breath
§ Gradual or acute? § Associated symptoms? § Vital signs including pulse ox? § Admitting diagnosis? § Related past medical problems? § Code status?
§ Gradual or acute? § Associated symptoms? § Vital signs including pulse ox? § Admitting diagnosis? § Related past medical problems? § Code status?

Shortness of Breath Shortness of Breath
§ Oxygen support § ? Stat CXR § ? Stat EKG § ?? ABG
§ Oxygen support § ? Stat CXR § ? Stat EKG § ?? ABG

Oxygen Support Oxygen Support
§ Room Air : FiO2 ~ 21% § Nasal Cannula : +3 FiO2 per 1 L/min increase in oxygen; increase up to 5 L/min § Venti Mask § Non rebreather mask § Dual flow mask § Bilevel positive air pressure (BiPap)
§ Room Air : FiO2 ~ 21% § Nasal Cannula : +3 FiO2 per 1 L/min increase in oxygen; increase up to 5 L/min § Venti Mask § Non rebreather mask § Dual flow mask § Bilevel positive air pressure (BiPap)
SEE THE PATIENT!!! SEE THE PATIENT!!!
Shortness of Breath Shortness of Breath § Pulmonary
– Pneumonia – COPD – Asthma – Pleural effusion – Pneumothorax – PE – Aspiration – Atelectasis
§ Cardiac – CHF – MI – Arrhythmia
§ Pulmonary – Pneumonia – COPD – Asthma – Pleural effusion – Pneumothorax – PE – Aspiration – Atelectasis
§ Cardiac – CHF – MI – Arrhythmia
§ Pericardial effusion § Neuromuscular § Psychogenic § Others
– Anemia – Deconditioning – CO poisoning – Massive ascitis – Renal failure – Med induced – anaphylaxis
§ Pericardial effusion § Neuromuscular § Psychogenic § Others
– Anemia – Deconditioning – CO poisoning – Massive ascitis – Renal failure – Med induced – anaphylaxis

At bedside At bedside
§ Focused history and PE § Talk to the nurses, Resp therapist § Review available data
§ Focused history and PE § Talk to the nurses, Resp therapist § Review available data
COPD COPD
§ Wheezing § Hx of tobacco use § Wheezing § Hx of tobacco use
§ Albuterol § Atrovent § Methylprednisolone 125 mg IV q 6hrs § Cultures § Bacterial antigens § Antibiotics
§ Albuterol § Atrovent § Methylprednisolone 125 mg IV q 6hrs § Cultures § Bacterial antigens § Antibiotics

Pneumonia Pneumonia
§ cough § Fever/hypothermia § Leukocytosis or leukopenia § Bandemia § Lungs with crackles, wheeze, rhonchi
§ cough § Fever/hypothermia § Leukocytosis or leukopenia § Bandemia § Lungs with crackles, wheeze, rhonchi
§ Oxygen support § Cultures (blood and sputum) § Bacterial antigen § Antibiotics
§ Oxygen support § Cultures (blood and sputum) § Bacterial antigen § Antibiotics

CHF CHF
§ JVD § Fluid overload § Lungs with crackles § Displaced PMI § S3 § Heart murmur § Edema
§ JVD § Fluid overload § Lungs with crackles § Displaced PMI § S3 § Heart murmur § Edema
§ Oxygen § Stop fluids § Lasix IV § Nitroglycerin SL § Morphine IV § Look for etiology then treat
§ Oxygen § Stop fluids § Lasix IV § Nitroglycerin SL § Morphine IV § Look for etiology then treat
MI MI
§ Chest pain/tightness § Anginal equivalent sx § Lightheadedness § Palpitation § Risk factors
§ Chest pain/tightness § Anginal equivalent sx § Lightheadedness § Palpitation § Risk factors
§ Oxygen § Nitroglycerin § Aspirin § Morphine § Metoprolol § Cardiac enzymes § Aim for resolution of angina
§ Oxygen § Nitroglycerin § Aspirin § Morphine § Metoprolol § Cardiac enzymes § Aim for resolution of angina

