The Limits of Scientific Evidence and the Ethics of Dietary Guidelines
Sixty years of AmbiguityPeter Attia, M.D.President, Nutrition Science Initiative
June 20, 2012

2

ObesityObesity
Metabolic diseases
Premature death
Insulin resistance
Type 2 diabetes
Fatty liver disease
Atherosclerosis
Hypertension
Stroke
Cancer
Asthma
Sleep apnea
Osteoarthritis
Neurodegeneration
Gall bladder disease

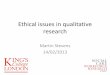
U.S. obesity ratesU.S. obesity rates
197131 million people
2010111 million people
15%
34%

19704.2 million people
201021.1 million
people
U.S. diabetes ratesU.S. diabetes rates
2%
8%

U.S. obesity rates U.S. obesity rates since 1960, by agesince 1960, by agePercent
U.S. consumption of U.S. consumption of food since 1970food since 1970Percent
For men aged 20-74, from National Health and Nutrition Examination Surveys (NHANES)

0
100
200
300
400
500
600
700
800
900
1960 1965 1970 1975 1980 1985 1990 1995 2000 2005 2010
5x5xdifferendifferen
cece
818%
168%
HealthcareHealthcare spendingspending
Economic Economic growthgrowth

Fat and Saturated Fat?
Recommendations
Fat and Saturated Fat?
Recommendations

“Intakes of dietary fatty acids and cholesterol are major determinants of cardiovascular disease (CVD) and Type-2 diabetes (T2D), two major causes of morbidity and mortality in Americans…In order to reduce the population’s burden from CVD and T2D and their risk factors, the preponderance of the evidence indicates beneficial health effects are associated with several changes in consumption of dietary fats and cholesterol. These include limiting saturated fatty acid intake to less than 7 percent of total calories…”
Dietary Guidelines Advisory Committee, 2010

Fat and Saturated Fat?
The Evidence
Fat and Saturated Fat?
The Evidence

“The available evidence from cohort and randomized controlled trials is unsatisfactory and unreliable to make judgment about and substantiate the effects of dietary fat on risk of CHD.”
FAO/WHO Expert Consultation background paper, 2009
Skeaff, Miller, 2009. Annals of Nutrition and Metabolism. Sept. 15: 173-201.

“A meta-analysis of prospective epidemiologic studies showed that there is no significant evidence for concluding that dietary saturated fat is associated with an increased risk of CHD or CVD.”
Siri-Tarino et al. American Journal of Clinical Nutrition, 2010
Siri-tarino et al. 2010. AJCN. Mar; 502-509.

A History Lesson1951-1961
A History Lesson1951-1961

19511951
Ancel Keys and his wife Margaret visit Naples, Italy. They assess the cholesterol and fat content of the diet among workers (no heart disease) and the wealthy (heart disease). Margaret Keys measures cholesterol levels.

19521952Keys presents his hypothesis at a WHO meeting in Amsterdam: “fatty diet, raised serum cholesterol, atherosclerosis, myocardial infarction.”

1961 1961 The American Heart Association
A 4-page AHA report from an ad-hoc committee that now includes Keys concludes that “the best scientific evidence of the time” strongly suggests that Americans would reduce their risk of heart disease by reducing the fat in their diets, and replacing saturated fats with polyunsaturated fats.

1961 1961 The Press
Keys tells Time that the ideal heart-healthy diet should be almost 70% carbohydrate and only 15% fat.

The competing philosophies
Proponents
The competing philosophies
Proponents

“We don’t have the luxury of
time to find the truth before
making policy…”
--The McGovern Report

The competing philosophies
Opponents/skeptics
The competing philosophies
Opponents/skeptics

Without definitive evidence, we don’t know if we’re
right.

Selection biasSelection bias1957-19701957-1970
Each new research adds detail, reduces areas of uncertainty, and, so far, provides further reason to believe.
Ancel Keys, 1957
Keys, 1957. JAMA. Aug. 24:1912-1919

Framingham Heart Study Framingham Heart Study
Positive data: Framingham “links” cholesterol to heart disease.
Negative data: In women over 50 “cholesterol had no predictive value.”
Kannel et al. Ann Int Med. Jan;74(1):1-12.

