THE OPIOID EPIDEMIC & IMPORTANCE OF
TOXICOLOGY TESTING
Dr. Patrick Rainey, Chief Operating Officer
Dr. Zhiyi Qiang, Director of Advanced Clinical technology
Select Laboratory Partners


http://www.cnbc.com/2016/04/27/americans-consume-almost-all-of-the-global-opioid-supply.html

http://www.nytimes.com/interactive/2016/01/07/us/drug-overdose-deaths-in-the-us.html?_r=0
Where can it be used?
• Pain Management• Primary Care• Psychiatry• Substance Abuse Monitoring (Rehab)
Benefits of use:• Identify substance use that affects medical decisions• Identify potential adulteration or adverse drug interactions• Identify illicits or nonprescription drugs• Medication compliance/diversion• Abstinence monitoring• Fetal & neonate risk assessment
UTILIZING DRUG TESTING IN CLINICAL PRACTICE
• Employment drug screening• DUI• Newborn screening• Forensics

Negative for Any Drug (Including Prescribed Drug, 25%
Negative for Prescribed Drug and
Positive for Other Drug,
15%
Positive for Prescribed Drug and Positive for
Other Drug, 20%
Positive for Prescribed Drug and
Negative for Other Drug,
40%
Percentage of UDT Positives and Negatives (Quest Diagnostics, 2012, n=151,405)
Pain Clinic Studies of UDT
http://www.cesar.umd.edu/cesar/cesarfax/vol22/22-22.pdfhttp://ccoe.rbhs.rutgers.edu/online/ARCHIVE/endurings/09MC07.pdf
Screen – Determines presence or absence of a drug (Qualitative).
Immunoassay – a biochemical test that measures the presence and concentration of a drug through the use of an antibody/antigen binding model (typically only semi-quantitative).
Confirmation – Determines presence or absence of a drug, the identity of the drug and the amount of the drug present (Quantitative).
A Few Definitions…
Cup Screening
Typically performed in physician office
Rapid results, but only qualitative (positive or negative) & drug class
False positives and negatives are typical
Depending on patient risk stratification, sample is sent for further testing
Immunoassay for rapid qualitative detection
High throughput
Cutoffs for detection high relative to LCMS or GCMS confirmation
Biggest issue - Low Specificity, both false positives and negatives
Theory based on human immune system: Drug is antigen; antibody in solution binds to drug and is detected.
Immunoassay Testing
Johnson-Davis KL et al. J Anal Toxicol. 2016; 40(2):97-107
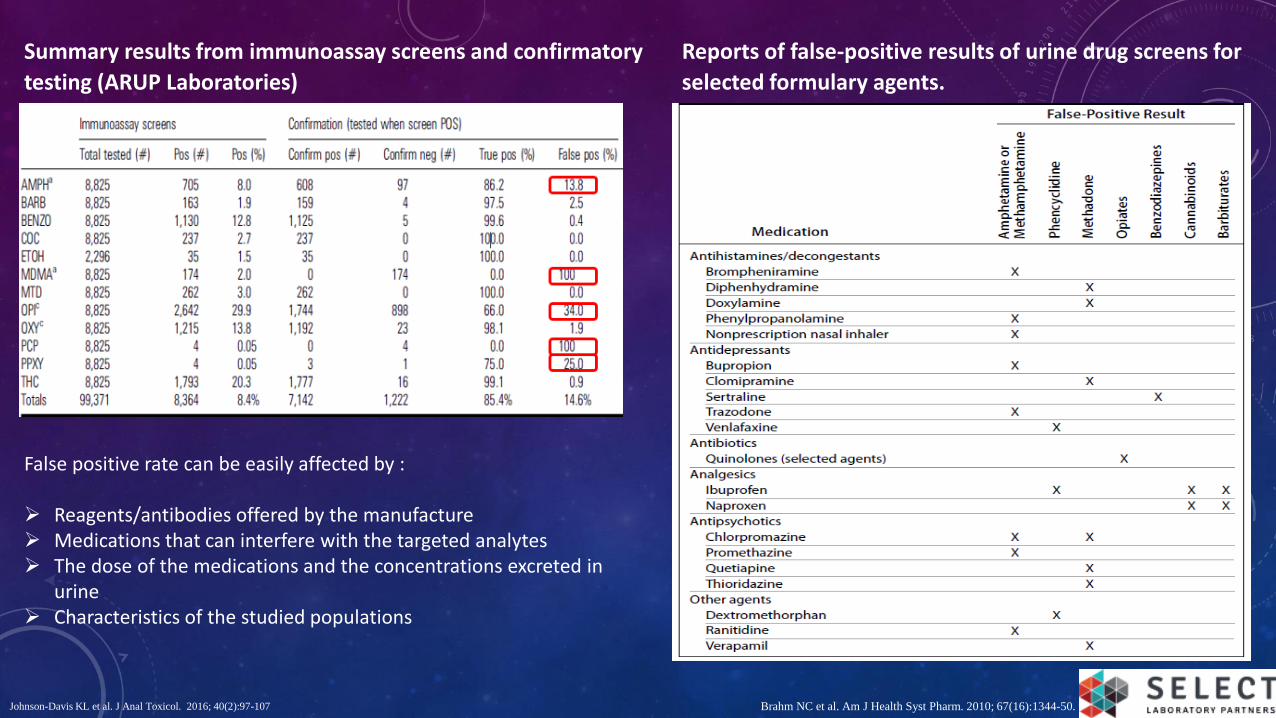
Summary results from immunoassay screens and confirmatory
testing (ARUP Laboratories)
False positive rate can be easily affected by :
Reagents/antibodies offered by the manufacture Medications that can interfere with the targeted analytes The dose of the medications and the concentrations excreted in
urine Characteristics of the studied populations
Reports of false-positive results of urine drug screens for
selected formulary agents.
Brahm NC et al. Am J Health Syst Pharm. 2010; 67(16):1344-50.
Now most common MS technique used
Specific & Quantitative over wide dynamic range
Large test menu
Metabolite confirmation
LC-MS/MS Confirmation

MS PLATFORM COMPARISONS
M. Sargent (Ed.), Guide to achieving reliable quantitative LC-MS measurements, RSC Analytical Methods Committee, 2013. ISBN 978-0-948926-27-3.