Intubation Intubation
§ When you start thinking about it… § Declining mental status § Unable to improve oxygen saturation § Patient getting tired: RR >30 § ABG: pH <7.30, pO2<60, pCO2>50; normal pH on a tachypneic patient § FULL CODE § Call your senior
§ When you start thinking about it… § Declining mental status § Unable to improve oxygen saturation § Patient getting tired: RR >30 § ABG: pH <7.30, pO2<60, pCO2>50; normal pH on a tachypneic patient § FULL CODE § Call your senior

DON’T FORGET DON’T FORGET
§ Write a note on patient’s chart § Notify patient’s PCP § Call your senior if you do not know what to do § Follow up labs/tests that you ordered § Do not leave the patient if he/she is unstable
§ Write a note on patient’s chart § Notify patient’s PCP § Call your senior if you do not know what to do § Follow up labs/tests that you ordered § Do not leave the patient if he/she is unstable

Under Pressure (Hypertension/Hypotension)
Connie J. Tomada MD

HYPERTENSION

Hypertension History Taking n Phone call
n Why is the patient in the hospital? n Is the patient pregnant? (Pre eclampsia/Eclampsia)
n Is the patient taking antidepressants? (MAO inhibitors)
n How high is the BP and what has the BP been previously?
n Does the Pt have symptoms suggestive of hypertensive emergency?
n What antihypertensives has the patient been taking?
Hypertension Elevator Thoughts n Work out your differential diagnoses
n Benign vs. Hypertensive Urgency vs. Hypertensive Emergency
n Major threats n Eclampsia n Aortic dissection n Pulmonary edema n Myocardial infarction n Hypertensive encephalopathy
Hypertension Bedside n What is the BP and HR?
n Retake BP in both arms (make sure to use the correct BP cuff size)
n Bradycardia + Hypertension in Pt not receiving beta blockers = increasing intracranial pressure
n Tachycardia + Hypertension = catecholamine crisis

Hypertension Focused History n Any symptoms suggestive of hypertensive emergency? n Headache n Blurring of vision n Chest pain n Dyspnea n Back or chest pain n Unilateral weakness/sensory symptoms

Hypertension Focused PE n HEENT: Assess the fundi for hypertensive changes/papilledema
n Lungs: Crackles, pleural effusion n CVS: Elevated JVP, S3 n Neuro: Confusion, delirium, agitation, lethargy, localized deficits

Hypertension Management n Essential hypertension
n In an asymptomatic patient acute lowering of BP is NOT indicated (Remember, treat the Patient not the number)
n Hypertensive urgency n SBP > 210 or DBP > 120 with no target organ damage
n Decrease MAP by 25% slowly within 24 hours