Framingham Heart Study Framingham Heart Study
[Unpublished] negative data: Framingham compares the diets of men with cholesterol over 300 to those of men with cholesterol under 170 and finds no association with the amount or type of fat consumed.
Kannel, W.B., and T. Gordon. 1968. The Framingham Diet Study: Diet and Regulation of Serum Cholesterol. Section 24 of The Framingham Study. An Epidemiological Investigation of Cardiovascular Disease. Bethesda, MD: U.S. Department of Health, Education, and Welfare, Public Health Service, and National Institutes of Health.

Framingham Heart Study Framingham Heart Study
“There is considerable range of serum cholesterol within the Framingham Study Group. Something explains this inter-individual variation, but it is not diet (as measured here).”
Kannel, W.B., and T. Gordon. 1968. The Framingham Diet Study: Diet and Regulation of Serum Cholesterol. Section 24 of The Framingham Study. An Epidemiological Investigation of Cardiovascular Disease. Bethesda, MD: U.S. Department of Health, Education, and Welfare, Public Health Service, and National Institutes of Health.

More negative evidence More negative evidence
Studies of Benedictine and Trappist monks, Navajo Indians, Irish immigrants to Boston, Swiss Alpine farmers and Maasai and other African pastoralists report no association of saturated fat to heart disease.
Keys rejects them as having “no relevance to diet-cholesterol-CHD relationships in other populations.”
Groen et al. 1962. AJCN. Jun:456-70., Page et al. 1956. Circulation. May: 675-9. , Trulson et al. 1964. JADA. 225-9. , Mann et al. 1964. J Atherosclerosis Res. Jul-Aug: 289-312, Keys. 1975. Atherosclerosis, Sep-Oct;22(2):149-92.

Selection biasSelection biasRevisitRevisit

19571957
Oglesby Paul and colleagues study 5,400 male employees of the Western Electric Company.
They compare the 15 percent of men who reported eating the fattest diets to the 15 percent who reported eating the leanest.
“Worthy of comment, is the fact that of the 88 coronary cases, 14 have appeared in the high-fat intake group and 16 in the low-fat group.”

19811981
Shekelle, Stamler et al. return to Western Electric
They compare heart disease morbidity and mortality to the fat content of the diet in 1957.
“The amount of saturated fatty acids in the diet was not significantly associated with the risk of death from CHD.”

19811981
Shekelle, Stamler et al. rationalize:
“Although most attempts to document the relation of dietary cholesterol, saturated fatty acids, and polyunsaturated fatty acids to serum cholesterol concentration in persons who are eating freely have been unsuccessful, positive results have been obtained in [four] investigations besides the Western Electric Study.”

19811981
Shekelle, Stamler et al. rationalize further:
“If viewed in isolation, the conclusions that can be drawn from a single epidemiologic study are limited. Within the context of the total literature, however, the present observations support the conclusion that the [fat] composition of the diet affects the level of serum cholesterol and the long-term risk of death from CHD in middle-aged American men.”

19811981
Enter the media...
Washington PostWashington Post“The new report strongly reinforces the view that a high-fat, high-cholesterol diet can clog arteries and cause heart disease.”
Shekelle in the New York TimesNew York Times“The message of these findings is that it is prudent to decrease the amount of saturated fats and cholesterol in your diet.”

19901990
The denouement...
The AHA and NHLBI co-author a report called
“The Cholesterol Facts.”
The Western Electric study is included as one of seven “epidemiologic studies showing the link between diet and CHD [that] have produced particularly impressive results” and “showing a correlation between saturated fatty acids and CHD” -- precisely what it did not do.

State of the EvidenceThe 1970s
State of the EvidenceThe 1970s

19701970An American Heart Association committee recommends low-saturated-fat diets (less than 10% of calories) for every American, including “infants, children, adolescents, lactating and pregnant women, and older persons.”
Inter-Society Commission for Heart Disease Resources. 1970. Circulation. July;A55-95.

1975 1975 “Two strikingly polar attitudes persist on this subject, with much talk from each and little listening between.”--Henry Blackburn, New England Journal of
Medicine
1978 1978 “It must still be admitted that the diet-heart relation is an unproved hypothesis that needs much more investigation.”--Thomas Dawber, New England Journal of
Medicine
Blackburn, 1975. NEJM. Jan 9; 105-7., Dawber, 1978. NEJM. Aug 31; 452-8.