QQQ Ion Trap TOF qTOF
Selectivity High High High High
Sensitivity High High Lower Lower
Matrix considerations (sample prep)
Minimum More More More
Duty Cycle (speed) Fast Slower Moderate Moderate
Dynamic Range High Lower Lower Lower
The available MS platforms all have unique benefits for specific purposes. The comparisonsin the table are with regard to drug confirmations in urine or oral fluids.
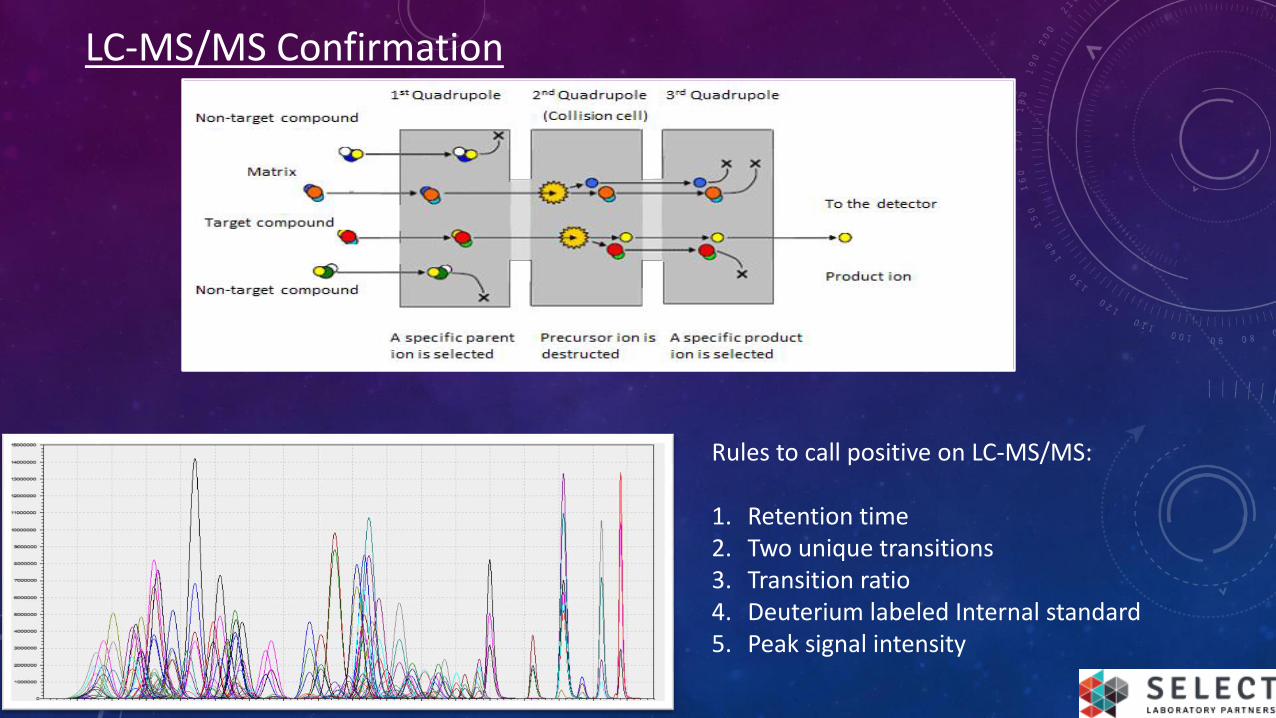
LC-MS/MS Confirmation
Rules to call positive on LC-MS/MS:
1. Retention time2. Two unique transitions3. Transition ratio4. Deuterium labeled Internal standard5. Peak signal intensity
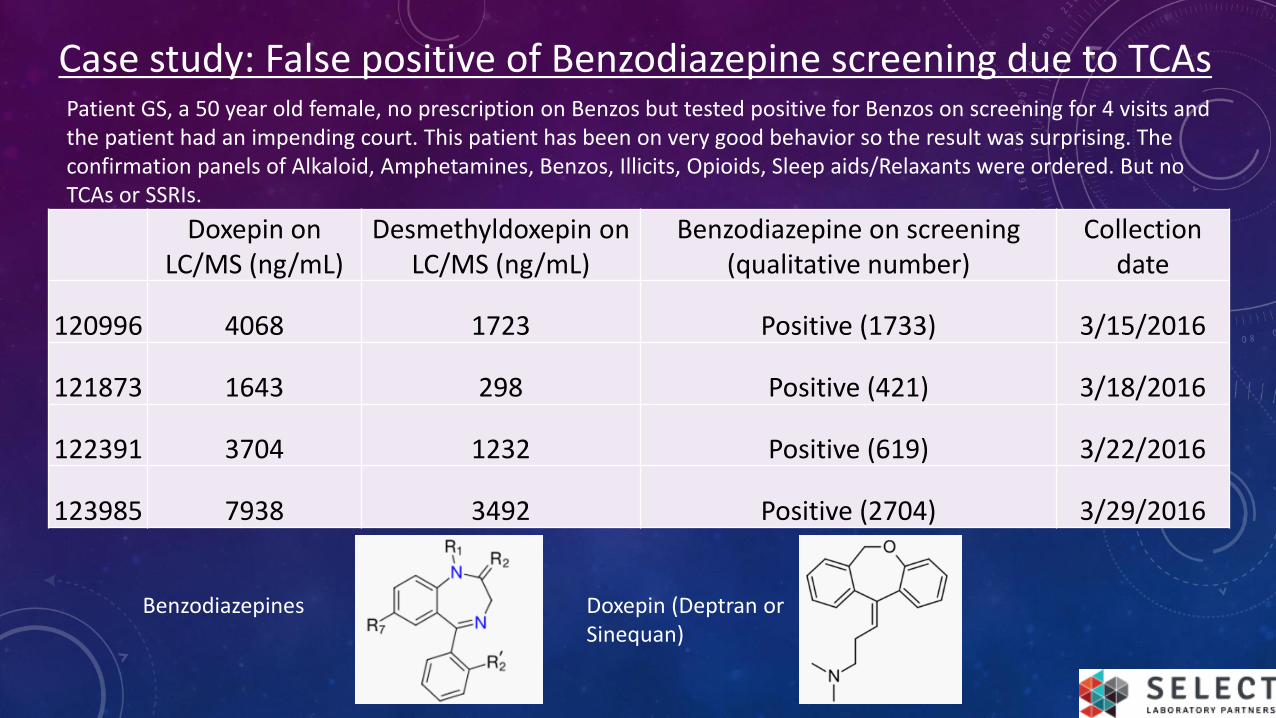
Doxepin on LC/MS (ng/mL)
Desmethyldoxepin on LC/MS (ng/mL)
Benzodiazepine on screening (qualitative number)
Collection date
120996 4068 1723 Positive (1733) 3/15/2016
121873 1643 298 Positive (421) 3/18/2016
122391 3704 1232 Positive (619) 3/22/2016
123985 7938 3492 Positive (2704) 3/29/2016
Case study: False positive of Benzodiazepine screening due to TCAs
Doxepin (Deptran or Sinequan)
Benzodiazepines
Patient GS, a 50 year old female, no prescription on Benzos but tested positive for Benzos on screening for 4 visits and the patient had an impending court. This patient has been on very good behavior so the result was surprising. The confirmation panels of Alkaloid, Amphetamines, Benzos, Illicits, Opioids, Sleep aids/Relaxants were ordered. But no TCAs or SSRIs.
