The Post-Clerkship Curriculum: A Lost Opportunity
THE GENERALIST IN MEDICAL EDUCATION MEETINGSunday, 11/8/2015, Baltimore (Hotel Monaco)
10:45-12:15pm (Problem Solving Session)

The Post-Clerkship Curriculum: A Lost OpportunityNicholas Kman MD: Academic Program Director, Part 3/Fourth Year Curriculum, The Ohio State University College of Medicine
Paul Ko MD: Interim Associate Dean for Undergraduate Medical Education, SUNY Upstate Medical University, Syracuse, NY.
Rahul Patwari MD: Assistant Dean for the Post-Clerkship Curriculum, Rush Medical College, Rush University, Chicago, IL
Kim Askew MD: Director, Clinical Curriculum, Wake Forest School of Medicine, Winston-Salem, NC
NO DISCLOSURES

Introductions
What is your institution, specialty and role in
education?

Objectives▪ Describe the building blocks of the 4th year of
medical school and how these can be used to prepare students for residency.
▪ Share common barriers students and educators face in the fourth year.
▪ Describe how a clinical track, boot camp or longitudinal curriculum based on competencies could bridge the chasm between UGME and GME.

Exercise 1 (10 minutes)
What does your 4th year of medical school look like?
Required Courses?
Electives?
Bootcamps?
Structure?

Arguments Against the 4th Year

What do we get for that extra year?
“A chance to travel about the country or engage in audition
electives.”Petersdorf 1990
a “year of drift, lax evaluations and passive absorption” where
students are allowed “great latitude in their choices with few constraints” and the “offerings
among departments are not coordinated.” Barzansky 2001
Flexner report (1910): medical training was 4 years,
now 7-10 years
student maturation enrich medical education
experiencestime for residency application
avoid student & faculty burnoutcomplexity of medicine
increasing

What can we do in 3/4th the time?
Eliminate one year of debt
Incentive to enter primary care
Faster turnover of physicians
Link UME and GMECompetency-based, flexible, learner centered
Abramson, S. B., Jacob, D., & Rosenfeld, M. A 3-year MD—accelerating careers, diminishing debt. New England Journal of Medicine. Sep 19, 2013Raymond, J. R., Sr, Kerschner, J. E., Hueston, W. J., & Maurana, C. A. (2015). The Merits and Challenges of Three-Year Medical School Curricula. Academic Medicine, 90(10), 1318–1323.

Eliminate one year of debt
▪ One less year of medical student tuition$10k’s savedMakes medical school more accessible to othersLet’s students consider lower paying specialities
▪ One more year of physician compensation▪ One more year to pursue interests outside medicine
Masters

Faster turnover of physicians
▪ World War II (1944)By reducing the length of the summer holiday, it is possible, without altering the
actual weeks of instruction, to complete the present curriculum in three calendar years… Sidney Burwell responding to the physician shortage of WWII
▪ Comprehensive Health Manpower Training Act (1971)
25% med schools had 3 year programs
▪ Projected physician shortage of 46,000 to 90,000 (2025)
▪ Age creephttps://www.aamc.org/download/426260/data/physiciansupplyanddemandthrough2025keyfindings.pdf
http://repository.countway.harvard.edu/xmlui/handle/10473/1784?show=fullhttp://uscode.house.gov/statutes/pl/92/157.pdf
https://www.washingtonpost.com/national/health-science/medical-school-done-faster/2014/01/13/4b6d9e54-5c40-11e3-be07-006c776266ed_story.html

Incentive to enter primary care
▪ Mercer University School of MedicineAccelerated Family Medicine Track
▪ University of California Davis + Kaiser PermanenteAccelerated Competency-Based Education in Primary Care
▪ Louisiana State UniversityLouisiana state residents (more likely to practice in underserved areas)
▪ New York UniversityNo restrictions, but slots allocated in local programs
▪ Texas Tech UniversityFamily Medicine Accelerated Track
▪ Medical College of WisconsinPreference for those from underserved communities
▪ Lake Erie College of Osteopathic MedicinePrimary Care Scholars Pathway
Bell HS1, Ferretti SM, Ortoski RA. “A three-year accelerated medical school curriculum designed to encourage and facilitate primary care careers.” Acad Med. 2007 Sep;82(9):895-9.