Clinical TrialsPre-1977
Clinical TrialsPre-1977

Low-fat diets? Low-fat diets?
1963Hungarian researchers report a benefit of consuming a maximum of 1.5 ounce of fat per day.
1965 British researchers report no benefit of consuming a maximum of 1.5 ounces of fat per day: “A low-fat diet has no place in the treatment of myocardial infarction.”
Korányi, 1963. Ther Hung. 11:17, Research Committee, 1965. Lancet. Sep 11; 501-4.

Cholesterol-lowering diets? Cholesterol-lowering diets?
1973* Minnesota Coronary Study
9,000 men and women: 269 deaths in intervention [low SF,
cholesterol] group. 206 deaths in control group.
*Results go unpublished for 16 years. Why? “We were disappointed in the way they
turned out.” (Frantz)
Frantz et al, 1989. Arteriosclerosis. Jan-Feb; 129-35.

The Tipping PointJanuary,1977
The Tipping PointJanuary,1977

Recommendation Recommendation #I#I
Increase carbohydrate consumption
to 55 to 60% of calories
Recommendation Recommendation #2#2
Reduce fat consumption to 30%
of calories

The Fallback Position? The Fallback Position? The Precautionary Principle
“The question to be asked is not why should we
change our diet but why not? There are [no risks]
that can be identified and important benefits can be
expected.”
--Mark Hegsted, Harvard, at the press conference

Cohort Studies1977-1984
Cohort Studies1977-1984

Total cholesterol does Total cholesterol does not predict future heart not predict future heart
diseasedisease
High LDL is a “marginal risk factor”
Low HDL is a 4-fold better predictor of risk than LDL and the only reliable predictor of risk for men or women
over 50.
Caveats: Saturated fat raises HDL. Carbohydrates lower HDL.
Castelli et al, 1977. Circulation. May; 767-72., Gordon et al, 1977. Am J Med. May;707-14.

19811981Honolulu, Framingham and Puerto
Rico
Saturated fat and total fat negatively associated with risk of heart attack
Saturated fat and total fat positively associated with longevity
Gordon et al, 1981. Circulation. Mar;500-15. Feinleib, 1981. Am J Epi. Jul;5-10. Feinleib,1983. Cancer Res. May; 2503s-2507s.

1981-31981-3
Low serum cholesterol (<160 mg/dl) associated with a higher risk of
cancer.
Observed in every cohort study with 3 exceptions (all Chicago cohorts studied by Jeremiah Stamler)
Gordon et al, 1981. Circulation. Mar;500-15. Feinleib, 1981. Am J Epi. Jul;5-10. Feinleib,1983. Cancer Res. May; 2503s-2507s.

Authors concluded:
Things that raise HDL should be considered to reduce the
risk of CVD
Authors concluded:
Things that raise HDL should be considered to reduce the
risk of CVD

Why ignore HDL and triglycerides for 20
years?
Why ignore HDL and triglycerides for 20
years?

19821982 The Multiple Risk Factor Intervention
Trial (MRFIT)Cost: $115,000,000
7 year mortality: 41.2/1,000 (intervention) vs. 40.4/1,000
(controls)
Wall Street JournalWall Street Journal “Heart attacks, a test collapses.”
MRFIT, 1982. JAMA. Sep 24;1465-77.

January, 1984January, 1984 The Lipid Research Clinics Primary
Prevention TrialCost: $150,000,000
10 year mortality35.8/1,000 (intervention) vs. 37.3/1,000
(controls)
Time Magazine Time Magazine “Sorry, it’s true. Cholesterol really is a
killer.”
LRC Program, 1984. JAMA. Jan 20; 351-64, 365-74.

The authors concludeThe authors conclude“Caution should be exercised before extrapolating the LRCPPT findings to cholesterol lowering drugs other than
bile acid sequestrants.”
“The LRCPPT was not designed to assess directly whether cholesterol lower by
diet prevents CHD.”
LRC Program, 1984. JAMA. Jan 20; 351-64, 365-74.

“It is now indisputable that lowering cholesterol with diet and drugs can actually cut the risk of developing heart disease and having a heart attack.”
--Basil Rifkind, NIH director of the LRCPPT, in Time
LRC Program, 1984. JAMA. Jan 20; 351-64, 365-74.