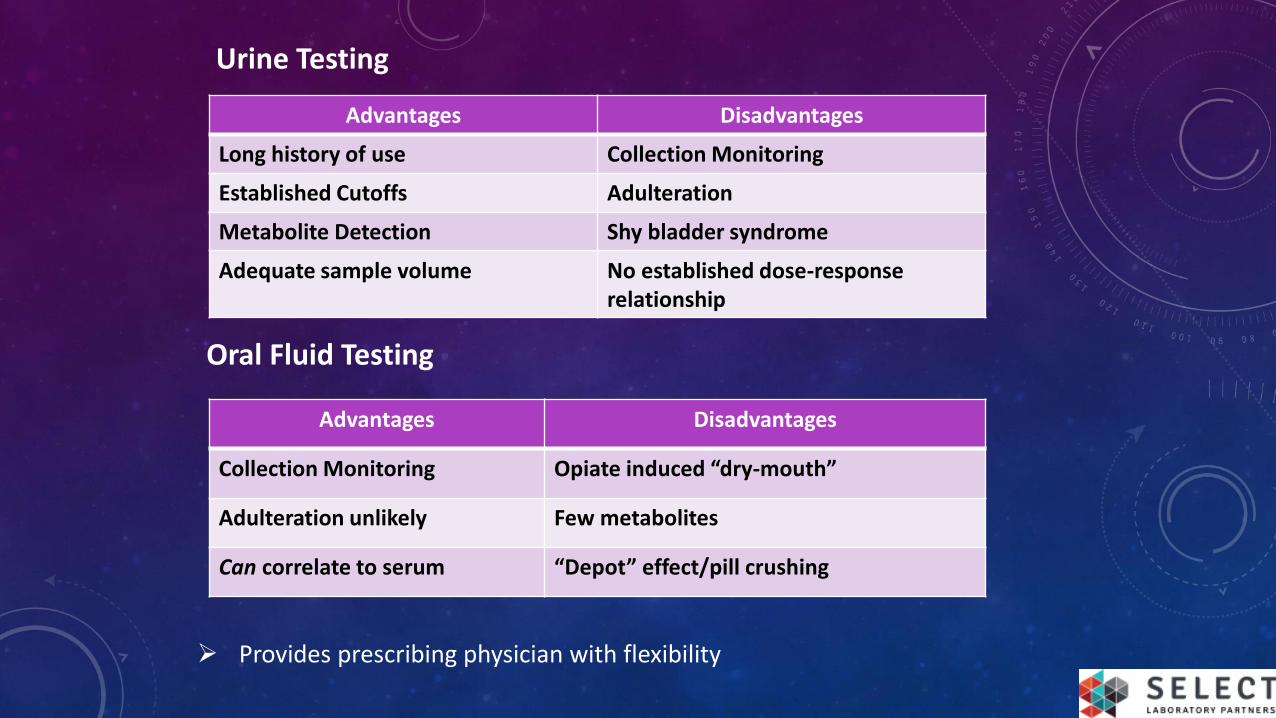
Urine Testing
Advantages Disadvantages
Long history of use Collection Monitoring
Established Cutoffs Adulteration
Metabolite Detection Shy bladder syndrome
Adequate sample volume No established dose-responserelationship
Oral Fluid Testing
Advantages Disadvantages
Collection Monitoring Opiate induced “dry-mouth”
Adulteration unlikely Few metabolites
Can correlate to serum “Depot” effect/pill crushing
Provides prescribing physician with flexibility
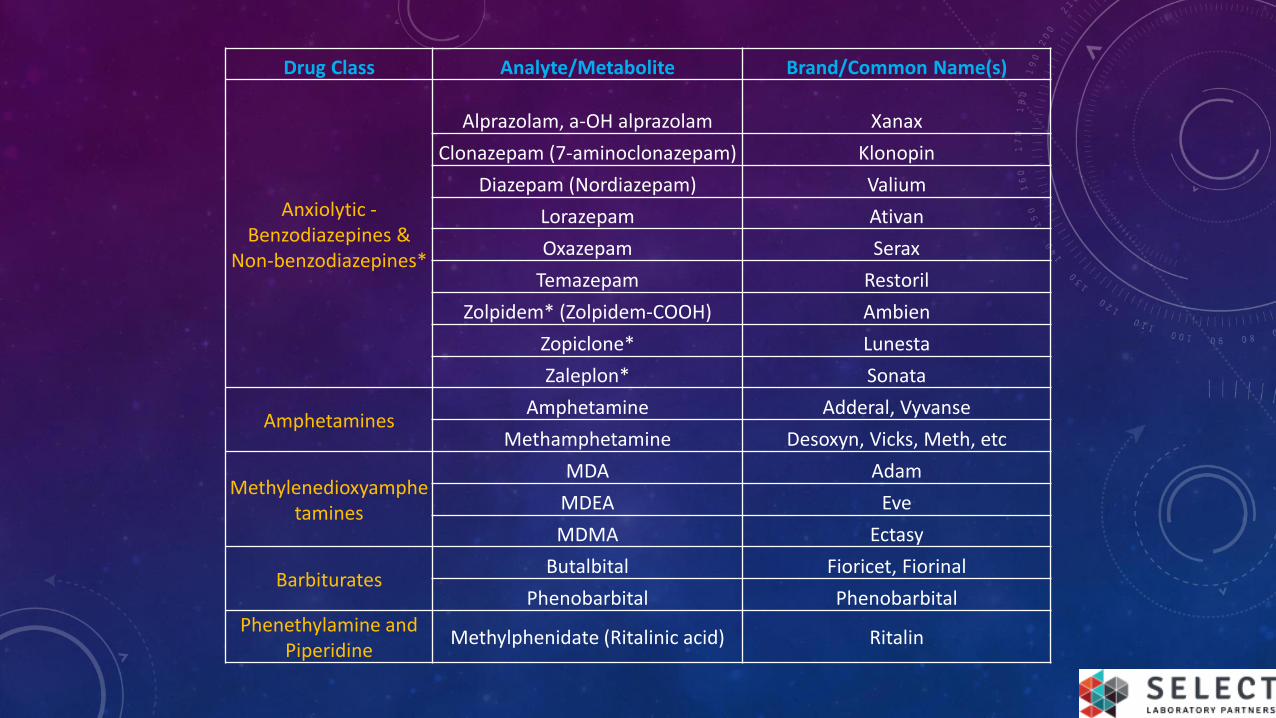
Drug Class Analyte/Metabolite Brand/Common Name(s)
Anxiolytic -Benzodiazepines &
Non-benzodiazepines*
Alprazolam, a-OH alprazolam Xanax
Clonazepam (7-aminoclonazepam) Klonopin
Diazepam (Nordiazepam) Valium
Lorazepam Ativan
Oxazepam Serax
Temazepam Restoril
Zolpidem* (Zolpidem-COOH) Ambien
Zopiclone* Lunesta
Zaleplon* Sonata
AmphetaminesAmphetamine Adderal, Vyvanse
