The role of imaging
to assist CTO-PCI
Gerald S. Werner, MD PhD FESC FACC FSCAI
Medizinische Klinik I
Klinikum Darmstadt GmbH

Imaging for CTO PCI
• Planning before the procedure
• Plaque composition
• Primary choice of strategy
• Analysis of problems with wire advancement
• Guidance in the cath lab
• Visualization of the wire pathway
• Optimization of viewing angles

20 years Post CABG: Ostial RCA CTO
What is the best strategy ?
Retrograde options are challenging

Moderate calcification -> medium-strengh wire

Occluded RCA: Value of MSCT

CTO
CT-scan shows details of the occluded segment

Reference-image“ from CT serves as
navigation support for the cardiologist
Segmentation Intra-op Planning Registration CT/C-Arm Side by side Guidance

The reference gives certainty for the wire advancement
without any other landmark

… and supports the successful recanalization of the
CTO in this case

An example from 2014 (Riga CTO Day)

An example from 2014 (Riga CTO Day)

An example from 2014 (Riga CTO Day)

MDCT analysis of plaque composition
Choi JH et al. Circulation Journal 2011; 75: 366-75 from Seoul, Korea
186 pats with MDCT, 77% success
Plaque density increases with
duration of CTO
Higher HU in failed PCI for CTO

Imaging for CTO PCI
• Planning before the procedure
• Plaque composition
• Primary choice of strategy
• Analysis of problems with wire advancement
• Guidance in the cath lab
• Visualization of the wire pathway
• Optimization of viewing angles

H IM AX IN NC Andreas Meyer
CT Segmentation of coronaries

H IM AX IN NC Andreas Meyer
Angio-CT co-registration

H IM AX IN NC Andreas Meyer
Planning based on co-registered CT
Crossectional view
Longitudinal view

H IM AX IN NC Andreas Meyer
Reference-image from CT follows all movements of C-arm and table
Segmentation Intra-op Planning Registration CT/C-Arm Side by side Guidance
Colouring of centerline indicates foreshortening in relationship to C-arm position

H IM AX IN NC Andreas Meyer
CT-reference serves as navigation support

H IM AX IN NC Andreas Meyer
Successful recanalization of the CTO

Set up in the cath lab
IVUS
MSCT
INTEGRATE

Number of MSCTs for CTO-PCI in my institution
0
50
100
150
200
250
300
2009 2010 2011 2012 2013 2014
MSCT
No MSCT
• Main indication for preprocedural MSCT
• Long ambiguous CTO of the RCA
• Poor visualization of an occluded vessel via
collaterals
• Previously failed procedure

LAD CTO: Where is the proximal cap ?

LAD CTO: Where is the proximal cap ?

LAD CTO: Where is the proximal cap ?
Pullback from distal vessel…

LAD CTO: Where is the proximal cap ?
• An occluded vessel
ostium is a solid structure
• There is a considerable
step-up in vessel size

LAD CTO: Where is the proximal cap ?

LAD CTO: antegrade wire for Rx CART

LAD CTO: Where is the proximal cap ?

IVUS in CTOs
• IVUS in the antegrade approach
• Identify the proximal cap
• Verify true lumen entry
• Try to guide reentry into true lumen
• Verify true lumen position after reentry
• IVUS in the retrograde approach
• Identify issues with hampered retrograde wire
• IVUS guided reverse CART
• Mandatory when approaching left main
• IVUS to optimize stenting in diffusely diseased CTOs
• What is the true vessel size
• How extensive should we cover the vessel by stents
• Can we leave a bifurcation or should we treat it

IVUS in CTOs
• IVUS in the antegrade approach
• Identify the proximal cap
• Verify true lumen entry
• Try to guide reentry into true lumen
• Verify true lumen position after reentry
• IVUS in the retrograde approach
• Identify issues with hampered retrograde wire
• IVUS guided reverse CART
• Mandatory when approaching left main
• IVUS to optimize stenting in diffusely diseased CTOs
• What is the true vessel size
• How extensive should we cover the vessel by stents
• Can we leave a bifurcation or should we treat it