The Tipping
Point Tips1984
The Tipping
Point Tips1984

The LRC results “strongly indicate that the more you lower cholesterol and fat in your diet, the more you reduce your risk of heart disease.” --Basil Rifkind, NIH director of the LRCPPT,
in Time
LRC Program, 1984. JAMA. Jan 20; 351-64, 365-74.

Why’d they exaggerate?Why’d they exaggerate?
“It’s an imperfect world. The data that would be definitive is ungettable, so you do your best with what is available.”
--Basil Rifkind, 2002
LRC Program, 1984. JAMA. Jan 20; 351-64, 365-74.

In sciences that are based on supposition and opinion, the object is to command assent, not master the thing itself.
--Francis Bacon, Novum Organum, 1620
Consensus BuildingConsensus Building1987 -1989

December, 1984December, 1984 The NIH consensus The NIH consensus
conferenceconference
ConclusionConclusionThere is “no doubt” that a low-fat diet
“will afford significant protection against coronary heart disease” to every
American over the age of two.
Consensus conference, 1985. JAMA. Apr 12;253(14):2080-6.

December, 1984December, 1984 The NIH consensus The NIH consensus
conferenceconference
Caveat Caveat If there had been a true consensus, says Dan Steinberg (chair of the consensus panel, co-PI of LRCPPT), “you wouldn’t
have had to have a consensus conference.”
Consensus conference, 1985. JAMA. Apr 12;253(14):2080-6.

19891989National Academy of National Academy of
Sciences Sciences Diet and Health: Diet and Health: Implications for Reducing Implications for Reducing
Chronic Disease Risk Chronic Disease Risk (1,300 pages)
“Highest priority is given to reducing fat intake, because the scientific evidence concerning dietary fats and other lipids and human health is strongest and the
likely impact on public health the greatest.”
USDHHS 1988.

Evidence, post-consensus1990 - today
Evidence, post-consensus1990 - today

Lifestyle Heart Trial (1990)Lifestyle Heart Trial (1990) 28 patients in treatment arm,
20 patients received no intervention1 year intervention
Treatment: smoking cessation, low-fat (10% max) vegetarian diet, no flour, no sugar, stress management, vigorous
exercise
Treatment group showed a significant reduction in angiographically documented
coronary atherosclerosis
Ornish et al, 1990. Lancet 336:129-133

Meta-Analyses (2001)Meta-Analyses (2001) Cochrane Collaboration: “Reduced or
Modified dietary fat for preventing cardiovascular disease”
27 well-controlled randomized trials10,000 subjects followed for an average of three
years each.
No effect on longevity. No “significant effect on cardiovascular
events.”
Hooper et al, 2001. Cochrane Database Syst Rev. (3):CD002137

Meta-Analyses (2006)Meta-Analyses (2006) Cochrane Collaboration: “Multiple risk
factor interventions for primary prevention for coronary heart disease”
Multiple interventions include lowering blood pressure and cholesterol10 well-
controlled trials900,000 patient years of observation
“The pooled effects suggest multiple risk factor intervention has no effect on
mortality.”
Ebrahim et al. 2006. Cochrane Database Syst Rev. Oct 18;CD001561.

Women’s Health Initiative Women’s Health Initiative (2006)(2006)
48,835 post-menopausal women randomized to a low-fat diet or a
control diet
After six years, total fat consumption was reduced by 8.2%; saturated fat
was reduced by 2.9%.
“Modest” increases in fruits, vegetables and whole grains

Women’s Health Initiative Women’s Health Initiative (2006)(2006)
“The intervention did not reduce risk of CHD or stroke.”
“A low-fat dietary pattern did not result in a statistically significant reduction in the
risk of invasive breast cancer...”
“There is no evidence that a low-fat dietary pattern intervention reduces colorectal
cancer risk...”
“A low-fat dietary pattern among generally healthy postmenopausal women showed no
evidence of reducing diabetes risk...”Howard et al. 2006. JAMA. Feb 8:655-666. Prentice et al. 2006. JAMA. Feb
8:629-642. Beresford et al. 2006. JAMA. Feb 8:643-654. Tinker et al. 2008. Arch Int Med.
Jul 28:1500-1511.