Methamphetamine Desoxyn, Vicks, Meth, etc
Methylenedioxyamphetamines
MDA Adam
MDEA Eve
MDMA Ectasy
BarbituratesButalbital Fioricet, Fiorinal
Phenobarbital Phenobarbital
Phenethylamine and Piperidine
Methylphenidate (Ritalinic acid) Ritalin
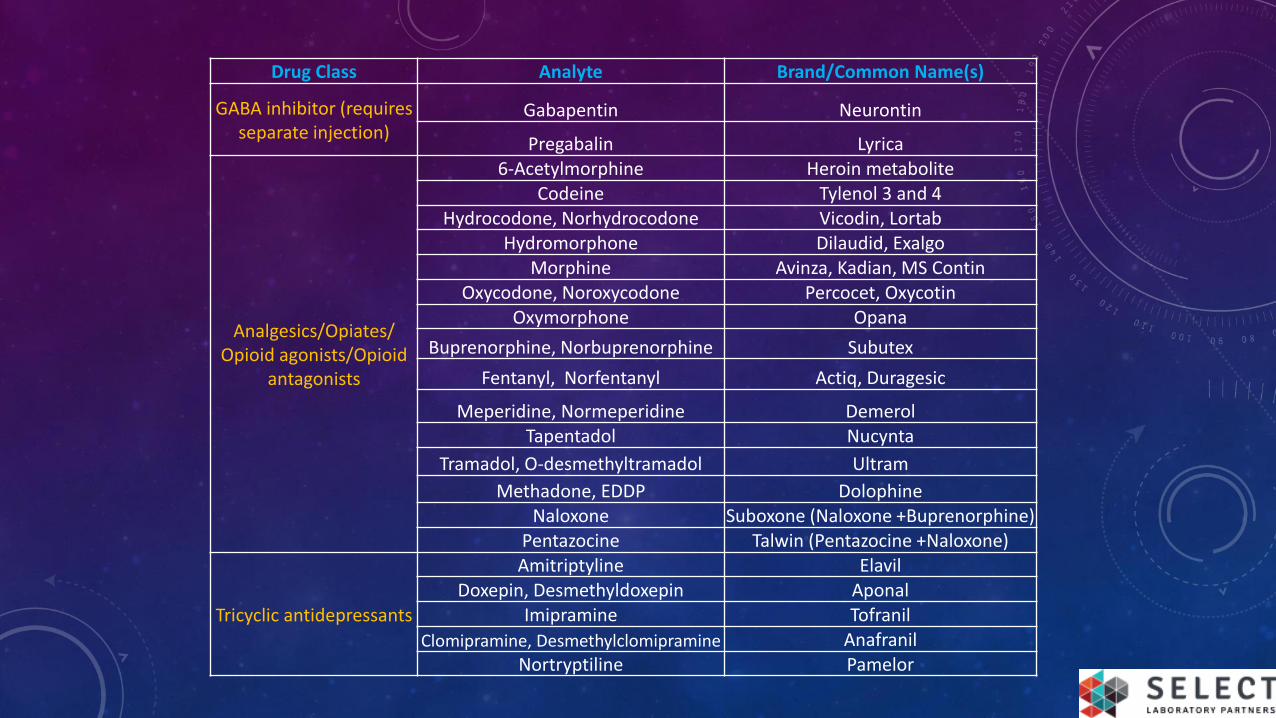
Drug Class Analyte Brand/Common Name(s)
GABA inhibitor (requires separate injection)
Gabapentin Neurontin
Pregabalin Lyrica
Analgesics/Opiates/ Opioid agonists/Opioid
antagonists
6-Acetylmorphine Heroin metaboliteCodeine Tylenol 3 and 4
Hydrocodone, Norhydrocodone Vicodin, LortabHydromorphone Dilaudid, Exalgo
Morphine Avinza, Kadian, MS ContinOxycodone, Noroxycodone Percocet, Oxycotin
Oxymorphone Opana
Buprenorphine, Norbuprenorphine Subutex
Fentanyl, Norfentanyl Actiq, Duragesic
Meperidine, Normeperidine DemerolTapentadol Nucynta
Tramadol, O-desmethyltramadol Ultram