RCA CTO: Strategic options
• Retrograde access
possible
• How likely is it to
pass the retrograde
wire all the way up?
• Antegrade wire
position required
• Antegrade wire
• No entry
• IVUS analysis to inquire
the proximal cap

RCA CTO: Strategic options

Puncture of the cap with Gaia 2

Then via Finecross wire downgraded

Stent placement, the real challenge

Bifurcation is covered with single stent

Complex long RCA CTO

Intramural hematoma and collapsed true lumen

Successful puncture into true lumen

Complex long RCA CTO

IVUS in CTOs
• IVUS in the antegrade approach
• Identify the proximal cap
• Verify true lumen entry
• Try to guide reentry into true lumen
• Verify true lumen position after reentry
• IVUS in the retrograde approach
• Identify issues with hampered retrograde wire
• IVUS guided reverse CART
• Mandatory when approaching left main
• IVUS to optimize stenting in diffusely diseased CTOs
• What is the true vessel size
• How extensive should we cover the vessel by stents
• Can we leave a bifurcation or should we treat it

Date of download:
1/18/2014
Copyright © The American College of Cardiology.
All rights reserved.
From: Fundamental Wire Technique and Current Standard Strategy of Percutaneous Intervention for Chronic
Total Occlusion With Histopathological Insights
J Am Coll Cardiol Intv. 2011;4(9):941-951. doi:10.1016/j.jcin.2011.06.011
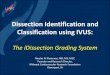
Principle of Retrograde Subintimal Tracking
Antegrade subintimal tracking (dotted line) and retrograde subintimal tracking (solid line). Even though the angiogram shows that
the 2 wires are separated (antegrade and retrograde), both wires can be positioned in the same subintimal space. After the
retrograde wire comes into the same lumen with the antegrade wire, crossing into the proximal true lumen with the retrograde wire
is highly promising.
Figure Legend:

Long RCA occlusion in a 51 year old male

Reverse CART, wire does not pass
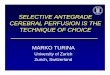
Romberg

Identify the wire inside the plaque
32577
• Retrograde wire within a
plaque formation
• Antegrade IVUS subintimal

Identify the wire inside the plaque
32577
• Retrograde wire reaching
the plane of the antegrade
wire/IVUS position
• Antegrade IVUS subintimal

Identify the wire inside the plaque
32577
• Retrograde wire reaching
the plane of the antegrade
wire/IVUS position
• Antegrade IVUS subintimal

Identify the wire inside the plaque
32577
• Antegrade IVUS intraluminal
• Retrograde wire exiting again
into massive proximal plaque

Proximal plaque needs to be expanded…

Long RCA occlusion in a 51 year old male

IVUS in CTOs
• IVUS in the antegrade approach
• Identify the proximal cap
• Verify true lumen entry
• Try to guide reentry into true lumen
• Verify true lumen position after reentry
• IVUS in the retrograde approach
• Identify issues with hampered retrograde wire
• IVUS guided reverse CART
• Mandatory when approaching left main
• IVUS to optimize stenting in diffusely diseased CTOs
• What is the true vessel size
• How extensive should we cover the vessel by stents
• Can we leave a bifurcation or should we treat it

What is the real long-term benefit
• Everyone who uses IVUS knows that we
underestimates the real vessel size despite
experience
• We can optimize stent coverage and
expansion by IVUS
• I am convinced that proper use of IVUS
guidance will be superior to angiography, …
• … but we need to prove it by a RCT

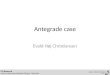
ECC 2014: IVUS diversity in CTOs
0
20
40
60
80
100
120
140
160
180
200
220
240
260
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35
IVUS
No IVUS
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35
IVUS
NO IVUS

Imaging for CTO PCI
• Imaging helps to plan and perform CTO PCI
• No one should perform CTO PCI in complex
lesions without IVUS in the lab
• IVUS image interpretation is not trivila and
requires training and experience
• MSCT is a valuable planning tool in long
lesions with no or little calcium in the course
of the lesion
• In selected cases, coregistration may improve
the procedure
58
Recommended