Hypertension Management n Hypertensive emergency
n Elevated BP with acute targetorgan damage
n Call your resident now to transfer the Pt to the ICU/CCU!
n Decrease MAP by 25% in minutes to 2 hours
Hypertension Management
n KNOW WHICH DRUGS YOU CAN GIVE, AND WHICH ONES YOU SHOULDN’T
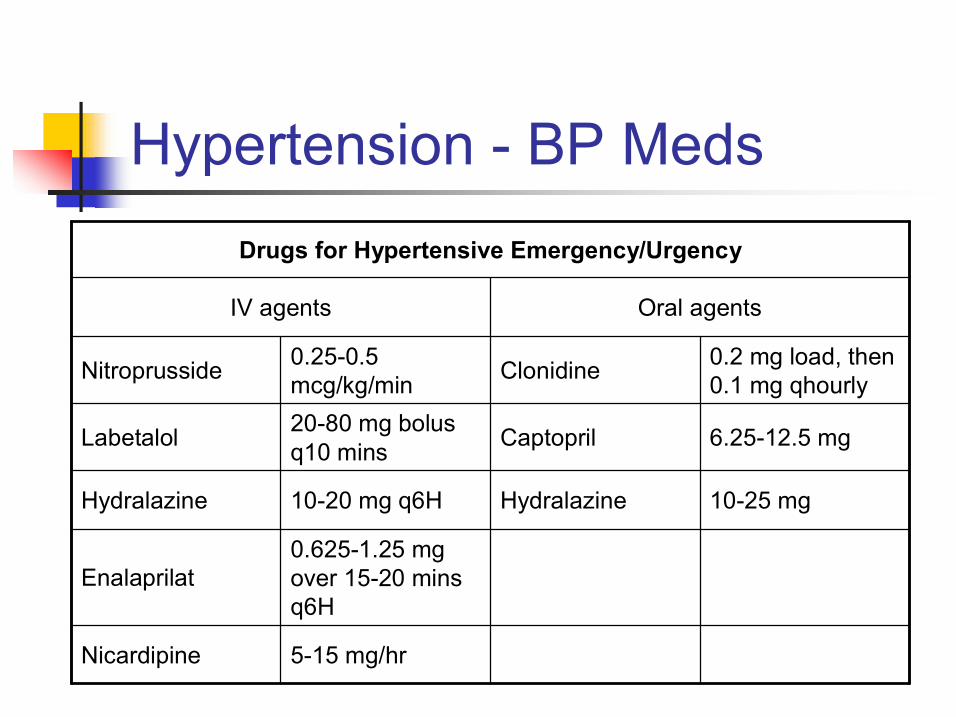
Hypertension BP Meds
515 mg/hr Nicardipine
0.6251.25 mg over 1520 mins q6H
Enalaprilat
1025 mg Hydralazine 1020 mg q6H Hydralazine
6.2512.5 mg Captopril 2080 mg bolus q10 mins Labetalol
0.2 mg load, then 0.1 mg qhourly Clonidine 0.250.5
mcg/kg/min Nitroprusside
Oral agents IV agents
Drugs for Hypertensive Emergency/Urgency

HYPOTENSION

Hypotension History Taking n Phone Call
n What’s the BP? n What’s the HR? n What’s the temperature? n Is the Pt conscious? n Is the Pt having chest pain? n Has the Pt been given IV contrast or antibiotic (think about anaphylaxis)?
n What was the admitting diagnosis?
Hypotension Elevator Thoughts n Hypotension requires you to see the patient IMMEDIATELY.
n Work out your differential diagnoses n Cardiogenic causes (MI, PE, tension pneumothorax, cardiac tamponade)
n Hypovolemia n Sepsis n Anaphylaxis n Adrenal crisis

Hypotension Bedside n Check airway and repeat vital signs (your ABCs)
n Is the patient in shock? n Assess the volume status
n Only cardiogenic shock will give you a clinical picture of volume overload
Hypotension Focused PE n Vitals: orthostatic vitals n HEENT: Elevated JVP (CHF, tamponade, PE, tension pneumothorax), flat neck veins
n Lungs: Stridor, crackles, pleural effusion, wheezes
n CVS: S3, rhythm abnormalities n Extremities: Edema, mottling, clammy n Skin: Urticaria n Neuro: mental status changes

Hypotension Immediate measures n Call your resident: Shock patients need to go to the ICU/CCU
n Labs: stat EKG, portable CXR, cardiac enzymes, CBC, BMP, lactic acid, mixed venous gas, ABG, type and cross, cortisol level, pancultures
Hypotension Management n If hypovolemic:
n Normalize intravascular volume n Reverse Trendelenburg n Blood transfusion if clinically bleed
n If anaphylaxis: n epinephrine, diphenhydramine, steroids
n If adrenal crisis: n Draw cortisol level PRIOR to giving IV steroids

Hypotension Management n If cardiogenic:
n treat the specific cause (e.g. MI urgent cath; tamponade pericardiocentesis; tension pneumothorax needle thoracostomy; PE thrombolytic therapy vs. anticoagulation)
n If sepsis: n Fluids, fluids, fluids, broadspectrum antibiotics and vasopressor support (if resistant to fluid resuscitation)

Good Luck Class 2011!

Abdominal Pain Abdominal Pain Ami R. Shah, DO Ami R. Shah, DO

Abdominal Pain Abdominal Pain
Is this a surgical Is this a surgical emergency???? emergency????