Methadone, EDDP DolophineNaloxone Suboxone (Naloxone +Buprenorphine)
Pentazocine Talwin (Pentazocine +Naloxone)
Tricyclic antidepressants
Amitriptyline ElavilDoxepin, Desmethyldoxepin Aponal
Imipramine Tofranil
Clomipramine, Desmethylclomipramine AnafranilNortryptiline Pamelor
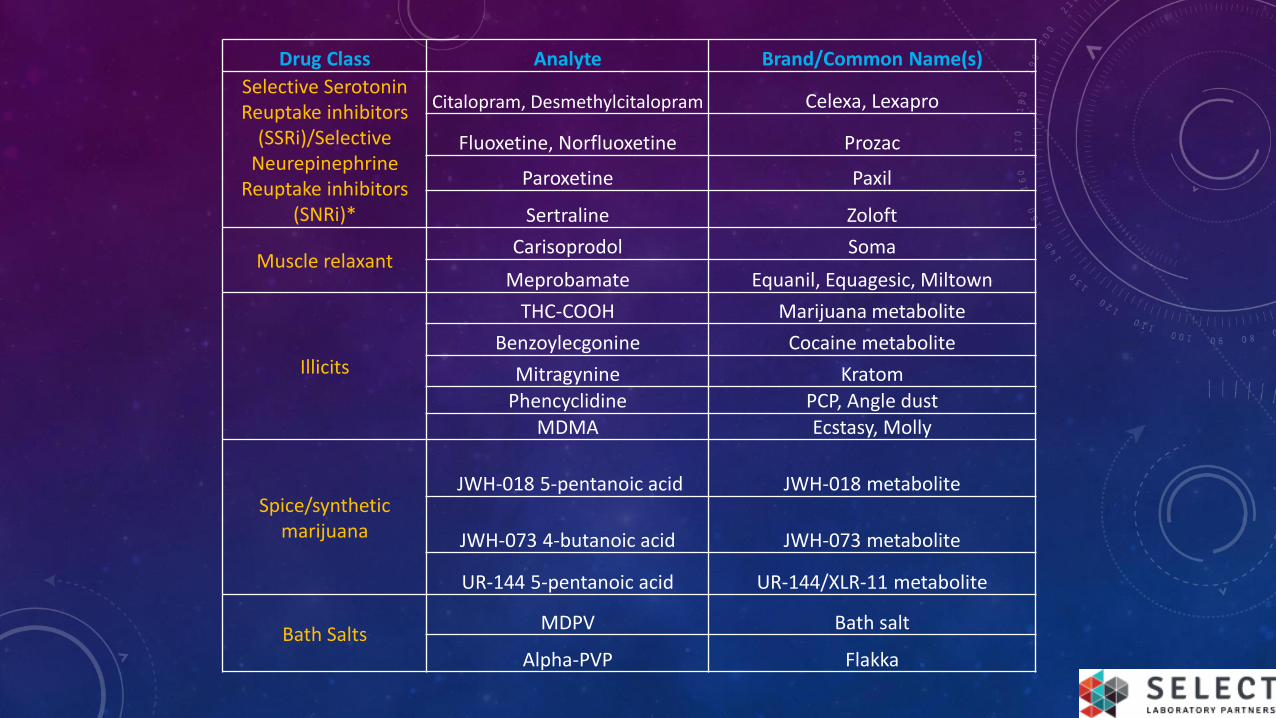
Drug Class Analyte Brand/Common Name(s)
Selective Serotonin Reuptake inhibitors
(SSRi)/Selective Neurepinephrine
Reuptake inhibitors (SNRi)*
Citalopram, Desmethylcitalopram Celexa, Lexapro
Fluoxetine, Norfluoxetine Prozac
Paroxetine Paxil
Sertraline Zoloft
Muscle relaxantCarisoprodol Soma
Meprobamate Equanil, Equagesic, Miltown
Illicits
THC-COOH Marijuana metabolite
Benzoylecgonine Cocaine metabolite
Mitragynine Kratom
Phencyclidine PCP, Angle dustMDMA Ecstasy, Molly
Spice/synthetic marijuana
JWH-018 5-pentanoic acid JWH-018 metabolite
JWH-073 4-butanoic acid JWH-073 metabolite