Link UME and GME
▪ Three programs will likely need to be competency-based
Accelerated Family Medicine Track▪ Columbia University
Four students for PhD students▪ Pediatrics Across the Continuum project
UCSF, U of Colorado (Denver), U of Minnesota, U of UtahEPA’s and Competencies
▪ Lake Erie College of Osteopathic MedicineAccelerated Physician Assistant Pathway

Can we teach medicine in 3 years?Core Curriculum in three years
▪ Duke University School of Medicine:M3-M4: electives and research
▪ University of PennsylvaniaM4: 36 weeks of flexible time and scholarly training
▪ Harvard’s New Integrated Curriculum carvesM4: advanced experiences in clinical medicine and basic science,
a scholarly capstone project, electives, and a subinternship

Can we teach medicine in 3 years?The whole thing in 3 years, eh? For the past 40 years.
▪ McMaster UniversityMichael G. DeGroote School of MedicineEqual or better competence (than Canadian or US 4-year schools)More likely to pursue academics
▪ University of CalgaryCumming School of MedicineHigher satisfaction (compared to Alberta)Equal or better competence
Lockyer J1, Violato C, Wright B, Fidler H, Chan R.. “Long-term outcomes for surgeons from 3- and 4-year medical school curricula.” Can J Surg. 2012 Aug;55(4):S163-70. doi: 10.1503/cjs.37610. http://www.ncbi.nlm.nih.gov/pubmed/22854154 Lockyer JM1, Violato C, Wright BJ, Fidler HM. “An analysis of long-term outcomes of the impact of curriculum: a comparison of the three- and four-year medical school curricula.” Acad Med. 2009 Oct;84(10):1342-7. doi: 10.1097/ACM.0b013e3181b6c08e.

Arguments For the 4th Year

Lyss-Lerman P, et al. What training is needed in 4th year of medical school? Views of residency program directors. Acad Med. 2009 Jul;84(7):823-9. ▪ Common struggles of interns:
▪ Lack of self-reflection and improvement▪ Poor organizational skills▪ Underdeveloped professionalism▪ Weak medical knowledge
▪ Competencies MS IV students should gain before starting residency▪ Advanced clinical reasoning▪ Near intern level independence▪ Ownership of patient care
16

Lyss-Lerman P, et al. What training is needed in 4th year of medical school? Views of residency program directors. Acad Med. 2009 Jul;84(7):823-9.
▪ “Organizing the curriculum with specialty-specific tracks could be explored by looking at specialty-specific data and expanding the interviews to include more PDs.”
17

Walling A, Merando A. The fourth year of medical education: a literature review. Acad Med. 2010 Nov;85(11):1698-704.
▪ Three recurring themes:▪ Lack of clarity about the educational purpose▪ Problems in curricular content and organization▪ Concerns about the educational quality of courses
18

Walling A, Merando A. The fourth year of medical education: a literature review. Acad Med. 2010 Nov;85(11):1698-704.
▪ ACGME policies and practices will increasingly influence medical student education
▪ 4th year as capstone for medical school versus preparation year for residency
▪ Turned in favor of the pre-residency viewpoint▪ Other factors that increase the pressure towards using
the fourth year to prepare for residency are student debt and the growing specter of unmatched US graduates
19

What is the 4th Year? What Can it Be?
20

Reddy ST, et al. ACE perspective paper: recommendations for redesigning the "final year" of medical school. Teach Learn Med. 2014;26(4):420-7.
▪ Demonstrate that they have mastered objectives (based on 6 ACGME Core Clinical Competencies)
▪ Complete a required capstone course prepares students for residency.
▪ Structure their 4th year schedules to accomplish specialty-specific objectives that prepare them for their intended specialty.
▪ Engage in thoughtful inventory of training. Identified gaps should be addressed through deliberate participation in rotations that address identified areas.
21

Reddy ST, et al. ACE perspective paper: recommendations for redesigning the "final year" of medical school. Teach Learn Med. 2014;26(4):420-7.
▪ Demonstrate that they have mastered objectives (based on 6 ACGME Core Clinical Competencies)
▪ Complete a required capstone course prepares students for residency.
▪ Structure their 4th year schedules to accomplish specialty-specific objectives that prepare them for their intended specialty.
▪ Engage in thoughtful inventory of their medical school training. Identified gaps should be addressed through the deliberate participation in rotations that address the identified areas.
22