Differential Diagnosis Differential Diagnosis n n Gastrointestinal Disorders Gastrointestinal Disorders
– – Appendicitis Appendicitis – – Small and large bowel obstruction Small and large bowel obstruction – – Perforated peptic ulcer Perforated peptic ulcer – – Incarcerated hernia Incarcerated hernia – – Bowel perforation Bowel perforation – – Diverticulitis Diverticulitis – – IBD IBD – – Gastroenteritis Gastroenteritis – – Gastritis Gastritis – – Mallory Mallory Weiss Tears Weiss Tears
n n Liver, spleen, and Liver, spleen, and billary billary tract tract disorders disorders – – Acute cholecystitis Acute cholecystitis – – Acute cholangitis Acute cholangitis – – Ruptured spleen Ruptured spleen
n n Pancreatic Disorders Pancreatic Disorders – – Pancreatitis Pancreatitis
n n Urinary Disorders Urinary Disorders – – Nephrolithiasis Nephrolithiasis – – pyelonephritis pyelonephritis
n n Gynecologic Disorders Gynecologic Disorders – – Ectopic pregnancy Ectopic pregnancy – – Ruptured ovarian cyst Ruptured ovarian cyst – – Endometriosis Endometriosis – – dysmenorrhea dysmenorrhea
n n Vascular Disorders Vascular Disorders – – AAA AAA – – Mysenteric Mysenteric ischemia ischemia
n n Peritoneal Disorders Peritoneal Disorders – – Peritonitis Peritonitis – – Intraabdominal abscess Intraabdominal abscess
n n Retroperitoneal Disorders Retroperitoneal Disorders – – Retroperitoneal Retroperitoneal hemmorhage hemmorhage

Abdominal Pain Abdominal Pain n n History History
– – Where is the pain located? Where is the pain located? § § Unilateral, midline, periumbilical, lower abdominal Unilateral, midline, periumbilical, lower abdominal § § Think of the four abdominal quadrants and what organs are Think of the four abdominal quadrants and what organs are contained in each. contained in each.
– – Does it radiate? Does it radiate? § § Shoulder? Groin? Thigh? Shoulder? Groin? Thigh?
– – Quality? Quality? § § Colicky? Tearing? Dull? Sharp? Colicky? Tearing? Dull? Sharp?
– – What makes the pain better or worse? What makes the pain better or worse? § § Position? Deep inspiration? meals? Position? Deep inspiration? meals?
– – Associated symptoms? Associated symptoms? § § Vomiting? Diarrhea? Constipation? Cough? Hematuria? Vomiting? Diarrhea? Constipation? Cough? Hematuria?
– – Past medical history, menstrual history & medications Past medical history, menstrual history & medications

Abdominal Pain Abdominal Pain
n n Physical Exam Physical Exam – – Vitals: fever? Tachycardia? Hypotension? Vitals: fever? Tachycardia? Hypotension? § § Give clues to an infection, inflammation, or volume Give clues to an infection, inflammation, or volume loss. loss.
– – General Appearance General Appearance § § Jaundice? Jaundice? § § Position that provides some comfort Position that provides some comfort vs vs writhing in writhing in pain. pain.

Abdominal Pain Abdominal Pain
n n Physical Exam (continued) Physical Exam (continued) – – Abdominal Exam Abdominal Exam § § Inspection Inspection
– – Distention? Cullen sign? Gray Turner Distention? Cullen sign? Gray Turner’ ’s sign? Caput medusae? s sign? Caput medusae?
§ § Auscultation Auscultation – – Normal, hypoactive, or hyperactive? Normal, hypoactive, or hyperactive? – – Bruits? Bruits?
§ § Percussion Percussion – – Fluid wave? Tympany? Fluid wave? Tympany?
§ § Palpation Palpation – – Localized vs. diffuse tenderness? Aortic pulsation? Localized vs. diffuse tenderness? Aortic pulsation?
n n Physical Exam Physical Exam
– –Don Don’ ’t Forget the Rectal t Forget the Rectal Exam Exam