UR-144 5-pentanoic acid UR-144/XLR-11 metabolite
Bath SaltsMDPV Bath salt
Alpha-PVP Flakka

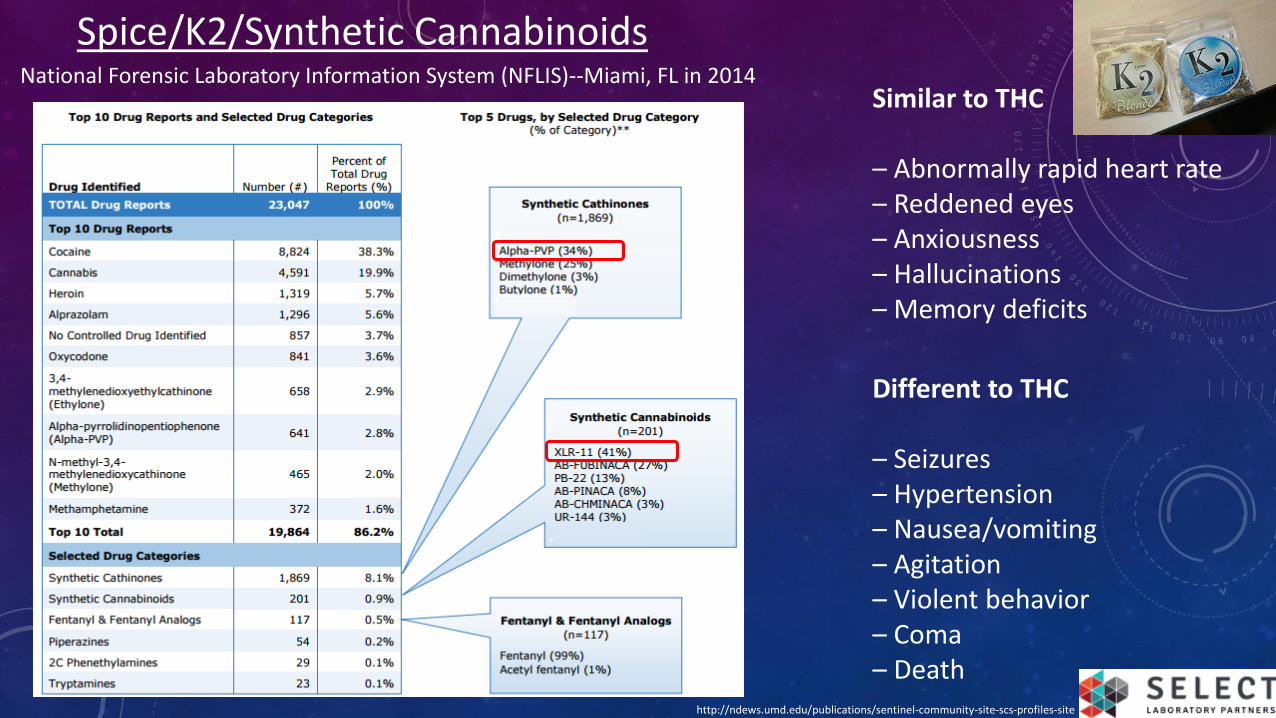
Spice/K2/Synthetic Cannabinoids
Different to THC
– Seizures– Hypertension– Nausea/vomiting– Agitation– Violent behavior– Coma– Death
Similar to THC
– Abnormally rapid heart rate– Reddened eyes– Anxiousness– Hallucinations– Memory deficits
National Forensic Laboratory Information System (NFLIS)--Miami, FL in 2014
http://ndews.umd.edu/publications/sentinel-community-site-scs-profiles-site
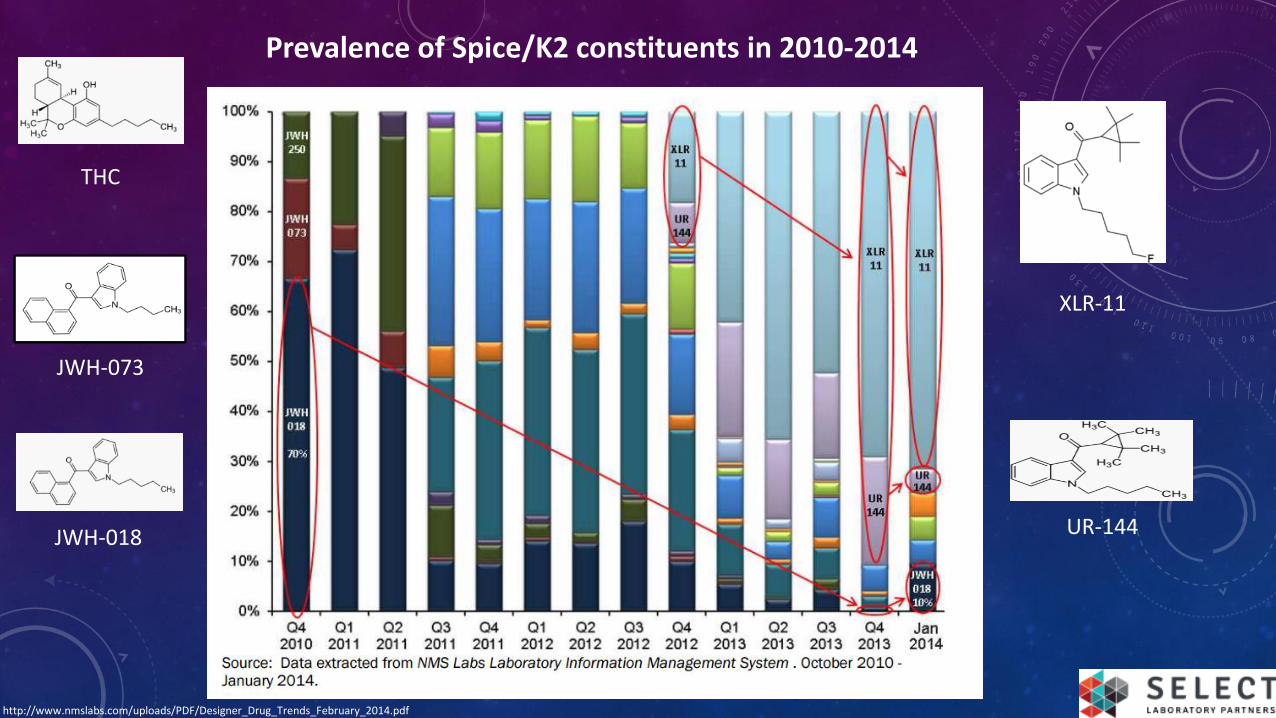
JWH-073
JWH-018
THC
UR-144
XLR-11
Prevalence of Spice/K2 constituents in 2010-2014
http://www.nmslabs.com/uploads/PDF/Designer_Drug_Trends_February_2014.pdf
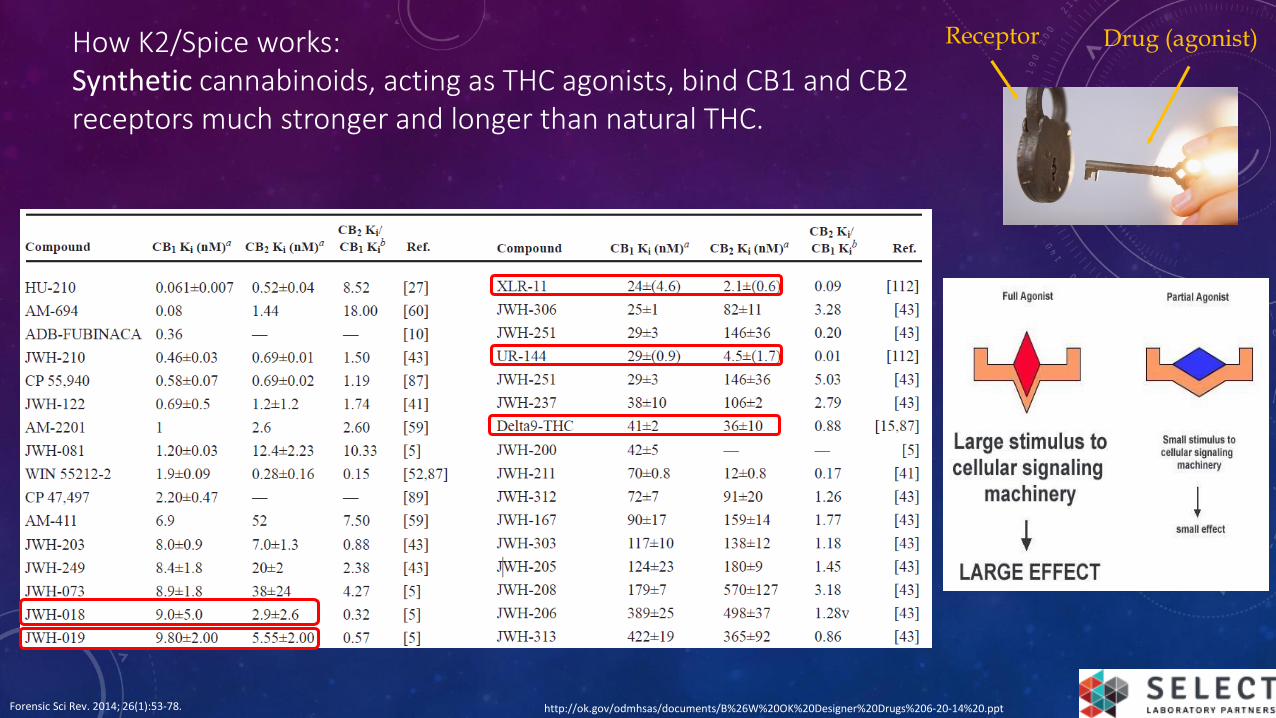
How K2/Spice works:Synthetic cannabinoids, acting as THC agonists, bind CB1 and CB2 receptors much stronger and longer than natural THC.