Reddy ST, et al. ACE perspective paper: recommendations for redesigning the "final year" of medical school. Teach Learn Med. 2014;26(4):420-7.
▪ 4th year is a bridge between medical school and Residency: ACGME Competencies and AAMC Core Entrustable Professional Activities (EPAs) should be used to guide curriculum development.
▪ These competencies and specialty-specific milestones and EPAs provide guidance to medical schools for the minimum level of competency for starting intern and can be used to design 4th-year curricula.
23

Chen HC, van den Broek WE, ten Cate O. The case for use of entrustable professional activities in undergraduate medical education. Acad Med. 2015 Apr;90(4):431-6
▪ Specialty-specific EPAs could guide student selection of senior year electives as well as help program directors ensure a baseline competency level of their entering residents.
▪ If operationalized properly, these specialty-specific EPAs could ease advising during the fourth year, ensure more adequately prepared entering residents, and obviate the need for extracurricular “boot camps”
24

Exercise 2 (10 minutes)
What are some of the perceived gaps in training or
weaknesses of the 4th year at your school?
How could you improve these weaknesses?

Review of our schools

The current M4 year can be as short as 26 weeks long.
As much as 5 months off.
Sub-
Inte
rnsh
ip
Emer
genc
y M
edici
ne
Flex
A
Flex
A
Flex
A
Flex
A
Flex
B
Flex
B
Elec
tive
Elec
tive
Elec
tive
M3
Elec
tive
M3
Elec
tive
M3
Elec
tive
M1
Elec
tive
M1
Elec
tive
36 weeks
5/9/
2016
5/23
/201
6
6/6/
2016
6/20
/201
6
7/5/
2016
7/18
/201
6
8/1/
2016
8/15
/201
6
9/26
/201
6
10/1
0/20
16
8/29
/201
6
9/12
/201
6
10/2
4/20
16
11/7
/201
6
11/2
1/20
16
12/5
/201
6
1/3/
2017
1/16
/201
7
1/30
/201
7
2/13
/201
7
3/27
/201
7
4/10
/201
7
2/27
/201
7
3/13
/201
7
12/1
9/20
16Ho
liday
s
48 weeks
26 weeks
The M4 year is currently set up as a 48-week long experience. Students have about 36 weeks of requirements toward graduation.
● 4 weeks of Sub-Internship● 4 weeks of Emergency Medicine● 28 weeks of electives including
○ 8 weeks of Flex A (“medicine specialties”)
○ 4 weeks of Flex B (“surgical specialties”)
○ 2 weeks clinical bridge
Students have the ability to take 4 weeks of electives in M1 and 6 weeks in the M3 year, thus shortening the M4 year to 26 weeks.
There are a few restrictions during the year:
● no more than 8 weeks in any particular discipline
● no more than four 2-week electives

48 weeks
5/9/
2016
5/23
/201
6
6/6/
2016
6/20
/201
6
7/5/
2016
7/18
/201
6
8/1/
2016
8/15
/201
6
9/26
/201
6
10/1
0/20
16
8/29
/201
6
9/12
/201
6
10/2
4/20
16
11/7
/201
6
11/2
1/20
16
12/5
/201
6
1/3/
2017
1/16
/201
7
1/30
/201
7
2/13
/201
7
3/27
/201
7
4/10
/201
7
2/27
/201
7
3/13
/201
7
12/1
9/20
16
Students get financial aid only for the time that they are enrolled. Those students with a 26 week M4 year, won’t get living expenses for the time they are not enrolled.
Financial aid will only be disbursed on or after the first day of each semester as long as students are enrolled in a class on that date. If they start afterward, they get their money on that later date.
Half the year’s coursework needs to be done in each half. Students cannot front load their schedules so they can finish early. If they do, their disbursement will be effected for the lighter semester.
Also there cannot be a 45-day block where they aren’t engaged in the curriculum. If a student takes 2 months off for interviewing, they won’t get financial aid for that time.
Half the coursework needs to be done in the first half of the academic year. The money will be disbursed on the
first day they’re enrolled in this block (on or after 5/9).
The other half of coursework needs to be done in the second half of the
year. Money will be disbursed on the first day they’re enrolled (on or after
10/24).
45 days off
Challenges of Financial aid regulations Students may not get financial aid if their M4 year is imbalanced.
Also RMC will need to follow the University Calendar and switch away from weeks credit to credit hours. Luckily, one week is roughly equivalent to 1 credit hour. Half the year’s credit hours will need to go in the first semester and half will need to be in the second half. Students will also need to be enrolled on the first day of each semester.
These
regulations are
what prompted
us to make the
Transition To
Residency Course.