Abdominal Pain Abdominal Pain
n n Labs Labs – – CBC CBC § § Leukocytosis, anemia (remember with acute blood loss, the Leukocytosis, anemia (remember with acute blood loss, the H/H may not normalize for a few hours). H/H may not normalize for a few hours).
– – CMP CMP § § Elevated BUN/Cr?, elevated Elevated BUN/Cr?, elevated LFTs LFTs? Hypokalemia? ? Hypokalemia? acidosis/alkalosis? acidosis/alkalosis?
– – Amylase/lipase Amylase/lipase – – Stool Stool Guiacs Guiacs – – U/A U/A § § Hematuria? Pyuria? Hematuria? Pyuria?
Abdominal Pain Abdominal Pain
n n Imaging Imaging – – Abdominal films Abdominal films § § Free air? Ileus? Obstruction? Constipation? Free air? Ileus? Obstruction? Constipation?
– – Ultrasound (RUQ, retroperitoneal) Ultrasound (RUQ, retroperitoneal) § § Gallstones? Hydronephrosis? Ectopic pregnancy? Gallstones? Hydronephrosis? Ectopic pregnancy?
– – Abdominal CT Abdominal CT § § Appendicitis? Diverticulitis? AAA? Appendicitis? Diverticulitis? AAA? § § Possibly considered the most sensitive test for Possibly considered the most sensitive test for evaluating abdominal pathology. evaluating abdominal pathology.
Abdominal Pain Abdominal Pain
n n Plan Plan – – Labs, imaging Labs, imaging – – STAT surgical consult if acute abdomen STAT surgical consult if acute abdomen – – NG tube if high suspicion of obstruction. NG tube if high suspicion of obstruction. – – IVF IVF – – Pain medications Pain medications – – Laxatives, enemas Laxatives, enemas – – Anti Anti emetics emetics – – Anti Anti spasmodics spasmodics – – Call your senior if things start going downhill !!! Call your senior if things start going downhill !!!

Mental Status Change
Ashita Sinha D.O.

Mental Status Change
• Problem: Floor call “patient is acting inappropriately.

Mental Status Change
• IMPORTANT Questions 1. How is the Pt confused? 2. What are the vitals? (new set) Need BP,
HR, Temp, O2 3. If Pt is Diabetic check for↓MBS 4. Why was the Pt admitted? 5. Ever happened before? 6.If Pt fell LOC? Head Trauma?
Mental Status Change
• Look thru the Chart/ Call PCP if needed to get an accurate history of pt’s baseline
• Question family if they are present • Meds administered: new/ old. • Demented
Mental Status Change
Differential Dx • Dementia (NL LOC) vs. Delirium • Head bleed from Fall • TIA/CVA • Postictal• Malignancy • HTN/Wernecke‛s encephalopathy • Vit. B12 deficiency
Mental Status Change • Don’t miss the bad stuff: 1. Intercranial mass: bleed, abscess, 2. CVA: asymmetry on neuro exam, • Rx: CT head, BAT team, call Neuro 3. Delirium Tremens: confusion, tachy,
fever, dilated pupils, diaphoresis • Rx: Valium, thiamine, folate, MVI 4. Meningitis: HA, stiff neck, fever, sz • Rx: CT head, LP, Abx

Mental Status Change Other Causes 1. Drugs: Etoh w/d, narcotics, benzos • psychotropic meds, etc. • Rx: Ativan, narcan, flumazenil, d/c med 2. Organ failure:↑CO 2 ,↓O 2 ,↑uremia 3. Changes in glucose, Na+, Ca 2 + Rx: replace 4. Infections: Meningitis, encephalitis, • abscess, lyme‛s Dz 5. Psych: Schizophrenia, mania, etc.

Mental Status Change
• Complete Physical Exam – Neck: Kernig/ Brudinski – Lungs: Crackles & wheeze – Heart: Irregular, new murmur – Abd: Stigmata of Liver ds – Skin: Jaundice, rashes – Neuro: NIH – Sx of Trauma

Mental Status Change
• CBC infection/ anemia • BMP electrolyte abnl (ask for BGT) • ABG if signs of respiratory distress • Urine studies • Toxicology screen • CT • ETC.