Receptor Drug (agonist)
Forensic Sci Rev. 2014; 26(1):53-78. http://ok.gov/odmhsas/documents/B%26W%20OK%20Designer%20Drugs%206-20-14%20.ppt
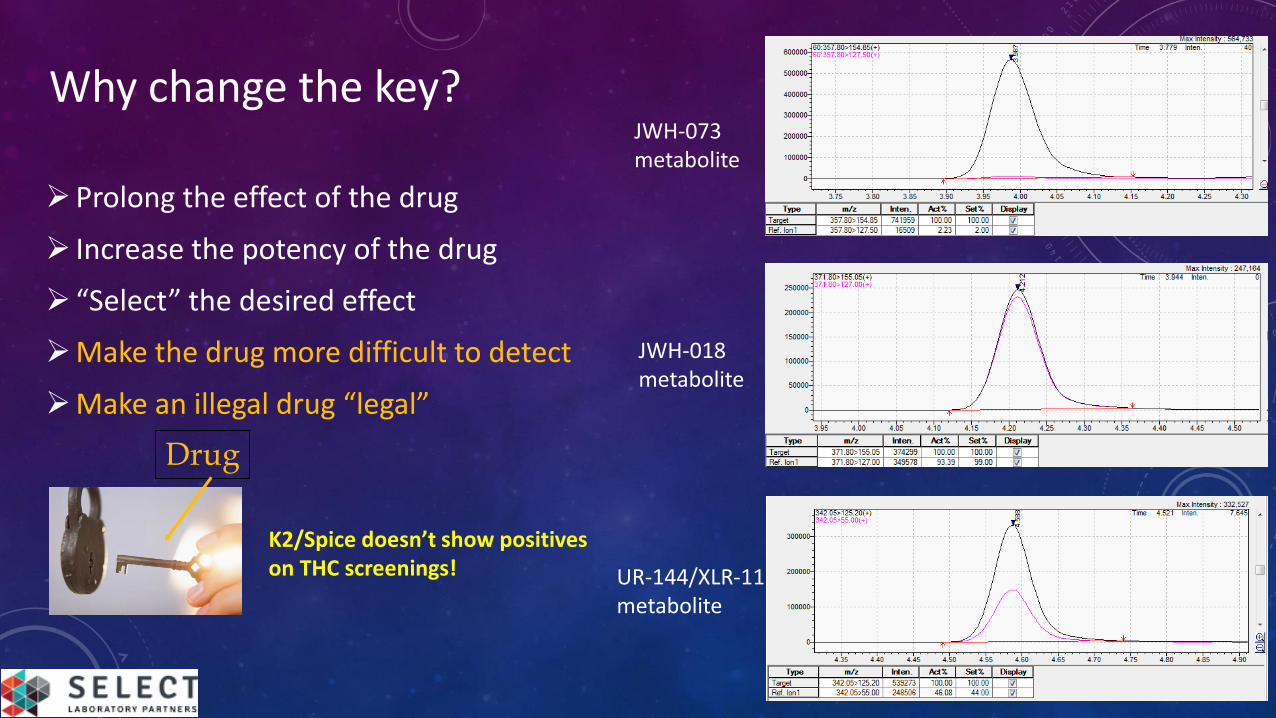
Why change the key?
Prolong the effect of the drug
Increase the potency of the drug
“Select” the desired effect
Make the drug more difficult to detect
Make an illegal drug “legal”
Drug
JWH-073 metabolite
JWH-018 metabolite
UR-144/XLR-11 metabolite
K2/Spice doesn’t show positives on THC screenings!