The proposed M4 Year Requirements, Selectives, Clinical Electives, Electives and EPA’s.
Students will need guidance in constructing their schedule to ensure they
● put half course load in each semester (22 weeks in each 24 week semester)
● enroll in something on each semester’s start date
● have no 45-day blocks of non-enrollment
In addition to the current required courses (Sub-Internship, Emergency Medicine and Clinical Bridge which is now 4 weeks), students will need to complete:
● 12 weeks of Selectives● 8 weeks of Clinical Electives ● 8 more weeks of any Elective● 2 weeks of application and
board prep (1st semester)● 2 weeks of interview
preparation (2nd semester) + 2 more as a free elective, if needed
Sub-
Inte
rnsh
ip
Emer
genc
y M
edici
ne
Clin
ical E
lect
ive
Elec
tive
Appl
/Boa
rd P
rep
48 weeks
Clin
ical
Brid
ge
Clin
ical E
lect
ive
Clin
ical E
lect
ive
Clin
ical E
lect
ive
Elec
tive
Elec
tive
22 credit hours in 24 weeks
22 credit hours in 24 weeks
Inte
rvie
w/El
ectiv
e
Sele
ctiv
e 1
Sele
ctiv
e 2
Sele
ctiv
e 3
Elec
tive
5/9/
2016
5/23
/201
6
6/6/
2016
6/20
/201
6
7/5/
2016
7/18
/201
6
8/1/
2016
8/15
/201
6
9/26
/201
6
10/1
0/20
16
8/29
/201
6
9/12
/201
6
10/2
4/20
16
11/7
/201
6
11/2
1/20
16
12/5
/201
6
1/3/
2017
1/16
/201
7
1/30
/201
7
2/13
/201
7
3/27
/201
7
4/10
/201
7
2/27
/201
7
3/13
/201
7
Inte
rvie
w Pr
ep
12/1
9/20
16Ho
liday
s
Clin
ical E
lect
ive

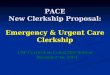
Entrustable Professional ActivitiesWe’ll organize the M4 year around the 13 AAMC’s Core EPA’s for Entering Residency (CEPAER)
Over the course of the Sub-Internship, Emergency Medicine and the three Selectives, students should complete each of the 13 EPA’s. An example distribution is seen below:
Core Entrustable Professional Activities for
Entering Residency01. Perform an H&P02. Make a DDx03. Select & interpret Dx tests04. Orders and treatment05. Documentation06. Oral presentations07. Use literature to answer questions08. Handovers09. Interprofessional teamwork10. Recognize patients requiring urgent intervention11. Obtain informed consents12. Perform simple procedures (IV, NG, venipuncture)13. Patient safety & QI
09 -
Inte
rpro
f Te
am
08 -
Hand
over
s
10 -
Urge
ncie
s
07 -E
BM
Sub-
Inte
rnsh
ip
Emer
genc
y M
edici
ne
Sele
ctiv
e 1
Sele
ctiv
e 2
Sele
ctiv
e 3
Clin
ical
Brid
ge
09 -
Inte
rpro
f Te
am
01 -
H&P
08 -
Hand
over
s
03 -
Dx Te
sts
02 -D
Dx
10 -
Urge
ncie
s
05 -
Docu
men
tatio
n
06 -P
rese
ntat
ions
12 -
Proc
edur
es
11 -C
onse
nts
07 -E
BM
13 -Q
ualit
y/Sa
fety
04 -O
rder
s & T
x
Even
tual
ly u
sed
to
test
all
EPA’
s
Holid
ays

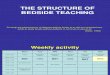
A sample scheduleFor a student who wants to match in Orthopedics.
She can take three ortho electives (all for credit) and still have a robust fourth year. There is time for interviewing. All EPA’s are assessed (and successfully completed).
Sub-
Inte
rnsh
ip
Emer
genc
y M
edici
ne
Pulm
onar
y
Thor
acic
Surg
ery
Card
iolo
gy
Clin
ical
Brid
ge
09 -
Inte
rpro
f Te
am
01 -
H&P
08 -
Hand
over
s
03 -
Dx Te
sts
02 -D
Dx
10 -
Urge
ncie
s
05 -
Docu
men
tatio
n
06 -P
rese
ntat
ions
12 -
Proc
edur
es
11 -C
onse
nts
07 -E
BM /
Qual
ity
13 -Q
ualit
y/Sa
fety
04 -O
rder
s & T
x
Disa
ster
Med
icine
Orth
oped
ics
Away
Orth
oped
ics
Away
Orth
oped
ics
Appl
/Boa
rd P
rep
Inte
rvie
w Pr
ep
Holid
ays
Inte
rvie
w Pr
ep
Disaster
Medicine, and
Interview prep
taken together
to allow time for
interviews.