Mental Status Change
• CXR: infectious/ pulmonary source • CT head: Ha, focal neurologic sx, • LP: Fever and Mental Status change with no identifiable cause.
• EKG: MI and Afib • Other Xray: trauma

Mental Status change
This should lead to a good working diagnosis and treatment plan.
Good Luck!!

Falls
Dean Yeropoli

Falls
• Expect to get a call from the floors (i.e. 5 North or 4 North) regarding a fall on almost every call
• Patients are typically elderly, so remember compounding factors (age, dementia, orthostatic hypotension, autonomic dysfunction, polypharmacy, sedatives, CAD, prior CVA with deficits, hypoglycemia, anemia, etc)
Falls
• First ask the nurse if the patient is hemodynamically stable
• Ask the nurse to check the patient’s blood glucose and a new set of vitals
• GO SEE THE PATIENT (IMMEDIATELY,if hemodynamically unstable)

Falls
• Find out from the patient and nurse the events surrounding the fall
• Find out where the patient is having pain • speak with any other witnesses to get as complete a picture as possible.
• Most patients will be elderly. Remember that their baseline mental status may be demented
• However, always rule out other possible causes of change in mental status if applicable

Falls • Perform a neurologic exam, including the level of consciousness and a head exam. Look for hematomas.
• If you have any concerns about head trauma or change in mental status, check a STAT CT of the head without contrast to rule out a bleed
• Is patient on anticoagulation (i.e. Coumadin, heparin drip, therapeutic LMWH)
• Check recent labs if applicable (EKG, telemetry monitor, etc.)
• Consider checking xrays for possible trauma

Falls
• Look at the medication list for possible contributing factors (sedatives, antihypertensives, hypoglycemic agents)
• Fill out an incident report and clearly document what occurred and what tests you performed.
• Notify the attending

Inam Khan, D.O.









Lili Poon, DO

It’s not a sign of impending doom, but it is temp that exceeds the patients normal daily temp range.
The best definition of a fever is a body symptom that requires attention.

Study of 25,000 healthy adults – checked axillary temps and found norm to be 37°C (98.6°F)
Axillary temp can be as much as 1°C (1.8°F) off from actual core body temp.
Diurnal variation of body temp: Nadir is in the early morning and peaks in the late afternoon.
The most accurate representation of core body temp is recorded from the pulmonary artery and urinary bladder.

It is the result of inflammatory cytokines (IL1, IL6, TNF) that act on the hypothalamus to increase the core body temperature. Do not confuse fever with hyperthermia. Hyperthermia is when the body temp is high because the body is not regulating the
temperature properly. Heat stroke. Antipyretics, such as aspirin or acetaminophen, reduce fever by decreasing
the hypothalamic set point through anti-prostaglandin effects, and are contraindicated. Fever tells us that the body’s temp regulatory system is intact but is just operating at
a higher set point for a reason. Fever enhances the immune system response by increasing production
of antibodies & cytokines, increasing T-cell activation, and enhances phagocytosis. The high temp is a less favorable environment for bacterial and viral replication
Fever is INFLAMMATION, not infection. Severity of fever is not indicative of presence or severity of infection. Febrile response: Body increases core temp by promoting peripheral
vasoconstriction and a generalized increase in muscle tone. This is the same thing that happens to the body in a cold environment….the body tries to keep its core temperature high.
Fever as defined by the Society of Critical Care Medicine: >38.3°C or 101°F
Noninfectious Drug induced Amphotericin, Cephalosporins, Penecillin, Phenytoin,
Procainamide, Quinidine, Cimetidine, Carbamazepine, Hydralazine, Rifampin, Streptokinase, Vancomycin
Infectious Procedure related (Hemodialysis, Bronchoscopy,
Blood transfusion, Postop)