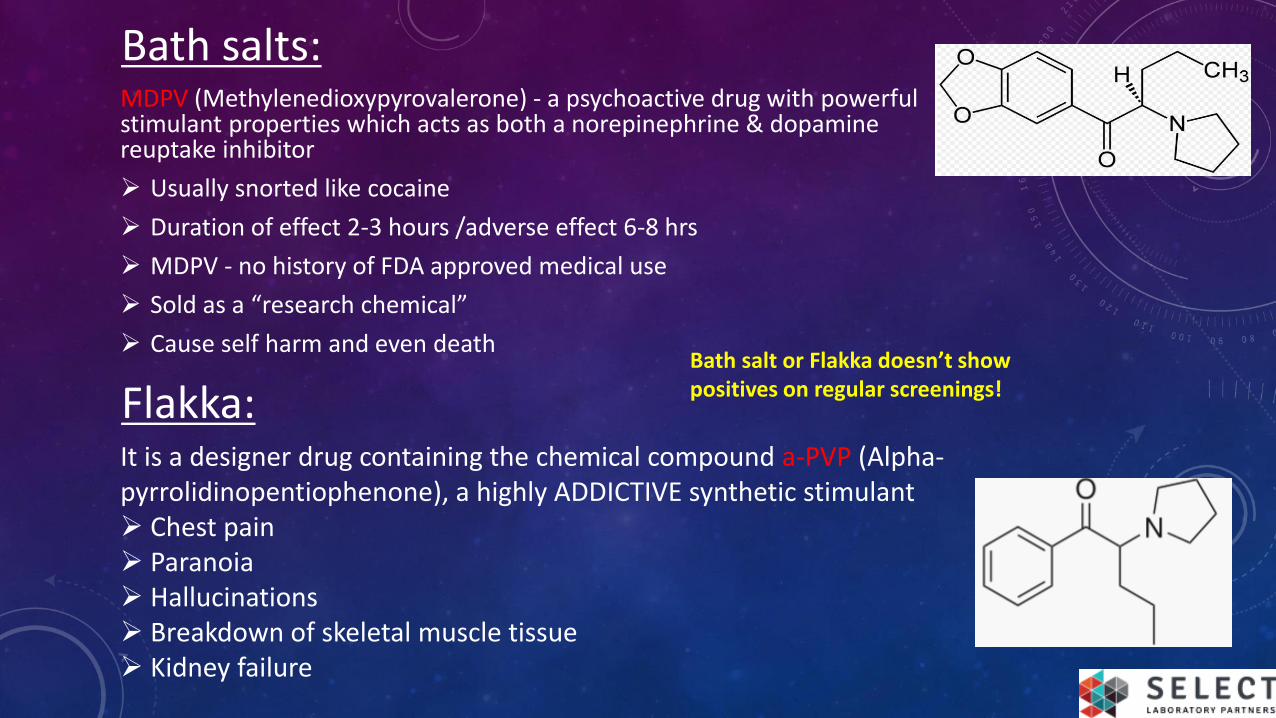
Bath salts:MDPV (Methylenedioxypyrovalerone) - a psychoactive drug with powerful stimulant properties which acts as both a norepinephrine & dopamine reuptake inhibitor
Usually snorted like cocaine
Duration of effect 2-3 hours /adverse effect 6-8 hrs
MDPV - no history of FDA approved medical use
Sold as a “research chemical”
Cause self harm and even death
Flakka:It is a designer drug containing the chemical compound a-PVP (Alpha-pyrrolidinopentiophenone), a highly ADDICTIVE synthetic stimulant Chest pain Paranoia Hallucinations Breakdown of skeletal muscle tissue Kidney failure
Bath salt or Flakka doesn’t show positives on regular screenings!
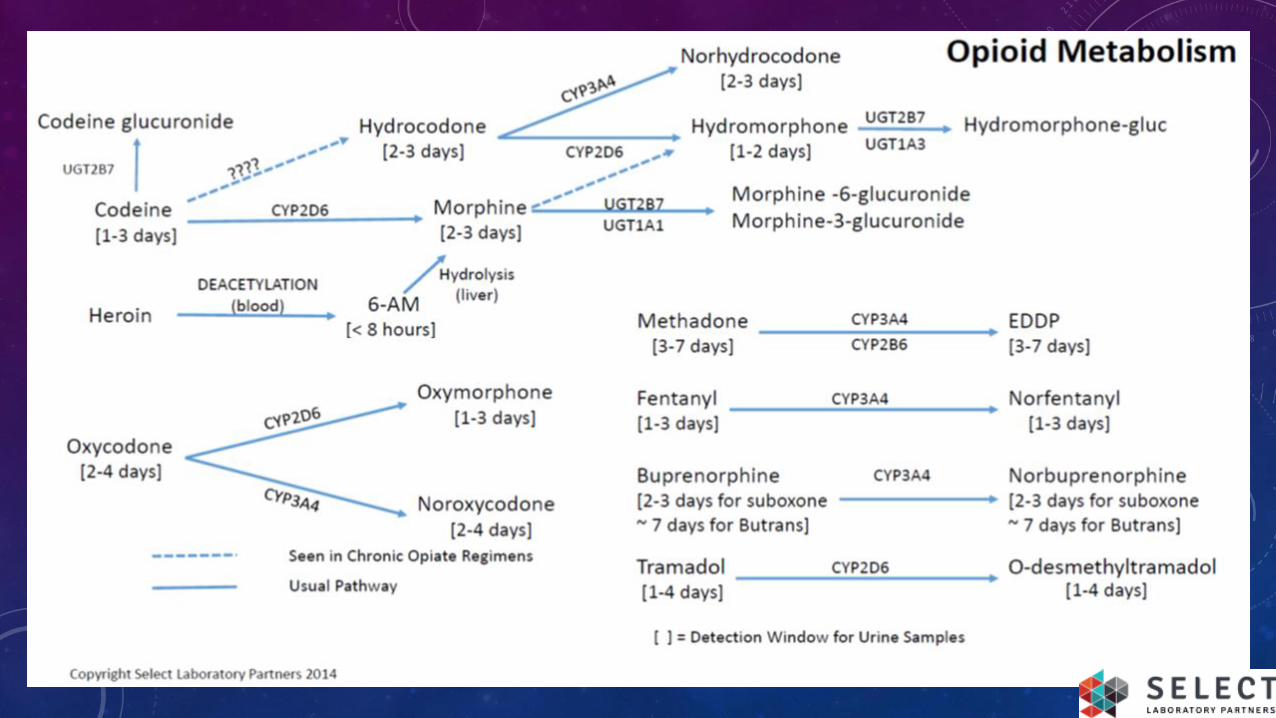
1) In a patient prescribed Tylenol #3, which of the following is expected to be detectable in the urine? (29% correct)
a. Codeineb. Hydrocodonec. Morphined. Hydromorphonee. all of the above
2) In a patient abusing heroin, one would be likely to detect which of the following in the urine? (7% correct)
a. heroinb. 6-AMc. Morphined. b and ce. all of the above
Exam
J Opioid Manag. 2007 Mar-Apr;3(2):80-6.

3) A patient taking Oxycontin is given a urine drug test. He notifies you that he ate a poppy seed muffin for breakfast. What might reasonably be detected in the urine? (22% correct)
a. Oxycodoneb. Codeinec. Morphined. all of the above
4) Which of the following are plausible explanations for a negative urine opiate screen in a patient on chronic opioid therapy? (17% correct)
a. Patient ran out of opioid early and has not used any in a few daysb. Patient is a "fast metabolizer"c. Drug screen does not detect that particular opioidd. a, b and ce. a and c only
THANK YOU!
Recommended

