Short, 1-page form
covering 2 EPA’s
How do we evaluate EPA’s

33
Medical Knowledge and
Skills
Practice and Lifelong Learning
Interpersonal Communications
Systems Based Practice
Professionalism
Patient Care
Medical Knowledge and Skills
Ohio State Old Curriculum 2 + 2 Approach

34
Part ThreeAdvanced
Clinical Management
4 Years18 months 12 months 13 months
Longitudinal ProjectsLife-Long Learning/Reflection
LongitudinalHealth Coach
CommunityHealth
EducationPatientSafety

PARTAdvanced Management inHospital Based CareAdvanced Management in Relationship Centered Care
Advanced Competency Elective
Clinical Tracks: A longitudinal experience in a specialty or subspecialty designed to prepare students to be an intern/incoming resident by meeting entry level milestones in that field.
Other Electives (4 total required including Advanced Competency)
Flex
Gateway Activities
Part ThreeAdvanced
Clinical Management
HSIQ Project

Hallmarks of L.S.I. Curriculum▪ Reinforce foundational science throughout curriculum▪ Early clinical service-learning experiences▪ Faculty coaching▪ Mastery based evaluations▪ Building Entrustment on all 13 EPA’s▪ Preparing for residency through increased patient care and working toward Milestones with
Clinical Tracks
36

Solution: Clinical Tracks!
37

38
College structure – 6 UCLA collegesAcute Care: time-based decision-making specialties(Anesthesia, critical care EM)
Applied Anatomy: structure-oriented fields (Surgery, radiology, pathology)
Medical Leadership: dual-degree programs in public health or business administration
Medical Subspecialties: subspecialties focused on clinical reasoning and advance fellowship training
Primary Care: longitudinal care specialties (FM, IM, pediatrics)
Urban Underserved: focuses on care of underserved communities

Clinical Track▪ Framework for 4th year medical school “curriculum” that
aligns UGME and GME such that the medical student is working toward entry level milestones (ACGME milestones) to prepare them for their intern year in specialty of choice.
▪ Composed of a conglomeration of experiences (required courses, electives, advanced competencies, bootcamps) the student has during 4th year to prepare them for internship.

Clinical Track▪ Reached out to departments that housed residency
programs that students commonly match into to develop the initial tracks
▪ Develop curricular content▪Advanced Topics Courses▪Required and recommended rotation (s)
▪ Develop evaluation method- ideally competency based using selected entry level milestones
▪ Choose faculty lead for the track

List of current tracks▪ Anesthesia▪ Emergency Medicine▪ Family Medicine▪ Internal Medicine (Preliminary medicine, IM-Peds included)▪ Obstetrics/Gynecology▪ Pediatrics▪ Psychiatry▪ Neurology▪ Radiology▪ Surgery/Surgical Subspecialties

How long should a track be?▪ A clinical track is not a set number of rotations but a
combination of different rotations/experiences that will allow the student to develop skills to become a proficient intern in that field
▪ Recommendations for rotations for the required components of part 3
▪ Recommendations for electives ▪ Required rotations
▪Advanced topics courses

What is required?▪ Each department/division creating the track would decide
what is required in order for students to complete the track
▪ Specialty specific scheduling guide (SSSG)- recommendations for required and elective rotations put together by departments/divisions to guide students on what to take during fourth year to prepare them for a particular field