Drug fever Transfusion reaction – stop transfusion and monitor
BP (give IVF and DA if needed) Adrenal insufficiency Thyroid storm Acalculous cholecystitis Pancreatitis Benign postoperative fever Benign post procedure fever (bronchoscopy,
hemodialysis) Thromboembolic disease Drug overdose (eg, aspirin anticholinergic drugs) Drug withdrawal (ETOH, Benzodiazepines)
Intracranial hemorrhage Seizures Heat stroke Neuroleptic malignant syndrome Malignant hyperthermia Pheochromocytoma Serotonin syndrome Malignancy Burns Gout Vasculitis Ischemic colitis Acute respiratory distress syndrome (late) Myocardial infarction

Pneumonia HCAP, CAP, VAP
Intravascular catheter related infection
Sepsis Surgical site infection Wind, Water, Wound
Urinary tract infection Sinusitis Empyema Intraabdominal Abscess
Endocarditis Suppurative
thrombophlebitis Cholangitis Pseudomembranous
colitis Diverticulitis Septic arthritis Cellulitis Myonecrosis Necrotizing fasciitis Meningitis

DO NOT JUST GIVE TYLENOL OVER THE PHONE! DO NOT USE A COOLING BLANKET TO TREAT FEVER! Ask what the current vitals are to determine whether the
patient is stable at this moment. Go see patient and do a complete ROS. Do a Physical Exam. Look through the chart. Admission diagnoses, current
problem list, are they on Abx? Is ID consulted? Check Current labs, Imaging studies, etc. Things you need to know: Admit Dx, How long has pt in the hospital, Lines/Catheters (foley, vascath, medports, PICC, etc.), Is the fever new? Cultures obtained during hospitalization Is this patient immunocompromised? (HIV, Chemo, S/P Transplant)

HEENT – sinusitis, pharyngitis, meningitis, LAD, conjunctivitis, oral lesions
SKIN – rash, open wounds, cellulitis, splinter hemorrhages, decubitus ulcers, examine all IV and catheter sites, open skin folds, large hematomas (after procedures)
LUNGS – decreased BS, crackles, rhonchi HEART – new murmur ABDOMEN – tenderness in RUQ, LLQ, periumbilical BACK – new pain, CVA tenderness RECTAL EXAM (NOT IN NEUTROPENIC PTS) – prostate
tenderness, perirectal abscess, skin break down (decubitus ulcers)
EXTREMITIES – edema, tenderness MUSCULOSKELETAL – joint pain, joint swelling

Blood Cx’s X2 (different sites) CBC w/ Diff Sputum Cx and gram stain UA & Urine Cx Wound Cx’s Stool Studies – C.Dif, WBC, Cx Lines (if they look infected or have been
present for a long time, change the line and culture the tip)

Common: CXR – look for infiltrates/consolidations
If localizing signs and symptoms are present: CT Scans Chest/Abd/Pelvis Acute Abd Series – look for fluid or free air TEE – look for vegetations on valves Lumbar Puncture –Meningitis Paracentesis – swollen tender abd…?SBP

Start IVF resuscitation and call your senior resident. Call code blue if you need to.
If you have a possible source of infection then make sure pt is on appropriate Abx.
Suspected line infections – remove/change line DOCUMENT , DOCUMENT, DOCUMENT

ANC < 500, panCx, start broad spectrum Abx monotherapy: cefepime, ceftazidime, zosyn, or
imepenem combination therapy: betalactam, or betalactam
with fluoroquinolone, or even a betalactam with an aminoglycoside
If not resolving after 5-7days then consider fungal infections and get an ID consult.

This is one case where antipyretic medications are needed
Higher temp means higher oxygen demand in the brain
Higher temp is also associated with higher production of toxic oxygen metabolites
These patients may already be on a hypothermia protocol


A 70 y/o man was admitted 11 days ago for STEMI & stent. His post-MI course has been complicated by moderate CHF requiring diuresis. You are called to evaluate the pt because of new onset fever to 38.5 o C. Possible sources of fever? Diagnostic W/U? Do we need empiric antibiotics?

