The Hip
Differential Diagnosis & Treatment
Mazyad Alotaibi

Capsular Lesions
• Most loss of medial rotation
• Less of flexion and abduction
• Least of extension

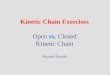
Osteoarthritis
• OA most common joint disorder
• Risk factors – family history, obesity, injury, occupation, elite athletes
• A- joint space narrowing
• B- marginal osteophytes
• C- marginal sclerosis
• D- cystic changes in the head of the acetabulum

Osteoarthritis
• Treatment• Stage 1) heat + slow
stretches into MR, ext, abd and flex
• +hep• Stage 2) steriod injec
+ rest• Stage 3) surgery

Non capsular

Loose Body
• Pain on lat rot with abd or flex with springy end feel
• Twinges of pain
• Refer to surgeon for opinion re: EUA

Contractile lesions

Hamstrings, adductor longus and rectus femoris
• Resisted test painful• Sudden onset –
overstreching• Hams and rec fem due to
combined movts over 2 joints
• Hamstrings• Rectus Femoris• Adductor Longus• Treatment – deep friction
and rest or steriod injec and rest

Bursa

Trochanteric Bursitis
• Resisted hip abd in side lying
• Direct trauma
• Treatment – injec or electrotherapy + rest

Psoas Bursitis
• Test with passive flex 90 degrees and add
• Also resisted hip flex• Overuse • Occasional trauma
• Treatement –injec or electrotherapy + rest

Gluteal Bursitis
• Pain on passive flexion, add and abduction
• Pain on resisted abduction and extension
• Sup and post to trochanter
• Overuse
• Treatment – injec or electrotherapy + rest

Sign of the Buttock
• Indicates possible neoplasm, abcess, fracture, osteomyelitis, sepsis
• Pain on: trunk flexion
passive hip flex with empty end feel
SLR
resisted hip movements

Groin Pain

Groin Pain
• Psoas bursa• Sportsman’s Hernia• OA Hip, perthes disease, loose body• L3• Ref from SIJ• Osteitis pubis• Slipped epiphysis• Gynae/ genito urinary
Recommended