Ex of SSSG
2. Emergency Medicine Clinical Track (Revised 2/9/2015)
AMHBC: EMERGENCY MEDICINE: Emergency Med at OSU.AMRCC: CHRONIC CARE COMPONENT Geriatrics, HIV Patient Care, Congestive Heart Failure, Adult Kidney Disease, Child Abuse/Child Advocacy, Alcohol and other Drug Abuse.AMHBC: MINI INTERNSHIP: MICU, Cardiology, Pulmonary. Electives: Advanced Topics in Emergency Medicine (ATEM: Honors Longitudinal EM Elective), Advanced Competency in Ultrasound, Advanced Competency in Emergency Preparedness, Radiology, Anesthesia, Sports Medicine, Dermatology, Surgical specialties in general, including Plastics, ENT/Ophtho (two 2-week electives if possible), Hand Surgery, Orthopedics.
Special Requirements: Away Electives in EM only at places where you may want to match. Students interested in Emergency Medicine should schedule their AMHBC: EMERGENCY MEDICINE at OSU in July, August or September.
Busiest interview months to consider for flex months are November through January
Residency Directors: Sorabh Khandelwal (Director), Jillian McGrath, Sarah Greenberger, Laura Thompson, Andy King.Faculty Advisors: Dan Martin, David Bahner, Nick Kman, Mark DeBard, Ash Panchal, Creagh Boulger, Cynthia Leung.

How are students evaluated?
▪Competency based assessments▪ Ideally- the departments/divisions who
created the tracks would select a subset of the ACGME milestones for that field that students would be evaluated on
▪Students would have “completed” the track if they achieve the selected milestones


List of medical student milestones assessed during an expert educator shift.
47
Milestone DescriptionRecognizes abnormal vital signs.Recognizes when a patient is unstable requiring immediate intervention.Performs and communicates a reliable, comprehensive history and physical exam.Performs and communicates a focused H&P which effectively addresses the chief complaint and urgent patient issues. Constructs a list of potential diagnoses based on chief complaint and initial assessment.Formulates basic diagnostic and therapeutic plans based on a differential diagnosis.Establishes rapport with and demonstrates empathy toward patients and their families.Demonstrates behavior that conveys caring, honesty, patient confidentiality, genuine interest and tolerance when interacting with a diverse population of patients and families.
Demonstrates basic professional responsibilities such as timely reporting for duty, appropriate dress, conference attendance, and timely completion of clerkship documents.
Effectively listens and communicates with patients and their families.

March Into ResidencyA 4th year Bootcamp Course



Capstone Courses• 80 of 136 schools required it (59%)• Variable setting/structure• Towards end of 4thyear• Duration: Longitudinal, several days to 4
weeks• Outcome Data on these courses are limited


March into Residency Course• 4 weeks in length• General Topics for ALL 4th year students (n=160)• Goals & Objectives
– Utilizing the Institutional Graduation Competency and Educational Program Objectives
– 13 AAMC Entrustable Professional Activities– Prepare students to be ready to be an intern and
potential topics they would face on the ‘First Day of Internship/Residency’

Course Focus• Generalist vs Specialist training
– Majority of content targeted to general medicine/surgery regardless of specialty
– Breakout Specialty specific Days for specialty training (3 days total)
• Surgical Bootcamp• OB/GYN Bootcamp• Psychiatry Bootcamp• Pediatrics Bootcamp

Format• 25 minute lectures• Small Group Case Based Session (8x 1.5 hour
sessions based on lecture topics)• Procedure/Skills Sessions• Panel Discussions• Online Self-Study Modules

Lecture/Small Group Topics• ACS• Pulmonary Embolism• Aortic Dissection• Delirium• Dementia• Intoxication• Psychosis• Seizures• Stroke• Meningitis/Encephalitis• Shock
• CHF• Pneumonia• Asthma• COPD• Ventilators• Electrolytes/DKA• General Infections
• Appendicitis• Mesenteric Ischemia• Cholecystitis• GI Perforations

Specialty Topics Covered• Prescription Writing• Pharmacology Panels/Opioid Safety• Radiology Sessions• EKG Sessions• Resident Panel• Bioethics Issues in Residency• Health Care Reforms/Health Economics• Social Media in Residency• Wellness/Burnout Issues

Procedure Sessions• Lumbar Puncture• Central Line• Suturing• IV Insertion• Airway Management

Considerations• Faculty Resources• General versus Specialty Specific Preparation
– Specialty specific Milestones– AAMC EPA
• Assessments of EPAs in the course• Student Buy-in

Wake Forest School Of Medicine: Senior Seminar
Graduating Medical Student
Intern

Wake Forest School Of Medicine: Senior Seminar
• 2 weeks in duration• Combination of Different Topics:
– General Topics Applicable to all Careers– Speciality Specific Sessions– Elective Sessions to Promote Personal Development
• Goals and Objectives– Based on Institutional Objectives/Competencies,
Entrustable Professional Activities and Milestones

Format
• Continuing Medical Education Conference Format
• Variety of sessions formats based on content– Small group discussion– Simulation events– Panel Discussions– Procedure/Skills Laboratories

Speciality Specific Days
• Students work in groups with peers entering similar intern year.
• Topics addressed have content specific to specialty

Procedures
• Basic and Advanced Procedures in Year III and IV of curriculum
• Additional exposure, practice for advanced procedures– Incorporation of ultrasound– Speciality specific skills/procedures

Intern as Teacher
Workshops on addressing tools for expanding role of teaching

Considerations
• Similar to SUNY Upstate– Faculty resources– Equipment– Student Buy-in
• Improved with Student Selection of Topics in Conjunction with Required Sessions
• Logistics!!!!