Possible sources of fever? Non-Infectious: Dressler’s, DVT / PE, Drugs Infectious: CABSI, typhlitis, HAP, UTI
Diagnostic W/U? H&P EKG, CK/Trop-I, CXR, U/A + micro, BCx x 2, sputum GS /
C&S, Dopplers, CT-A
Empiric antibiotics? If above suggests infxn, cover nosocomial-MDR pathogens
Wrong way to evaluate fever is to culture everything, order a bunch of labs, and imaging studies, and starting antibiotics without hesitation.
Bedside evaluation is a must Not all fevers are due to infections Remember that hypothermia can be a “ominous
febrile equivalent” The Sanford guide is a helpful reference, but
a senior resident is better.

Pain Meds/Hypnotics
Samir Makati
112
• Temazepam (Restoril) 7.5 30 mg. • Zolpidem (Ambien) 5 10 mg. • Eszopiclone (Lunesta) 1 3 mg. • Lippincott’s Illustrated Reviews: Biochemistry 4 th Edition. • Have Dr. Scrocco tell the patient one of his famous “to make a long story short” stories.
• Teach the patient how to meditate. “A ruffled mind makes a restless pillow.” – Charlotte Bronte.
• Use lower dose in the elderly.
Sleep

113
• Look for underlying causes and treat. – Pain – Respiratory distress – Mental status change – Drug withdrawal
• Lorazepam (Ativan): PO or IV. • Haloperidol. • May require bed check, sitter, restraints.
Agitation/Anxiety

114
• Evaluate for and treat underlying causes. • Check renal and hepatic function. • Check vitals (BP), mental & respiratory status. • Look for contraindications. • Routes of Administration: PO/IM/IV/PR/Trans dermal.
Pain
115
• PO: – Tylenol – NSAIDS (ibuprofen, naproxen, etc.) – Tylenol 3 – Tramadol – Vicodin – Percocet – Morphine – Oxycodone
• IV: – Toradol – Morphine – Dilaudid
• Fentanyl patch
Pain

116
• Longacting: – MS Contin – Oxycontin
Pain

117
• Red Flags: – History of substance abuse. – Patient frequents multiple hospitals. – Patient knows specific names of pain meds. – Patient asks for IV med to be pushed through closest IV port and to be pushed faster.
– Loosing prescriptions/calling for refills sooner than should be necessary.
– Patient not interested in following through on other recommendations to get better (stop smoking, do physical therapy, etc.).
Pain med abuse
118
• Review progress notes and notes in ECW. • Patients with substance abuse still can become ill and have legitimate pain. – Rule out organic causes of pain each time patient presents.
– Palpation with auscultation. • Offer resources to patient to help against addictive behavior.
Pain med abuse

119
Thank you.

Pronouncing Death
Aashi Singh July 1,2008

Things to do First…
• Make sure the patient is actually dead. • Don’t tell the family the patient is dead when they are actually alive.
Physical Exam
• Call name loudly. • Sternal rub, nail pressure, axillary pinch. • Feel for carotid pulse. • Listen for heart tones, breath sounds. • Examine pupils for size and reactivity.

Death Note Identify the patient name, age, admit Dx.
• Pt did not respond to verbal or noxious stimuli. • Pt did not have palpable pulse or audible heart tones. • Pt did not have spontaneous respirations or breath sounds. • Pt had fixed and dilated pupils.
(Pt name) was pronounced dead at (Hospital), (City, State), by (resident) at (military time, date).
Family was present (have been contacted) and is (are) aware. (Admitting Physician) was notified and will sign death certificate. The coroner has declined(accepted) this case for autopsy.
Who do you call?
• PCP • Coroner • Family
What the Coroner will Ask • Name • SSN • Phone • Co morbidities • Next of Kin (NOK) • NOK Address • Physician for death
certificate
Coroner: 3306432101
• DOB • Address • Dx • Invasive Procedures • NOK Phone • Funeral Home • Manner of death, Code
Status
DOM Paperwork
• Complete Internal Medicine Death Packet should be available at every nursing station.
• Return to Chief Resident.
Recommended