Diet trials (2003)Diet trials (2003)Low-carbohydrate/high-fat vs. low-
calorie, low-fat
Foster et al. 2003. NEJM. May 22;2082-90
63 obese
men and women
R
Conventional LOW-FAT, HIGH-CARB diet instruction
Women: 1200-1500 calories/dMen: 1500-1800 calories/d60 % carbs, 25 % fat, 15 %
protein
HIGH-FAT, LOW-CARB diet instruction
First two weeks < 20 g carbs/d
Then gradually increase until stable weight

Diet trials (2003)
Foster et al
Diet trials (2003)
Foster et al
Low carb/conventional low fat
TGs TC
LDL HDL
Foster et al. 2003. NEJM. May 22;2082-90

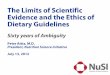
Diet trials (2007)Diet trials (2007)A TO Z TrialA TO Z Trial
Gardner et al. 2007. JAMA. March 7;969-77
2 MONTHS
Group n kcal/d CHO PRO FAT Weight LDL Trig HDL DBP
Atkins 77 1381 ~62g 97 84 -4.3 kg +2.3-52.3-0.4 -2.9
Zone 79 1455 152 87 57 -2.0 kg -5.3 -24.8-0.5 -2.1
LEARN 79 1476 180 73 49 -2.8 kg -7.3 -17.2-3.8 -1.4
Ornish 76 1408 220 60 33 -2.8 kg-10.1-10.9-5.3 -0.4
12 MONTHS
Group n kcal/d CHO PRO FAT WeightLDL Trig HDL DBP
Atkins 77 1599~140g84 78 -4.5 kg+0.8 -29.3+4.9 -4.4
Zone 79 1594 179 80 62 -1.5 kg 0 -4.2 +2.2 -2.1
LEARN 79 1654 194 79 61 -2.5 kg+0.6 -14.6-2.8 -2.2
Ornish 76 1505 195 68 50 -2.4 kg-3.8 -14.9 0 -0.7

Diet trials Diet trials (2008)(2008)
Workplace Diet Workplace Diet TrialTrial
Shai et al. 2008. NEJM. Jul 17;229-41

Diet trials (2008)Diet trials (2008)Workplace Diet Trial
Test Low FatMediterrane
an Low Carb
Systolic BP, mm Hg -4.3 -5.5 -3.9
Diastolic BP, mm Hg -0.9 -2.2 -0.8
LDL-C, mg/dl -0.05 -5.6 -3.0
HDL-C, mg/dl 6.3 6.4 8.4
Triglyceride, mg/dl -2.8 -21.8 -23.7
T Chol : HDL ratio -0.6 -0.9 -1.1
Hemoglobin A1c, % -0.4 -0.5 -0.9
C-reactive protein, mg/l -0.6 -0.9 -1.3
Red denotes p<0.05 for within-group change from baseline. Blue denotes p<0.05 for comparison of Low Carb vs. Low Fat.
Shai et al. 2008. NEJM. Jul 17;229-41

Why the confidence?Pre-1984
Populations with very low cholesterol levels have a low incidence of heart
disease
Why the confidence?Pre-1984
Populations with very low cholesterol levels have a low incidence of heart
disease

Why the confidence?Post-1984
Cholesterol-lowering drugs work (statins, in particular)
Why the confidence?Post-1984
Cholesterol-lowering drugs work (statins, in particular)

Caveat
Drugs and diets are not comparable.
Drugs have multiple actions as do diets.
“Saying that statins reduce heart disease risk by lowering cholesterol, is like saying that aspirin reduces heart disease risk by reducing headaches.”
--Kronmal
Caveat
Drugs and diets are not comparable.
Drugs have multiple actions as do diets.
“Saying that statins reduce heart disease risk by lowering cholesterol, is like saying that aspirin reduces heart disease risk by reducing headaches.”
--Kronmal

President John F. KennedyYale University commencement address June 11, 1962
“For the greatest enemy of truth is very often not the lie – deliberate, contrived and dishonest – but the myth – persistent, persuasive, and unrealistic. Too often we hold fast to the clichés of our forebears. We subject all facts to a prefabricated set of interpretations. We enjoy the comfort of opinion without the discomfort of thought.”
Recommended