Generalist vs Specialist

Exercise 3(20 minutes)
Develop your ideal/prototype 4th year curriculum:
What will it look like?
Share with the entire group at the end

References▪ Wolf, S J (02/19/2014). "Students' Perspectives on the Fourth Year of Medical School: A Mixed-
Methods Analysis". Academic medicine (1040-2446), p. 1. ▪ Cosgrove, E M (02/19/2014). "Empowering Fourth-Year Medical Students: The Value of the Senior
Year". Academic medicine (1040-2446), p. 1.▪ Reddy ST, Chao J, Carter JL, Drucker R, Katz NT, Nesbit R, Roman B, Wallenstein J, Beck GL. Alliance
for clinical education perspective paper: recommendations for redesigning the "final year" of medical school. Teach Learn Med. 2014;26(4):420-7. doi: 10.1080/10401334.2014.945027. PubMed PMID: 25318040.
▪ Chen HC, van den Broek WE, ten Cate O. The case for use of entrustable professional activities in undergraduate medical education. Acad Med. 2015 Apr;90(4):431-6. doi: 10.1097/ACM.0000000000000586. PubMed PMID: 25470310.
▪ Elnicki, et al for the CDIM/Association of Program Directors in Internal Medicine Committee on Transition to Internship. Course Offerings in the Fourth Year of Medical School: How U.S. Medical Schools Are Preparing Students for Internship. Academic Medicine 2015.
▪ Lyss-Lerman P, Teherani A, Aagaard E, Loeser H, Cooke M, Harper GM. What training is needed in the fourth year of medical school? Views of residency program directors. Acad Med. 2009 Jul;84(7):823-9. doi: 10.1097/ACM.0b013e3181a82426. PubMed PMID: 19550170.
▪ Chen HC, van den Broek WE, ten Cate O. The case for use of entrustable professional activities in undergraduate medical education. Acad Med. 2015 Apr;90(4):431-6. doi: 10.1097/ACM.0000000000000586. PubMed PMID: 25470310.

References▪ Abramson, S. B., Jacob, D., & Rosenfeld, M. A 3-year MD—accelerating careers, diminishing debt.
New England Journal of Medicine. Sep 19, 2013▪ Raymond, J. R., Sr, Kerschner, J. E., Hueston, W. J., & Maurana, C. A. (2015). The Merits and
Challenges of Three-Year Medical School Curricula. Academic Medicine, 90(10), 1318–1323. ▪ Bell HS1, Ferretti SM, Ortoski RA. “A three-year accelerated medical school curriculum designed to
encourage and facilitate primary care careers.” Acad Med. 2007 Sep;82(9):895-9.▪ Lockyer J1, Violato C, Wright B, Fidler H, Chan R.. “Long-term outcomes for surgeons from 3- and 4-
year medical school curricula.” Can J Surg. 2012 Aug;55(4):S163-70. doi: 10.1503/cjs.37610. http://www.ncbi.nlm.nih.gov/pubmed/22854154
▪ Lockyer JM1, Violato C, Wright BJ, Fidler HM. “An analysis of long-term outcomes of the impact of curriculum: a comparison of the three- and four-year medical school curricula.” Acad Med. 2009 Oct;84(10):1342-7. doi: 10.1097/ACM.0b013e3181b6c08e.
▪ https://www.aamc.org/download/426260/data/physiciansupplyanddemandthrough2025keyfindings.pdf
▪ http://repository.countway.harvard.edu/xmlui/handle/10473/1784?show=full▪ http://uscode.house.gov/statutes/pl/92/157.pdf▪ https://www.washingtonpost.com/national/health-science/medical-school-done-faster/2014/01/13/4b6
d9e54-5c40-11e3-be07-006c776266ed_story.html
70

Thank You
Recommended